Dark Chocolate Mood and PEA
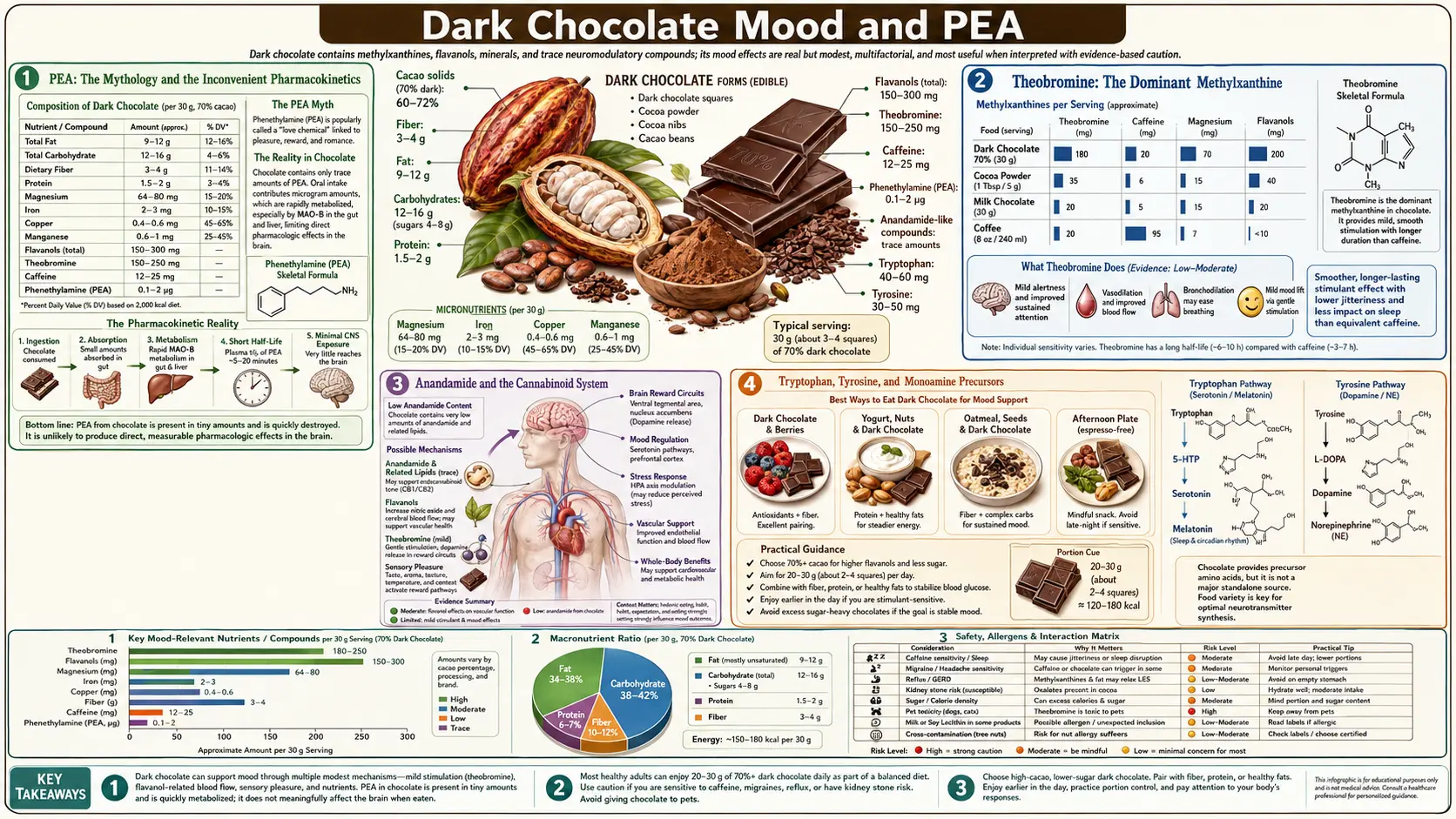
The cultural mythology that dark chocolate is a "love food" or "happiness food" is real but built on thinner physiology than the marketing implies. Cocoa contains beta-phenylethylamine (PEA), an endogenous trace amine released by the brain during attraction and elevated mood — but dietary PEA is largely degraded by monoamine oxidase B in the gut wall before reaching the brain, so the chocolate-as-love-drug story is more elegant than functional. The genuine mood mechanisms in dark chocolate are different: theobromine's mild dopaminergic and adenosine-antagonist effect (the dominant pharmacology), anandamide and N-acyl-ethanolamine signaling at cannabinoid receptors (small doses, plausible contribution), tryptophan and tyrosine as precursors for serotonin and dopamine (modest contribution at typical chocolate doses), and the well-documented hedonic-reward response to highly palatable food regardless of specific neuroactive content. This page walks through each mechanism honestly, distinguishes what the science actually supports from what marketing claims, and lands on a practical synthesis: dark chocolate genuinely modestly improves mood in short-term experiments, but mainly through the methylxanthine pharmacology, the placebo and pleasure response, and the broader cardiovascular-cognitive benefit — not through dietary PEA crossing into the brain.
