Eggs for Lutein, Zeaxanthin & Eye Health
Lutein and zeaxanthin are two yellow xanthophyll carotenoids out of roughly 600 carotenoids found in nature. They are the only two carotenoids that selectively cross the blood-retinal barrier and accumulate in the macula lutea (Latin for "yellow spot") at the center of the retina, where they form the macular pigment that filters blue light and quenches singlet oxygen at the photoreceptor outer segments. Egg yolk is not the densest source of these carotenoids — spinach and kale contain 10-20× more per gram — but the egg-yolk lipid matrix makes them dramatically more bioavailable. The Chung 2004 trial showed egg-derived lutein produced higher serum responses than equivalent doses from spinach or supplements. The 2013 AREDS2 trial established that lutein and zeaxanthin should replace beta-carotene in the original AREDS formulation for age-related macular degeneration. For most adults concerned about long-term eye health, two eggs per day for 12 weeks measurably raises serum lutein/zeaxanthin and macular pigment optical density.
Table of Contents
- What Are Lutein and Zeaxanthin?
- The Macula Lutea and Macular Pigment Optical Density
- Two Mechanisms: Blue-Light Filter and Antioxidant
- Why Egg-Yolk Bioavailability Beats Spinach
- The AREDS2 Trial and Macular Degeneration
- Egg-Intervention Trials (Wenzel, Kelly, Goodrow)
- Cataract Prevention Evidence
- Blue Light, Screen Use, and MPOD
- Practical Intake — How Many Eggs?
- Cautions and Special Populations
- Key Research Papers
- Connections
- Featured Videos
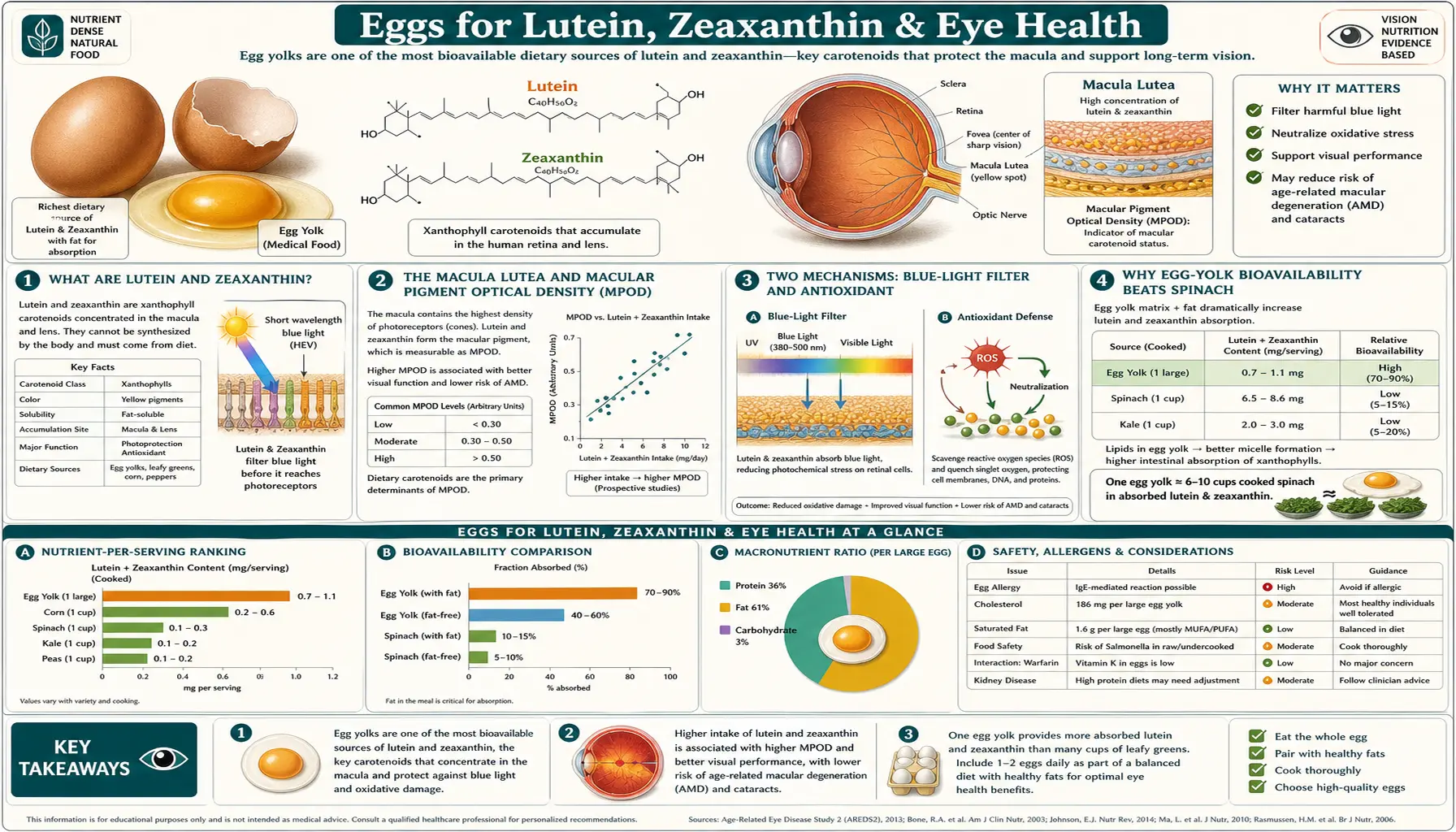
What Are Lutein and Zeaxanthin?
Carotenoids are the family of fat-soluble plant pigments responsible for the yellow, orange, and red colors of carrots, peppers, tomatoes, marigolds, and autumn leaves. Plants synthesize them as accessory photosynthetic pigments and as photoprotectants — the same pigments that absorb excess light energy in the chloroplast to prevent oxidative damage to chlorophyll also work in human tissue to absorb light energy and quench reactive oxygen species. Of the ~600 known carotenoids, only about 20 appear in measurable concentration in human serum, and only two — lutein and zeaxanthin — selectively accumulate in the retina at the back of the eye.
