Bananas for Potassium and Heart Rhythm
A medium banana delivers 422 mg of potassium against essentially zero sodium, a ratio of roughly 200:1 that is the inverse of nearly every processed food in the modern Western diet. The clinical consequences are large: every 1,000 mg per day increase in dietary potassium intake is associated with a 24% reduction in stroke risk (D'Elia 2011 meta-analysis), the DASH-Sodium trial established a roughly 7-11 mm Hg systolic blood pressure reduction from a potassium- and magnesium-rich diet pattern, and chronic hypokalemia from loop diuretics is independently associated with ventricular arrhythmia and sudden cardiac death. The banana is not the densest potassium food per gram (a baked potato, white beans, and yogurt all win on density), but it is the most convenient, the least preparation-intensive, and the most clinically recognized — which is why generations of cardiologists have written "eat a banana a day" on discharge instructions next to furosemide prescriptions.
Table of Contents
- Why Potassium Matters: The Intracellular Cation
- The Sodium / Potassium Ratio (Not Just Sodium)
- The DASH and DASH-Sodium Evidence
- Stroke Prevention
- Hypokalemia, Ventricular Arrhythmia, and Atrial Fibrillation
- The Loop Diuretic / Banana Interaction
- How Much Banana to Move the Needle?
- Cautions: When Bananas Are Dangerous (CKD, Spironolactone, ACE Inhibitors)
- Practical Guidance
- Key Research Papers
- Connections
- Featured Videos
Why Potassium Matters: The Intracellular Cation
Potassium is the dominant intracellular cation in the human body. Approximately 98% of total body potassium (roughly 3,500 mmol in a 70 kg adult) sits inside cells, where it maintains the resting membrane potential of every excitable tissue — cardiac myocytes, neurons, skeletal muscle, vascular smooth muscle. The remaining 2% in the extracellular space (4 mmol per liter of plasma, by reference range) is the part that gets measured on a basic metabolic panel, but it represents only the tip of an iceberg whose stability depends on transmembrane gradients maintained by the Na+/K+ ATPase pump.
The cardiac consequences of disturbed potassium are direct. Hypokalemia (serum K+ < 3.5 mmol/L) lengthens the action potential by delaying repolarization, prolonging the QT interval, and predisposing to torsades de pointes, ventricular tachycardia, and ventricular fibrillation. Hyperkalemia (serum K+ > 5.5 mmol/L) shortens the action potential, depolarizes the membrane toward firing threshold initially but then inactivates the sodium channel, producing peaked T waves, widened QRS, sine-wave morphology, and ultimately asystole. The therapeutic window for serum potassium is one of the narrowest of any electrolyte, and the dietary lever to keep a patient inside it — high dietary potassium relative to sodium — is one of the most consistently underutilized tools in cardiology.
The Sodium / Potassium Ratio (Not Just Sodium)
For roughly 40 years, public health messaging on cardiovascular nutrition focused almost exclusively on sodium reduction. The DASH (Dietary Approaches to Stop Hypertension) and INTERSALT studies forced a more nuanced view: the ratio of sodium to potassium matters at least as much as absolute sodium intake, and possibly more.
The Yang et al. analysis of NHANES III follow-up data (Archives of Internal Medicine 2011) followed 12,267 U.S. adults for a median of 14.8 years and found that the sodium-to-potassium ratio was a stronger predictor of cardiovascular and all-cause mortality than sodium or potassium alone. Adults in the highest quartile of Na/K ratio had a 46% higher risk of cardiovascular mortality compared to the lowest quartile. The PURE study (Prospective Urban Rural Epidemiology, Lancet 2014) of over 100,000 adults in 17 countries found that potassium excretion of 1.5 to 2 g per day (corresponding to a dietary intake of roughly 2 to 3 g) was associated with significantly lower blood pressure and cardiovascular events.
The dietary translation is that a meal containing a single banana with a slice of bread converts the meal from net-sodium to net-potassium. The same is true of substituting sweet potato for white potato chips, yogurt for sour cream, beans for cheese, leafy greens for bacon. These swaps do not require the disciplined "low sodium" mindset that most patients eventually abandon — they are positive substitutions in which the high-potassium food displaces the high-sodium food at the level of the plate.