Table of Contents
- PEA: The Mythology and the Inconvenient Pharmacokinetics
- Theobromine: The Dominant Methylxanthine
- Anandamide and the Cannabinoid System
- Tryptophan, Tyrosine, and Monoamine Precursors
- Cocoa Flavanols and Cognition
- What Mood Trials Actually Show
- The Hedonic-Reward Component
- Pre-Menstrual Chocolate Cravings: What the Research Says
- Dark Chocolate, Depression, and Anxiety
- Cautions and Limits of the Evidence
- Key Research Papers
- Connections
- Featured Videos
PEA: The Mythology and the Inconvenient Pharmacokinetics
Beta-phenylethylamine (PEA, sometimes written as 2-phenylethylamine) is an endogenous trace amine produced in the brain by decarboxylation of L-phenylalanine. Brain PEA acts as a neuromodulator that potentiates dopaminergic and noradrenergic signaling. Endogenous brain PEA levels rise during attraction, romantic love, exercise, certain types of exhilaration, and the manic phase of bipolar disorder. PEA is also one of the structural building blocks of stimulant drugs (amphetamine and its derivatives are substituted phenylethylamines).
Cocoa contains modest amounts of dietary PEA — approximately 0.5-3 mg per 100 g of cocoa or dark chocolate, with substantial variation by fermentation conditions and cacao variety. The Crews et al. and Pastore et al. surveys of biogenic amines in chocolate document the range. This is small in absolute terms (a 30 g serving of dark chocolate contains 0.15-1 mg PEA — the equivalent of a single drop of pure compound).
The chocolate-as-love-food cultural story rests on the assertion that dietary PEA from chocolate raises brain PEA and produces the mood and attraction effects of endogenous brain PEA. This assertion fails three rigorous tests:
- Gut-wall monoamine oxidase B degrades dietary PEA before systemic absorption. PEA is an excellent MAO-B substrate, and the intestinal mucosa contains substantial MAO-B activity. The vast majority of an oral PEA dose is deaminated to phenylacetic acid within the gut wall before reaching the portal circulation.
- What little PEA reaches portal circulation is largely cleared by hepatic first-pass metabolism. Liver MAO-A and MAO-B further degrade circulating PEA. Systemic plasma PEA after a typical dietary dose is essentially indistinguishable from baseline.
- Even systemically-administered pure PEA in clinical trials produces only brief and modest mood effects because the half-life is so short. The Sabelli group studied oral PEA combined with the MAO-B inhibitor selegiline in depressed patients and reported some benefit, but this required active MAO-B inhibition to allow PEA to reach the brain — conditions not present with dietary chocolate alone.
The honest summary: dietary PEA from chocolate does not meaningfully cross into the brain in the absence of MAO-B inhibition. The cultural story of chocolate as a "love chemical" is a real cultural fact and a thin physiological one. The mood effect from chocolate consumption is real but mechanistically operates through other pathways discussed below, not through PEA.