Lutein and zeaxanthin are structural isomers (same molecular formula, different arrangement). Both are xanthophylls, meaning they contain hydroxyl groups that distinguish them from the hydrocarbon carotenes like beta-carotene and lycopene. The hydroxyl groups make them slightly polar, which gives them a different absorption pattern and a different cellular distribution than the pure-hydrocarbon carotenes.
A third closely related carotenoid, meso-zeaxanthin, is found in the human macula but not in most dietary sources. It is produced from lutein by an enzyme in the retinal pigment epithelium (RPE65 family) and concentrates at the very center of the fovea. Meso-zeaxanthin is essentially an internal conversion product, not a dietary nutrient in most populations, though some specialty supplements (including the patented Lutemax 2020 formulation) provide it directly.
In the macula, the three carotenoids segregate spatially: meso-zeaxanthin at the foveal center, zeaxanthin in the surrounding parafovea, and lutein in the peripheral macula. This spatial arrangement is exquisitely conserved across vertebrate retinas and strongly suggests the macular pigment evolved for a specific photoprotective purpose.
The Macula Lutea and Macular Pigment Optical Density
The macula lutea is the 5 mm-diameter central region of the retina that handles high-acuity central vision. It contains the highest density of cone photoreceptors and is the area you use to read, recognize faces, and focus on detail. The macula is anatomically distinguishable from the surrounding retina by its yellow color — the result of accumulated lutein and zeaxanthin in the inner retinal layers anterior to the photoreceptors.
The concentration of macular pigment is measured clinically as macular pigment optical density (MPOD), expressed as the log-base-10 of the ratio of incident to transmitted blue light at the peak absorbance wavelength (460 nm). Higher MPOD means more pigment present, which means more blue-light filtering and more antioxidant capacity. Typical MPOD in healthy adults ranges from 0.2 to 0.6, and the variance is largely driven by dietary intake of lutein and zeaxanthin, smoking history, and obesity status (smoking and obesity both reduce MPOD).