The DASH and DASH-Sodium Evidence
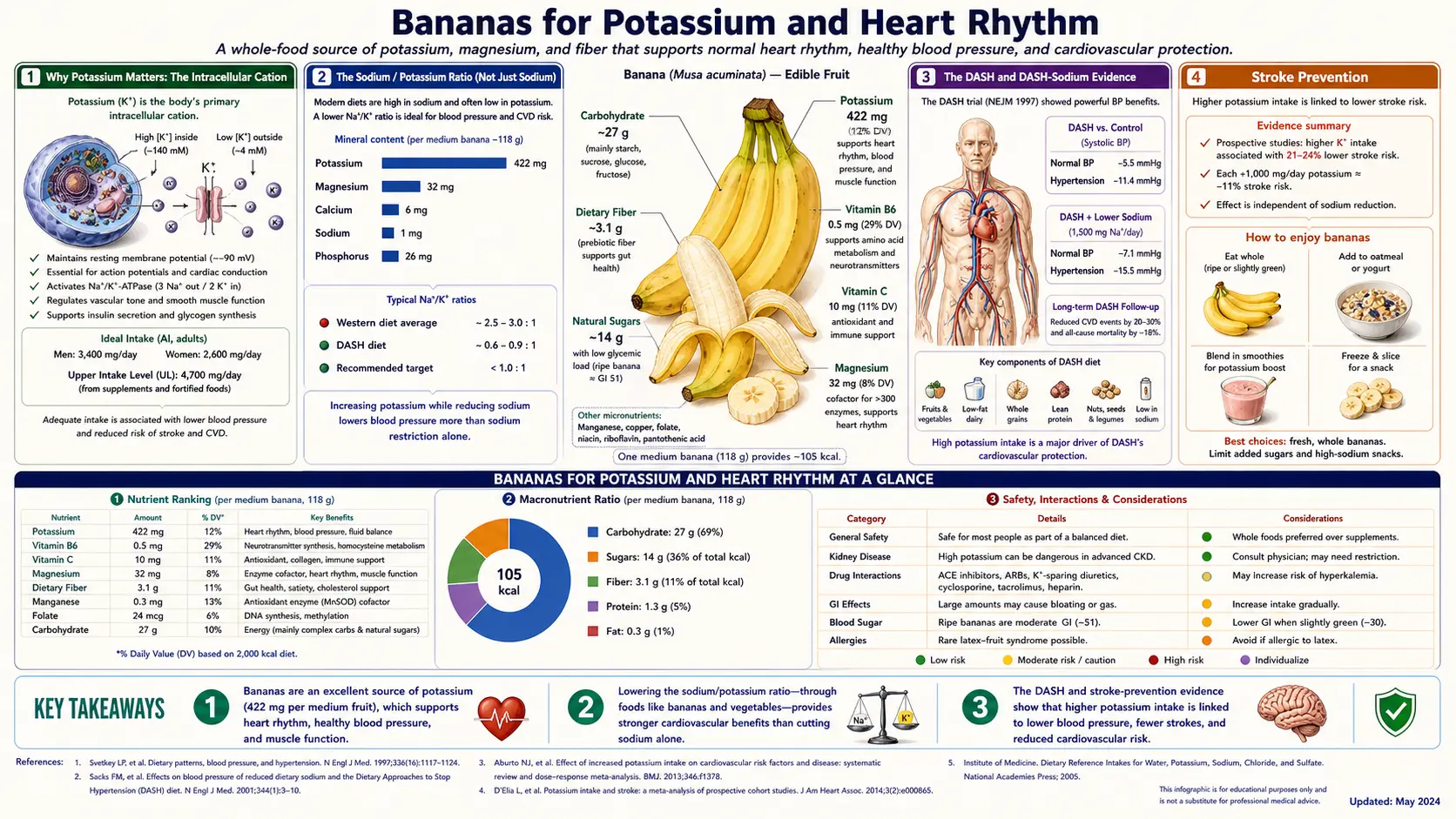
The DASH trial (Appel LJ et al., NEJM 1997) randomized 459 adults with systolic BP < 160 and diastolic 80-95 to one of three diets for eight weeks: a control diet typical of the average American intake, a fruit-and-vegetable-enriched version of the control, or the full DASH diet (rich in fruits, vegetables, low-fat dairy, with reduced saturated and total fat). The fruit-and-vegetable diet alone reduced systolic BP by 2.8 mm Hg and diastolic by 1.1 mm Hg compared to control. The full DASH diet reduced systolic by 5.5 mm Hg and diastolic by 3.0 mm Hg. In the subgroup with hypertension at baseline, the DASH diet reduced systolic by 11.4 mm Hg and diastolic by 5.5 mm Hg — a magnitude of effect comparable to single-agent antihypertensive monotherapy.