(Some patients on irreversible MAO-B inhibitors for Parkinson's disease — selegiline, rasagiline — may experience genuinely enhanced PEA effects from dietary sources including chocolate. The interaction is well documented but rarely clinically problematic. The MAO-A inhibitors used for atypical depression are a different concern because of the tyramine reaction, but the PEA in chocolate is not the relevant amine for that interaction.)
Theobromine: The Dominant Methylxanthine
The most pharmacologically active compound in dark chocolate for mood and energy is theobromine — not PEA, not anandamide, not flavanols. A 30 g serving of 70-85% dark chocolate contains approximately 200-300 mg theobromine plus 20-40 mg caffeine. Theobromine and caffeine are both methylxanthines with similar mechanisms but different kinetics.
Theobromine pharmacology:
- Mechanism — competitive antagonism at adenosine A1 and A2A receptors (the mechanism shared with caffeine), plus weak inhibition of phosphodiesterases. The adenosine antagonism reduces the inhibitory tone that adenosine normally exerts on dopaminergic and cholinergic neurons, producing mild stimulation of these systems.
- Half-life — approximately 7-12 hours in humans (compared with caffeine's 4-6 hours). The longer half-life produces a more sustained, gentler stimulant character.
- Onset — approximately 30-60 minutes after consumption, slower than caffeine's 15-30 minute onset. The effect builds gradually rather than spiking.
- Subjective character — smoother, less jittery than caffeine, with less vasoconstriction and less tendency to produce anxiety. The lower CNS stimulant intensity is a feature, not a bug.
- Mild vasodilation — theobromine produces modest peripheral vasodilation (in contrast to caffeine's vasoconstriction in the cerebral circulation), which may contribute to the warming sensation associated with dark chocolate consumption.
- Mild diuresis — theobromine is a mild diuretic. Heavy daily chocolate consumption can modestly increase urine output.
The Mitchell et al. 2011 paper in Psychopharmacology directly compared theobromine alone, caffeine alone, the combination, and placebo in healthy volunteers. Theobromine alone produced mild mood enhancement and small reductions in blood pressure; the combination of caffeine plus theobromine (as in chocolate) produced the largest improvement in mood and self-rated alertness. The Smit, Gaffan, and Rogers 2004 paper in Appetite reached the parallel conclusion that the methylxanthines are the dominant psychopharmacologically active constituents of chocolate, with the other neuroactive components contributing only marginally at typical dietary doses.
The practical implication is that dark chocolate is best understood pharmacologically as a gentler, more sustained-release alternative to coffee, with the cocoa flavanols and minerals as cardiovascular and metabolic add-ons. The 8-12 hour theobromine half-life means that mid-afternoon dark chocolate consumption can disrupt sleep for sensitive individuals.
Anandamide and the Cannabinoid System
The 1996 Nature paper by di Tomaso, Beltramo, and Piomelli identified that cocoa contains three lipid molecules with biological activity at the cannabinoid receptor system: anandamide (the prototypical endogenous cannabinoid, N-arachidonoylethanolamine), and two related N-acyl-ethanolamines (N-oleoylethanolamine and N-linoleoylethanolamine). Anandamide itself binds the CB1 and CB2 cannabinoid receptors; the N-acyl-ethanolamines inhibit FAAH (fatty acid amide hydrolase), the enzyme that degrades endogenous anandamide.
The mechanism is conceptually elegant: cocoa contains both the active ligand and the enzyme inhibitor that prolongs the ligand's half-life. The doses, however, are very small. The anandamide content of cocoa is approximately 50-60 ng per gram — meaning a 30 g serving delivers approximately 1.5-2 mcg of anandamide. The N-acyl-ethanolamine content is similarly small.