The retina presents MPOD a counterintuitive but elegant arrangement. The yellow macular pigment sits in the inner retinal layers, anterior to the photoreceptors. Light entering the eye must pass through the pigment before reaching the rods and cones that actually detect it. This means the pigment selectively absorbs short-wavelength blue light (the most energetic visible wavelengths, most likely to cause photochemical damage) before the light reaches the vulnerable photoreceptor outer segments. The macula is therefore protected by a built-in optical filter that is preferentially placed exactly where central vision is most concentrated and most metabolically active.
MPOD is measurable with a heterochromatic flicker photometer (HFP), a small clinical device that compares the brightness of a flickering blue/green light at the center of vision (where pigment is dense) versus the parafoveal region (where pigment is minimal). The technique is non-invasive, takes about 10 minutes, and produces a reproducible single number that quantifies an individual's macular pigment status.
Two Mechanisms: Blue-Light Filter and Antioxidant
The macular pigment protects the retina through two distinct biophysical mechanisms.
- Blue-light filtration. Lutein and zeaxanthin have peak absorbance around 460 nm, which is in the short-wavelength visible range that overlaps with the "blue light hazard" wavelengths (415-455 nm). Short-wavelength visible light has the highest photon energy in the visible spectrum and is most likely to produce free radicals when absorbed by retinal pigments. By absorbing this light before it reaches the photoreceptors, the macular pigment reduces the photochemical stress on the most metabolically vulnerable retinal cells. The effect is analogous to wearing yellow-tinted sunglasses internally and permanently.
- Singlet oxygen quenching. When visible light is absorbed by retinal pigments (lipofuscin in the RPE, melanin in the choroid), the absorbed energy occasionally transfers to molecular oxygen to produce singlet oxygen — an extremely reactive oxygen species that initiates lipid peroxidation chains in cell membranes. The macular carotenoids physically quench singlet oxygen, dissipating the energy as heat before it can damage neighboring tissue. This mechanism is biochemically similar to the photoprotective role carotenoids play in plant chloroplasts.
Both mechanisms protect the same vulnerable target: the polyunsaturated fatty acid-rich photoreceptor outer segments, which contain disproportionately high concentrations of docosahexaenoic acid (DHA, 22:6 n-3) and other long-chain omega-3 fatty acids. These fatty acids are essential for photoreceptor function but also highly susceptible to oxidative damage. The combination of high-energy light, high oxygen tension, and high omega-3 content makes the retina one of the most oxidatively stressed tissues in the body, and the macular pigment is the local antioxidant system that protects it.
Why Egg-Yolk Bioavailability Beats Spinach
On a per-gram basis, leafy greens absolutely dominate eggs for lutein and zeaxanthin content. One cup of cooked spinach contains roughly 20 mg of lutein + zeaxanthin. One large egg yolk contains only about 0.25 mg of lutein + zeaxanthin. Spinach is 80× denser by direct measurement.
And yet, the Chung et al. 2004 study published in the Journal of Nutrition delivered a startling result: when adult men were fed equivalent doses of lutein from spinach, lutein supplements, or lutein-enriched eggs (eggs from hens fed marigold petals to boost yolk lutein), serum lutein responses were:
- Spinach: baseline serum lutein response
- Lutein supplement (free crystalline lutein): approximately equal to spinach
- Egg-enriched lutein: approximately 3× greater serum response per unit dose
The explanation: lutein and zeaxanthin are fat-soluble. To be absorbed by the small intestinal enterocytes, they must first be solubilized in mixed micelles formed by bile acids and dietary lipids. From a leafy-green source, the carotenoids are bound within the plant cell matrix (cellulose cell walls, chloroplast thylakoid membranes) and must be released by chewing and mechanical/chemical digestion before they can partition into micelles. From an egg yolk, the carotenoids are already dissolved in a natural lipid emulsion stabilized by phospholipids (lecithin) — essentially a pre-formed micelle. Absorption is much more efficient.