DASH-Sodium (Sacks FM et al., NEJM 2001) added a sodium-reduction arm to the DASH diet and demonstrated additive blood-pressure reduction. The combination of the full DASH diet plus the lowest sodium intake (1,500 mg per day) reduced systolic blood pressure by an additional 8.9 mm Hg compared to the control diet at the highest sodium intake (3,300 mg per day) — a total effect comparable to two-drug antihypertensive therapy. The potassium content of the DASH diet is roughly 4,500 mg per day, of which a daily banana would contribute approximately 9% — meaningful but not transformative on its own.
Stroke Prevention
Stroke is the cardiovascular endpoint most consistently and robustly responsive to dietary potassium intake. The D'Elia et al. meta-analysis (Journal of the American College of Cardiology 2011) pooled 11 cohort studies with 247,510 participants and 7,066 stroke events and found that for every 1,000 mg per day increase in dietary potassium intake, total stroke risk fell by 24%. The relationship was dose-responsive and consistent across study populations.
The mechanism is partly the blood-pressure-lowering effect described above, but appears to be larger than blood pressure alone can account for. Direct vascular effects of potassium include reduced free-radical generation in endothelium, reduced vascular smooth muscle proliferation, and improved nitric-oxide-mediated vasodilation. There is also evidence that high-potassium diets reduce platelet aggregation independent of blood pressure.
The implication for the individual patient is that even if a single banana per day produces a clinically trivial change in blood pressure (1-2 mm Hg), the lifetime accumulation of high-potassium dietary days produces a substantial reduction in stroke risk. For an adult with a 10% lifetime stroke risk, a sustained shift to higher potassium intake could reduce that to 7% or below — comparable to or larger than the effect of a daily aspirin in primary prevention.
Hypokalemia, Ventricular Arrhythmia, and Atrial Fibrillation
Hypokalemia is one of the most common electrolyte disturbances in hospitalized patients and the most common iatrogenic electrolyte disturbance in outpatients (driven almost entirely by thiazide and loop diuretics). The relationship between serum potassium and arrhythmia is non-linear and clinically consequential.
- Serum K+ 3.5 to 4.0 mmol/L: within reference range but associated with increased risk of ventricular ectopy in patients with structural heart disease. Many cardiologists target > 4.0 mmol/L in patients with heart failure or after myocardial infarction.
- Serum K+ 3.0 to 3.5 mmol/L: mild hypokalemia, usually asymptomatic but with measurable increase in premature ventricular contractions and prolongation of the QT interval. The threshold for replacement in hospitalized patients.
- Serum K+ < 3.0 mmol/L: moderate-to-severe hypokalemia, marked QT prolongation, risk of torsades de pointes especially in the setting of any QT-prolonging medication.
- Serum K+ < 2.5 mmol/L: severe hypokalemia, IV replacement indicated, high risk of ventricular fibrillation.