For comparison, the endogenous anandamide production rate in a typical adult is in the range of mg/day. Dietary anandamide from chocolate is roughly 1,000-fold smaller than endogenous production. Whether this 0.1% perturbation produces a meaningful pharmacologic effect at cannabinoid receptors is doubtful. The contribution of the FAAH-inhibiting N-acyl-ethanolamines to extending endogenous anandamide signaling is somewhat more plausible but also small.
The honest summary: cocoa contains genuine endocannabinoid-system ligands, the doses are small, and any contribution to mood from this pathway is at the margin. The 1996 Nature paper that put this on the cultural map was a genuine and elegant scientific discovery, but the popular framing that "chocolate produces cannabis-like effects" substantially over-reads what the doses can do.
Tryptophan, Tyrosine, and Monoamine Precursors
Cocoa is a modest source of the aromatic amino acids tryptophan and tyrosine. Tryptophan is the precursor to serotonin (via 5-hydroxytryptophan); tyrosine is the precursor to dopamine, norepinephrine, and epinephrine (via L-DOPA). The brain's synthesis of these monoamines is partly dependent on plasma availability of the precursor amino acids.
The numbers are small. A 30 g serving of dark chocolate provides approximately 50 mg tryptophan and 100 mg tyrosine. By comparison, a 30 g serving of pumpkin seeds provides ~170 mg tryptophan; a 3 oz serving of turkey provides ~250 mg tryptophan; a 3 oz serving of beef provides ~400 mg tyrosine. Dark chocolate is a minor amino acid source.
The classic story that "eating tryptophan-rich foods boosts serotonin" is itself substantially overstated — the actual rate-limiting step for brain serotonin synthesis is more closely tied to the ratio of tryptophan to other large neutral amino acids (LNAA) crossing the blood-brain barrier than to total dietary tryptophan. A pure-carbohydrate meal raises this ratio (via insulin clearing the competing LNAA) more effectively than a tryptophan-rich protein meal.
The honest assessment: cocoa's amino acid contribution to mood is small relative to the methylxanthine pharmacology and the hedonic-reward response. The "chocolate raises serotonin via tryptophan" story is real but quantitatively modest.
Cocoa Flavanols and Cognition
The cocoa flavanol benefit story extends to mood and cognition in part because of the cerebrovascular effect — flavanols dilate cerebral arteries, raise cerebral blood flow, and modestly improve cognitive performance, particularly in older adults and in cognitively-demanding tasks under stress.
- Brickman et al. 2014 (Nature Neuroscience) showed that a 3-month intervention with high-flavanol cocoa drink in healthy older adults produced measurable improvement in dentate-gyrus-dependent memory tasks, parallel to improvement in cerebral blood flow to that brain region.
- Scholey AB et al. reported acute improvements in cognitive performance (serial subtraction, rapid visual information processing) within 2 hours of cocoa flavanol drink in healthy young adults, with parallel improvements in self-rated mental fatigue.
- Sokolov AN et al. 2013 reviewed cocoa flavanol effects on neurobiology, concluding that the evidence for cerebrovascular and cognitive benefit is more robust than for mood effects specifically.
- Pase MP et al. reported modest mood improvement (positive affect, fatigue reduction) but not cognitive performance improvement after chronic cocoa flavanol intake in healthy adults.
- COSMOS-Mind sub-study reported small but statistically significant improvement in executive function in older adults taking cocoa extract for 3 years, consistent with a cerebrovascular mechanism.
The mechanism is consistent across studies: cocoa flavanols improve cerebrovascular function via the same eNOS-nitric-oxide pathway that operates in the peripheral vasculature. The brain benefit is partly direct (better-perfused brain regions perform better) and partly indirect (improved global cardiovascular function reduces cumulative microvascular brain injury over years).
The mood-specific effects of cocoa flavanols are smaller and more heterogeneous than the cognitive effects. Some trials report meaningful mood improvement, others find no significant effect. The summary is that flavanols contribute mildly to mood through the cerebrovascular pathway, but the dominant short-term mood effect of dark chocolate is the methylxanthine pharmacology and hedonic reward.