The practical implication: although spinach delivers far more total lutein per serving, a smaller dose from eggs is absorbed and reaches the macula more reliably. The two strategies are complementary, not competitive. The ideal dietary approach is both: eat leafy greens for the high total dose, and eat eggs alongside them so that the lipid matrix improves absorption of the green-vegetable carotenoids as well. A common mistake is eating salad with a low-fat dressing, which dramatically reduces carotenoid absorption from the greens; adding eggs (or olive oil, or another fat source) to the meal can double or triple bioavailability.
The AREDS2 Trial and Macular Degeneration
The Age-Related Eye Disease Study (AREDS) was a landmark NIH-funded clinical trial published in 2001 that established a specific combination of antioxidant vitamins and minerals (the "AREDS formula": Vitamin C 500 mg, Vitamin E 400 IU, beta-carotene 15 mg, zinc 80 mg, copper 2 mg) as effective in slowing progression of age-related macular degeneration (AMD) in patients with intermediate or advanced disease. The trial randomized 3,640 participants and found a 25% reduction in progression to advanced AMD over five years in the active arm.
Two problems with the original AREDS formula emerged:
- High-dose beta-carotene was found in the contemporaneous ATBC and CARET trials to increase lung cancer risk in current and former smokers. AREDS patients who smoked or had recently smoked therefore could not safely take the AREDS formula as designed.
- Subsequent research suggested that lutein and zeaxanthin, not beta-carotene, were the carotenoids most directly relevant to macular pigment density and AMD pathophysiology — reflecting the fact that beta-carotene does not accumulate in the retina, while lutein and zeaxanthin selectively do.
AREDS2, published in JAMA in 2013, was designed to address both problems. The trial randomized 4,203 participants with intermediate or advanced AMD to receive (a) the original AREDS formula, (b) AREDS with lutein 10 mg + zeaxanthin 2 mg substituted for beta-carotene, (c) AREDS plus omega-3 fatty acids (EPA + DHA), or (d) AREDS with both substitutions. Results:
- Substituting lutein/zeaxanthin for beta-carotene preserved the AMD-progression benefit and eliminated the smoker safety concern.
- Adding omega-3 fatty acids provided no additional benefit beyond the carotenoids.
- Patients in the lowest tertile of dietary lutein/zeaxanthin intake at baseline benefited most from the substitution — supporting the hypothesis that the benefit operates through carotenoid repletion of macular pigment.
The AREDS2 formula (Vitamin C 500 mg, Vitamin E 400 IU, lutein 10 mg, zeaxanthin 2 mg, zinc 80 mg, copper 2 mg) became the new standard of care for intermediate and advanced AMD. It is sold as PreserVision AREDS2 (Bausch & Lomb) and as generic equivalents from most pharmacy chains.
For more on AMD pathophysiology, see our Macular Degeneration page.
Egg-Intervention Trials (Wenzel, Kelly, Goodrow)
A series of well-controlled intervention trials have established that adding eggs to the diet measurably raises serum lutein/zeaxanthin and macular pigment optical density.
- Wenzel et al. (2006) Journal of Nutrition — 24 healthy women aged 24-59 consumed 6 eggs per week (modified-yolk eggs with elevated lutein content) for 12 weeks. Serum zeaxanthin nearly doubled. MPOD increased significantly. Total serum cholesterol did not change. This was the cleanest demonstration that egg intake could raise macular pigment in adult women.
- Goodrow et al. (2006) Journal of Nutrition — 33 older adults (mean age 79) consumed one egg per day for five weeks. Serum lutein increased by 26%, zeaxanthin by 38%. Critically, serum LDL cholesterol and HDL cholesterol did not change — this study was one of the first to demonstrate the lutein/zeaxanthin benefit was decoupled from any LDL response in an older population.