The atrial fibrillation literature is somewhat different. Hypomagnesemia is the more direct trigger for new-onset AF, but hypokalemia compounds the effect because magnesium and potassium handling are physiologically linked at the renal tubule (you cannot effectively correct hypokalemia in the presence of hypomagnesemia). A banana is not a clinically meaningful magnesium source (only 32 mg per fruit, about 8% DV) but the combination of a banana plus a small handful of almonds or a spoonful of pumpkin seeds covers both bases.
The Loop Diuretic / Banana Interaction
The most consequential single-patient population for the banana-as-potassium-source story is the heart failure patient on furosemide (Lasix), torsemide, or bumetanide. Loop diuretics inhibit the Na+/K+/2Cl- cotransporter in the thick ascending loop of Henle, increasing sodium and water excretion. As a side effect, they also increase potassium excretion at distal tubules due to increased distal sodium delivery. A patient on 40 mg of furosemide twice daily will typically lose 30-60 mmol of potassium per day — equivalent to roughly three to six bananas, more than what dietary substitution alone can usually replace.
The standard cardiology approach to diuretic-induced hypokalemia is potassium chloride supplementation (e.g., 20-40 mEq oral KCl daily) plus a "potassium-rich diet" of which bananas are the iconic representative. The realistic estimate is that bananas account for about 10-25% of the corrective potassium intake; KCl tablets do the rest. The dietary contribution still matters because:
- Patients are more adherent to a daily banana than to a daily KCl tablet (which most patients find unpleasant).
- Dietary potassium comes packaged with magnesium, fiber, and antioxidants, none of which are present in a KCl tablet.
- The dietary form is less likely to produce the acute hyperkalemia that can occur from a missed-dose-doubled-up KCl regimen.
The combination of a loop diuretic, an aldosterone antagonist (spironolactone or eplerenone), and an ACE inhibitor or ARB — the modern guideline-directed medical therapy for HFrEF — produces a more balanced potassium handling. Aldosterone antagonists and RAAS blockers retain potassium; loop diuretics waste it; the patient ends up with a serum potassium close to baseline. In this triple-therapy setting, the banana prescription is less universal and requires monitoring — some patients on the triple regimen develop hyperkalemia from a high-potassium diet.
How Much Banana to Move the Needle?
The U.S. adequate intake (AI) for potassium in adults is 3,400 mg per day for men and 2,600 mg per day for women. The actual median intake in U.S. adults is approximately 2,500 mg for men and 1,900 mg for women — well below the AI. The gap of roughly 700-900 mg per day translates to about two medium bananas per day, but the more realistic dietary advice is to combine several potassium-rich foods rather than rely on a single source.
Worked example for a 60-year-old hypertensive patient currently consuming a typical American diet:
- Baseline potassium intake: ~2,200 mg per day
- Add one medium banana at breakfast: +422 mg
- Switch from white potato chips to baked sweet potato at lunch: +542 mg (sweet potato) − 0 (chips) = net +542 mg
- Add 1 cup of cooked spinach with dinner: +839 mg
- Add 6 oz plain Greek yogurt as snack: +240 mg
- New total: ~4,243 mg per day — comfortably above the AI and approaching the DASH-diet target of ~4,500 mg.
The banana is the single easiest entry point in this menu of substitutions, which is the practical reason for its iconic status. It is portable, requires no preparation, has biodegradable packaging, is inexpensive year-round, and is well-tolerated by patients with sensitive stomachs or chemotherapy-induced nausea where many other potassium-rich foods are not.
Cautions: When Bananas Are Dangerous (CKD, Spironolactone, ACE Inhibitors)
The general "eat more bananas" advice has important exceptions in three populations where the kidneys cannot adequately excrete a potassium load, or where co-administered medications retain potassium:
- Chronic kidney disease (CKD stages 4-5): as glomerular filtration rate falls below 30 mL/min/1.73m², the kidney loses its ability to excrete a potassium load. A meal containing 1,000 mg of dietary potassium that an intact kidney clears in a few hours can produce a sustained hyperkalemia in advanced CKD. Renal-diet education emphasizes restricting potassium-rich foods including bananas, oranges, potatoes, tomatoes, and spinach.