What Mood Trials Actually Show
A series of controlled trials have measured short-term mood response to chocolate or cocoa consumption versus placebo. The general pattern:
- Macht and Mueller 2007 (Appetite) showed that 12.5 g of palatable chocolate (vs. unpalatable chocolate or no food) produced significant short-term improvement in negative mood in induced sad mood states. The improvement was largely abolished when participants disliked the chocolate. This indicates a palatability/hedonic-reward effect rather than a pharmacologic effect of any specific cocoa constituent.
- Parker, Parker, Brotchie 2006 (J Affect Disord) reviewed chocolate and mood interactions, concluding that mood-driven chocolate consumption (the seeking of palatable food during dysphoric mood) is well-documented, while pharmacologic mood improvement from chocolate is small and short-lived.
- Pase MP et al. 2013 reported that 4 weeks of daily cocoa polyphenol intake improved self-rated calmness and contentment in healthy adults, without parallel improvement in cognitive performance.
- Cosmos-Mind 2023 did not show significant mood improvement with cocoa extract over 3 years in healthy older adults, despite some cognitive benefit.
- Mitchell et al. 2011 directly compared methylxanthines and showed theobromine contributed more to mood improvement than caffeine alone, with the combination producing the largest effect.
The honest synthesis: dark chocolate produces a small but real short-term mood improvement that compounds three contributions of similar magnitude:
- Methylxanthine pharmacology (theobromine + caffeine; the largest single contributor)
- Hedonic reward from palatable food (well-documented even for non-chocolate palatable foods)
- Modest cerebrovascular and possibly endocannabinoid effects (smaller contributors)
The PEA story, in contrast, has essentially no empirical support beyond the cultural narrative. PEA from dietary chocolate does not reach the brain at meaningful concentrations.
The Hedonic-Reward Component
One of the most consistent findings in chocolate-and-mood research is that the mood benefit depends substantially on whether the participant enjoys the chocolate. In Macht and Mueller's 2007 work, palatable chocolate improved mood while unpalatable chocolate produced no significant mood improvement — despite delivering the same pharmacologic load of theobromine, caffeine, flavanols, and PEA.
This is the hedonic-reward component, mediated by the brain's mesolimbic dopamine system. The anticipation, consumption, and post-consumption pleasure of a highly palatable food activates the ventral tegmental area, nucleus accumbens, and related reward circuitry. The dopamine release produces the immediate "mood lift" that is the most subjectively obvious effect of chocolate consumption. This effect is non-specific — any food that the eater enjoys produces a similar mesolimbic activation. Chocolate is exceptionally good at this because of its texture (cocoa butter melts precisely at body temperature, producing a unique melt-in-mouth sensation), its flavor complexity, its cultural associations, and its calorie density (the mesolimbic system evolved to reward high-energy foods).
The implications:
- Eating chocolate you genuinely enjoy produces real mood benefit. This is not "just placebo" — it is a real neurobiological effect of pleasure perception.
- Eating chocolate you do not enjoy produces little mood benefit, regardless of the cocoa content.
- The mood improvement from chocolate is largely temporary (resolving in 30-90 minutes), parallel to the time course of the hedonic-reward response. The longer-term methylxanthine effect persists for several hours.
- The mood-improving effect of chocolate, like other palatable foods, can drive overconsumption when used as a coping mechanism for chronic negative affect. The pattern of using chocolate as emotional self-medication is common and not benign at the population level — it contributes to weight gain and to the substitution of food rewards for needed lifestyle, social, or psychological interventions.
Pre-Menstrual Chocolate Cravings: What the Research Says
The frequently-reported cultural pattern of pre-menstrual chocolate craving in women is real (consistent across surveys; approximately 30-50% of menstruating women in Western countries report increased chocolate craving in the late luteal phase). The mechanism is less clear and probably multi-causal:
- Magnesium hypothesis — pre-menstrual magnesium status drops modestly with the late-luteal progesterone increase, and chocolate is a magnesium-rich food. The body's craving for magnesium could partially explain the chocolate-specific pattern. Empirical support is weak.