- Kelly et al. (2014) Investigative Ophthalmology & Visual Science — 101 participants aged 50+ received egg-based interventions (whole eggs, egg-yolk beverage, or modified eggs) over 8 weeks. All three intervention arms produced measurable increases in serum lutein/zeaxanthin and macular pigment density.
- Handelman et al. (1999) American Journal of Clinical Nutrition — the original demonstration that egg-yolk consumption raises plasma lutein and zeaxanthin in healthy adults. This trial laid the groundwork for the larger interventions that followed.
The dosing range across these trials was one egg per day to one egg per day on average across the week. The duration was 5-12 weeks. All trials showed measurable benefit. The consistent finding is that modest egg intake (one to two eggs per day) over weeks-to-months is sufficient to raise macular carotenoid status — the dose-response is achievable from ordinary dietary intake, not from pharmacological supplementation.
Cataract Prevention Evidence
Cataract — the age-related opacification of the lens of the eye — is the leading cause of treatable blindness globally. Modern cataract surgery (phacoemulsification with intraocular lens implantation) is among the safest and most successful surgical procedures, but prevention of cataract formation remains a worthwhile goal.
The lens, like the macula, is a highly oxidatively stressed tissue. It is continuously exposed to visible and ultraviolet light, contains a high concentration of long-lived proteins (crystallins) that cannot be replaced, and depends on a metabolically expensive antioxidant system to prevent oxidative damage to those proteins. Lutein and zeaxanthin are the only carotenoids that accumulate measurably in the lens (at concentrations far lower than in the macula, but still functionally relevant), where they protect the lens crystallins from photooxidation.
Observational data from the Nurses' Health Study and the Health Professionals Follow-Up Study (both large US cohort studies running for decades) have consistently shown that participants in the highest quintile of lutein/zeaxanthin intake have approximately 20-30% lower risk of cataract extraction surgery compared to those in the lowest quintile. The effect is modest in absolute terms but consistent across populations and dose-responsive within the observational range.
Interventional evidence for cataract prevention is weaker than for AMD — the trials have not been done at the scale or duration needed to establish causation. But the mechanism is plausible, the observational signal is consistent, and the dietary intervention (eating eggs and leafy greens) has no downside. Patients concerned about cataract risk should ensure adequate lutein/zeaxanthin intake along with the other oxidative-stress mitigators (UV protection with quality sunglasses, smoking cessation, adequate Vitamin C and Vitamin E).
Blue Light, Screen Use, and MPOD
The proliferation of LED screens (smartphones, laptops, tablets, modern televisions) has generated public concern about "blue light" exposure and its effects on the retina. The relevant facts:
- LED screens emit relatively high proportions of short-wavelength blue light compared to older CRT and fluorescent displays. Peak emission is typically around 450-460 nm.
- The absolute intensity of blue light from a screen is far lower than from sunlight. A laptop at typical viewing distance emits roughly 1% of the blue light dose received by simply being outdoors on a sunny day.
- Direct screen-induced retinal photodamage at typical brightness and viewing distance is not biologically plausible based on dose-response data from photochemistry of the retinal photoreceptors.
- The legitimate concern with evening screen use is suppression of melatonin secretion (which is exquisitely sensitive to blue light through the intrinsically photosensitive retinal ganglion cells), leading to disrupted sleep timing and quality — not direct retinal damage.
So while blue-light-blocking glasses and screen filters have become a substantial consumer product category, the rigorous evidence for their value in preventing retinal damage is weak. The clearer benefit is for sleep hygiene: warmer color temperature in the evening (whether via blue-blocking glasses or device night-mode settings) reduces melatonin suppression and improves sleep onset.
For long-term retinal health, the more meaningful intervention is maintaining adequate macular pigment density throughout life. Higher MPOD provides a built-in optical filter that operates 24 hours a day, in every light condition, without requiring any consumer product purchase. The dietary approach (eggs, leafy greens, fat-containing meals) is essentially free and durable.
Practical Intake — How Many Eggs?