- Aldosterone antagonists (spironolactone, eplerenone): these drugs block the aldosterone-mediated potassium secretion at the principal cell of the cortical collecting duct. Patients on spironolactone 25 mg or higher daily, particularly in the context of heart failure or cirrhosis, can develop hyperkalemia even with modest dietary increases.
- ACE inhibitors and ARBs: these drugs reduce aldosterone secretion and produce a milder potassium-retention effect. Most patients tolerate normal dietary potassium, but the combination of ACE inhibitor + ARB + aldosterone antagonist + low GFR can produce dangerous hyperkalemia.
Other medications that increase the risk of hyperkalemia include trimethoprim (Bactrim), potassium-sparing diuretics (amiloride, triamterene), heparin (in prolonged use), and non-steroidal anti-inflammatories. Patients on any of these who are also told to "eat more bananas" should have their serum potassium checked within two weeks of initiating the dietary change.
Practical Guidance
- For the average healthy adult: a daily banana, ideally consumed alongside other potassium-rich foods (sweet potato, spinach, beans, yogurt), is a safe and effective contribution toward meeting the 3,400 mg adequate intake.
- For the hypertensive patient not on potassium-sparing medications: two bananas per day plus the DASH-diet emphasis on fruits, vegetables, and low-fat dairy reliably reduces blood pressure by 5-11 mm Hg over 4-8 weeks.
- For the heart failure patient on loop diuretics without aldosterone antagonists: a daily banana is a useful but insufficient adjunct to prescription potassium replacement; do not substitute a banana for prescribed KCl.
- For the heart failure patient on the guideline triple therapy (loop diuretic + ACE inhibitor + spironolactone): dietary potassium should be moderated, not maximized; consult the treating cardiologist before increasing daily intake.
- For the CKD patient with GFR < 30 mL/min: follow the renal dietitian's specific potassium prescription; bananas may need to be restricted to 1-2 per week or eliminated.
- Timing tip: a banana eaten with the evening meal (rather than as a morning snack) tends to produce a more sustained serum potassium because the postprandial insulin response drives potassium into cells, smoothing the peak and trough.
Key Research Papers
- Appel LJ et al., A clinical trial of the effects of dietary patterns on blood pressure (DASH original) — NEJM 1997 — PMID: 9099655
- Sacks FM et al., Effects on blood pressure of reduced dietary sodium and the DASH diet (DASH-Sodium) — NEJM 2001 — PMID: 11136953
- INTERSALT Cooperative Research Group, sodium and blood pressure across populations — BMJ 1988 — PMID: 3416162
- O'Donnell M et al., PURE study, urinary sodium and potassium and cardiovascular events — NEJM 2014 — PMID: 25119608
- D'Elia L et al., potassium intake and stroke risk meta-analysis — JACC 2011 — PMID: 21371638
- Yang Q et al., sodium and potassium intake and mortality among U.S. adults (NHANES III follow-up) — Arch Intern Med 2011 — PMID: 21747015
- Aburto NJ et al., effect of increased potassium intake on cardiovascular risk factors — BMJ 2013 — PMID: 23558164
- SPRINT trial, intensive vs standard blood pressure control — NEJM 2015 — PMID: 26551272
- Knochel JP, mechanism of diuretic-induced potassium depletion — PubMed: Knochel diuretic K+ depletion
- Macdonald JE, Struthers AD, hypokalemia and arrhythmia in heart failure — PubMed: K+ and arrhythmia in HF
- Krishna GG, effect of potassium intake on blood pressure — PubMed: Krishna K+ and BP
- Whelton PK et al., effects of oral potassium on blood pressure meta-analysis — JAMA 1997 — PMID: 9168293
Connections
- Bananas Benefits (Hub)
- Bananas (Main Page)
- Bananas for Athletic Performance
- Resistant Starch: Green vs Ripe
- Potassium
- Magnesium
- Sodium
- Hypertension
- Atrial Fibrillation
- Heart Failure
- Chronic Kidney Disease
- Sweet Potatoes (Potassium Comparison)
- Yogurt
- DASH Diet