- Serotonin hypothesis — the same late-luteal progesterone increase reduces serotonin synthesis, contributing to pre-menstrual dysphoria. Carbohydrate-rich foods (including chocolate) raise the tryptophan-to-LNAA ratio crossing the blood-brain barrier and transiently increase brain serotonin synthesis. This is a general carbohydrate effect, not chocolate-specific.
- Cultural conditioning — in cross-cultural comparison, the chocolate-craving pattern is much stronger in Western countries than in countries where chocolate is not the culturally-defined comfort food. Egyptian and Japanese women report similar magnitude of pre-menstrual cravings but for different specific foods. This suggests that the chocolate-specificity is partly learned, not entirely biological.
- Hedonic-reward mechanism — during pre-menstrual dysphoric mood, the brain seeks reliable mood-improving stimuli. Chocolate is reliably mood-improving for most women, so it gets sought.
The practical clinical synthesis: pre-menstrual chocolate craving is a real phenomenon, the mechanism is multi-factorial, and modest consumption (one ounce of high-cacao dark chocolate) is unlikely to cause meaningful harm and may genuinely improve dysphoric mood. The pattern becomes problematic only when it escalates to consumption levels that cause weight gain or substitute for needed pre-menstrual symptom management (exercise, sleep, magnesium supplementation, and in some cases SSRI luteal-phase dosing for severe PMDD).
Dark Chocolate, Depression, and Anxiety
The question of whether dark chocolate has clinical utility in depression and anxiety has been studied in several small trials with mixed results. The general findings:
- Several short-term trials in subclinical and mild depression report modest improvement in mood scales with daily dark chocolate or cocoa flavanol intake compared with placebo. Effect sizes are small (often <0.3 standardized mean difference).
- The benefit is comparable to other small dietary interventions (e.g., increased omega-3 intake, increased fruit and vegetable intake) and substantially smaller than evidence-based psychotherapy or pharmacologic treatment for moderate-to-severe depression.
- The benefit is most consistent in older adults, where the cerebrovascular mechanism is most plausible — cocoa flavanols may improve mood partly by improving general brain perfusion in adults with subclinical microvascular brain dysfunction.
- For anxiety specifically, the evidence is weaker than for depression. Some short-term reduction in self-rated anxiety with cocoa flavanol intake has been reported but is inconsistent across trials.
- The MIND-AD and similar diet-and-depression studies place dark chocolate among the "neutral or modestly beneficial" foods, not in the high-priority dietary intervention list for depression.
The honest synthesis: dark chocolate produces small mood benefits in subclinical and mild depression but is not a substitute for evidence-based depression treatment. People with significant depressive or anxiety symptoms should pursue established interventions (psychotherapy, exercise, light therapy where seasonal, pharmacologic treatment where indicated) rather than treating dark chocolate as a primary intervention. Dark chocolate is at most a complementary dietary adjunct.
For people with subclinical or non-pathological negative mood (the routine "had a hard day" experience), a small portion of high-quality dark chocolate is a reasonable and culturally sanctioned mood-improving food choice. The improvement is real, even if its mechanism is largely the methylxanthine pharmacology and the hedonic-reward response rather than the more romantic PEA story.
Cautions and Limits of the Evidence
- Do not use dark chocolate as a substitute for evidence-based depression treatment. The mood effect is small and not clinically adequate for moderate-to-severe depression.
- The "chocolate as PEA / love drug" framing is mostly cultural mythology. Dietary PEA is degraded by gut-wall MAO-B before systemic absorption. The genuine mood mechanisms are methylxanthine pharmacology, hedonic reward, and (smaller) cerebrovascular and endocannabinoid pathways.
- Methylxanthine load matters for sleep. 30 g of 85% chocolate delivers ~300 mg theobromine plus ~40 mg caffeine, with theobromine's 7-12 hour half-life. Mid-afternoon and later consumption can impair sleep for sensitive individuals.