There is no formally established RDA for lutein and zeaxanthin. Most observational and intervention research suggests target intake in the range of 6-12 mg/day combined lutein + zeaxanthin for prevention of AMD and other oxidative retinal conditions. AREDS2 used 10 + 2 mg/day. The average American consumes approximately 1-2 mg/day, leaving most adults far below the protective range from diet alone.
Approximate dietary lutein + zeaxanthin content of common foods (per serving):
- Kale, 1 cup cooked: ~24 mg
- Spinach, 1 cup cooked: ~20 mg
- Collard greens, 1 cup cooked: ~12 mg
- Swiss chard, 1 cup cooked: ~12 mg
- Broccoli, 1 cup cooked: ~2 mg
- Brussels sprouts, 1 cup cooked: ~2 mg
- Green peas, 1 cup cooked: ~4 mg
- Pasture-raised egg yolk: ~0.4 mg per yolk (about 60% more than conventional eggs)
- Conventional egg yolk: ~0.25 mg per yolk
- Lutein-enriched eggs (marigold-fed hens): ~1.0 mg per yolk
- Avocado, 1/2 medium: ~0.4 mg
- Pistachios, 1 oz: ~0.4 mg
The pragmatic strategy for adequate macular carotenoid intake combines (a) daily leafy greens for total dose, (b) two to three eggs per day for high-bioavailability complement, (c) fat with every meal (olive oil, butter, avocado, or the eggs themselves) to improve micellar absorption of the green-vegetable carotenoids, and optionally (d) AREDS2 supplementation for patients with established AMD or significant family history.
Cautions and Special Populations
- Smokers and the AREDS formula history. Patients who currently smoke or have recently smoked should never take the original AREDS formula containing 15 mg beta-carotene because of the ATBC/CARET trial data showing increased lung cancer risk from high-dose isolated beta-carotene in smokers. The AREDS2 reformulation (substituting lutein/zeaxanthin for beta-carotene) is safe for smokers.
- Lutein/zeaxanthin from food is uniformly safe. No upper limit has been established because dietary intake at any realistic level has not been associated with adverse effects.
- Carotenoid yellowing. Very high intake of carotenoids (typically from carrot juice or pumpkin) can cause carotenodermia, a benign yellow-orange discoloration of the skin (especially the palms and soles). Lutein/zeaxanthin can also produce this effect at very high doses but it is rare from typical food intake. The discoloration resolves over weeks when intake is reduced.
- Drug interactions. No clinically significant drug interactions are established for lutein or zeaxanthin at typical intake levels.
- Obesity and reduced MPOD. Obese adults have measurably lower MPOD than lean adults at equivalent carotenoid intake, likely because adipose tissue sequesters fat-soluble carotenoids and reduces the proportion available for retinal accumulation. Weight loss can partially restore MPOD.
- Smoking and reduced MPOD. Active smoking dramatically reduces MPOD independent of dietary intake. The mechanism is thought to involve increased systemic oxidative stress that consumes circulating carotenoids before they can accumulate in the retina. Smoking cessation is the single largest modifiable intervention for retinal health.
- Macular degeneration progression beyond intermediate stage. The AREDS2 formula slows progression but does not reverse established AMD. Patients with neovascular ("wet") AMD typically require anti-VEGF intravitreal injections (ranibizumab, aflibercept, brolucizumab) as the primary intervention, with AREDS2 as adjunct.
Key Research Papers
- Chung HY, Rasmussen HM, Johnson EJ (2004). Lutein bioavailability is higher from lutein-enriched eggs than from supplements and spinach in men. J Nutr. 134(8):1887-93. — Search PubMed
- AREDS2 Research Group (2013). Lutein + zeaxanthin and omega-3 fatty acids for age-related macular degeneration: the Age-Related Eye Disease Study 2 (AREDS2) randomized clinical trial. JAMA. 309(19):2005-15. — PubMed: AREDS2 2013
- Wenzel AJ, Gerweck C, Barbato D, Nicolosi RJ, Handelman GJ, Curran-Celentano J (2006). A 12-wk egg intervention increases serum zeaxanthin and macular pigment optical density in women. J Nutr. 136(10):2568-73. — Search PubMed
- Goodrow EF, Wilson TA, Houde SC, Vishwanathan R, Scollin PA, Handelman G, Nicolosi RJ (2006). Consumption of one egg per day increases serum lutein and zeaxanthin concentrations in older adults without altering serum lipid and lipoprotein cholesterol concentrations. J Nutr. 136(10):2519-24. — Search PubMed
- Kelly ER, Plat J, Haenen GR, Kijlstra A, Berendschot TT (2014). The effect of modified eggs and an egg-yolk based beverage on serum lutein and zeaxanthin concentrations and macular pigment optical density: results from a randomized trial. PLoS One. 9(3):e92659. — Search PubMed
- Handelman GJ, Nightingale ZD, Lichtenstein AH, Schaefer EJ, Blumberg JB (1999). Lutein and zeaxanthin concentrations in plasma after dietary supplementation with egg yolk. Am J Clin Nutr. 70(2):247-51. — Search PubMed
- Bone RA, Landrum JT, Cao Y, Howard AN, Alvarez-Calderon F (2007). Macular pigment response to a xanthophyll supplement of lutein, zeaxanthin, and meso-zeaxanthin. Vision Res. 47(20):2580-90. — Search PubMed
- SanGiovanni JP, Chew EY, Clemons TE, Ferris FL 3rd, Gensler G et al. (2007). The relationship of dietary carotenoid and vitamin A, E, and C intake with age-related macular degeneration in a case-control study: AREDS Report No. 22. Arch Ophthalmol. 125(9):1225-32. — PubMed: SanGiovanni 2007
- Krinsky NI, Landrum JT, Bone RA (2003). Biologic mechanisms of the protective role of lutein and zeaxanthin in the eye. Annu Rev Nutr. 23:171-201. — Search PubMed
- Stringham JM, Hammond BR (2008). Macular pigment and visual performance under glare conditions. Optom Vis Sci. 85(2):82-8. — Search PubMed
- Christen WG, Liu S, Glynn RJ, Gaziano JM, Buring JE (2008). Dietary carotenoids, vitamins C and E, and risk of cataract in women: a prospective study. Arch Ophthalmol. 126(1):102-9. — PubMed: Christen cataract 2008
- Ma L, Dou HL, Wu YQ, Huang YM, Huang YB et al. (2012). Lutein and zeaxanthin intake and the risk of age-related macular degeneration: a systematic review and meta-analysis. Br J Nutr. 107(3):350-9. — PubMed: Ma meta-analysis 2012
- Hammond BR Jr, Fletcher LM, Roos F, Wittwer J, Schalch W (2014). A double-blind, placebo-controlled study on the effects of lutein and zeaxanthin on photostress recovery, glare disability, and chromatic contrast. Invest Ophthalmol Vis Sci. 55(12):8583-9. — Search PubMed
- Beatty S, Koh HH, Phil M, Henson D, Boulton M (2000). The role of oxidative stress in the pathogenesis of age-related macular degeneration. Surv Ophthalmol. 45(2):115-34. — PubMed: Beatty 2000
PubMed Topic Searches
- PubMed: Lutein zeaxanthin MPOD
- PubMed: AREDS2 AMD treatment
- PubMed: Egg yolk lutein bioavailability
- PubMed: Lutein zeaxanthin cataract
- PubMed: Meso-zeaxanthin macula
Connections
- Eggs Overview
- Eggs Benefits Hub
- Eggs for Choline & Brain
- Cholesterol Myth Revisited
- Pasture vs Cage-Free Eggs
- Macular Degeneration
- Vitamin A
- Vitamin A for Vision
- Vitamin C
- Vitamin E
- Zinc
- Kale
- Spinach
- Omega-3 Fatty Acids
- All Food