- MAO-B inhibitor users (selegiline, rasagiline for Parkinson's) may experience enhanced effects from dietary PEA in chocolate. This is rarely clinically problematic but worth knowing.
- SSRI users who experience initial GI upset may find dark chocolate worsens it during the first weeks of therapy.
- Emotional eating pattern. The use of palatable food (including chocolate) as a primary coping mechanism for chronic negative affect is a documented contributor to weight gain and to the avoidance of needed lifestyle and psychological interventions. Modest deliberate enjoyment is fine; reflexive emotional self-medication is not.
- Children with ADHD — the methylxanthine load (caffeine plus theobromine) can interact unfavorably with stimulant medications. Adjust afternoon and evening chocolate intake if a child is on stimulants.
- Pregnancy — methylxanthine intake should be moderated during pregnancy. The standard guidance limits total daily caffeine to 200 mg; the caffeine in dark chocolate plus theobromine should be factored in. The mood effect of pregnancy-appropriate amounts (one ounce) is modest and probably worthwhile if cravings exist.
- Migraine patients — a subset identifies chocolate as a migraine trigger. The evidence for chocolate as an independent trigger is weaker than for cheese, red wine, or aged meats, but individual variation matters and patients should test their own response.
Key Research Papers
- di Tomaso E, Beltramo M, Piomelli D (1996). Brain cannabinoids in chocolate. Nature. — Search PubMed
- Smit HJ, Gaffan EA, Rogers PJ (2004). Methylxanthines are the psycho-pharmacologically active constituents of chocolate. Psychopharmacology. — PubMed
- Mitchell ES et al. (2011). Differential contributions of theobromine and caffeine on mood, psychomotor performance and blood pressure. Physiol Behav. — Search PubMed
- Macht M, Mueller J (2007). Immediate effects of chocolate on experimentally induced mood states. Appetite. — Search PubMed
- Parker G, Parker I, Brotchie H (2006). Mood state effects of chocolate. J Affect Disord. — Search PubMed
- Pase MP et al. (2013). Cocoa polyphenols enhance positive mood states but not cognitive performance: a randomized, placebo-controlled trial. J Psychopharmacol. — PubMed
- Scholey AB et al. (2010). Consumption of cocoa flavanols results in acute improvements in mood and cognitive performance during sustained mental effort. J Psychopharmacol. — PubMed
- Brickman AM et al. (2014). Enhancing dentate gyrus function with dietary flavanols improves cognition in older adults. Nat Neurosci. — PubMed
- Sokolov AN et al. (2013). Chocolate and the brain: neurobiological impact of cocoa flavanols on cognition and behavior. Neurosci Biobehav Rev. — PubMed
- Sabelli HC et al. (1996). Sustained antidepressant effect of PEA replacement. J Neuropsychiatry Clin Neurosci. — Search PubMed
- Crews C et al. (2001). A survey of bioactive amines in chocolate and other cocoa-containing products. Food Addit Contam. PubMed
- Mumford GK et al. (1996). Absorption rate of methylxanthines following capsules, cola and chocolate. Eur J Clin Pharmacol. — Search PubMed
- Mostofsky E et al. (2010). Chocolate intake and incidence of heart failure: a population-based prospective study of middle-aged and elderly women. Circ Heart Fail. — Search PubMed
PubMed Topic Searches
- PubMed: Chocolate mood randomized trials
- PubMed: Theobromine mood human
- PubMed: PEA depression MAO-B
- PubMed: Anandamide chocolate
- PubMed: Cocoa flavanol cognition older adults
Connections
- Dark Chocolate Overview
- Dark Chocolate Benefits Hub
- Flavanols & Endothelial Function
- Iron, Magnesium & Mineral Content
- Cacao Percentage & Sugar
- Coffee (Methylxanthines)
- Green Tea (L-Theanine)
- Tryptophan
- Tyrosine
- Magnesium
- Depression
- Anxiety
- Migraine
- Parkinson's Disease
- Antioxidants