Bronchiectasis
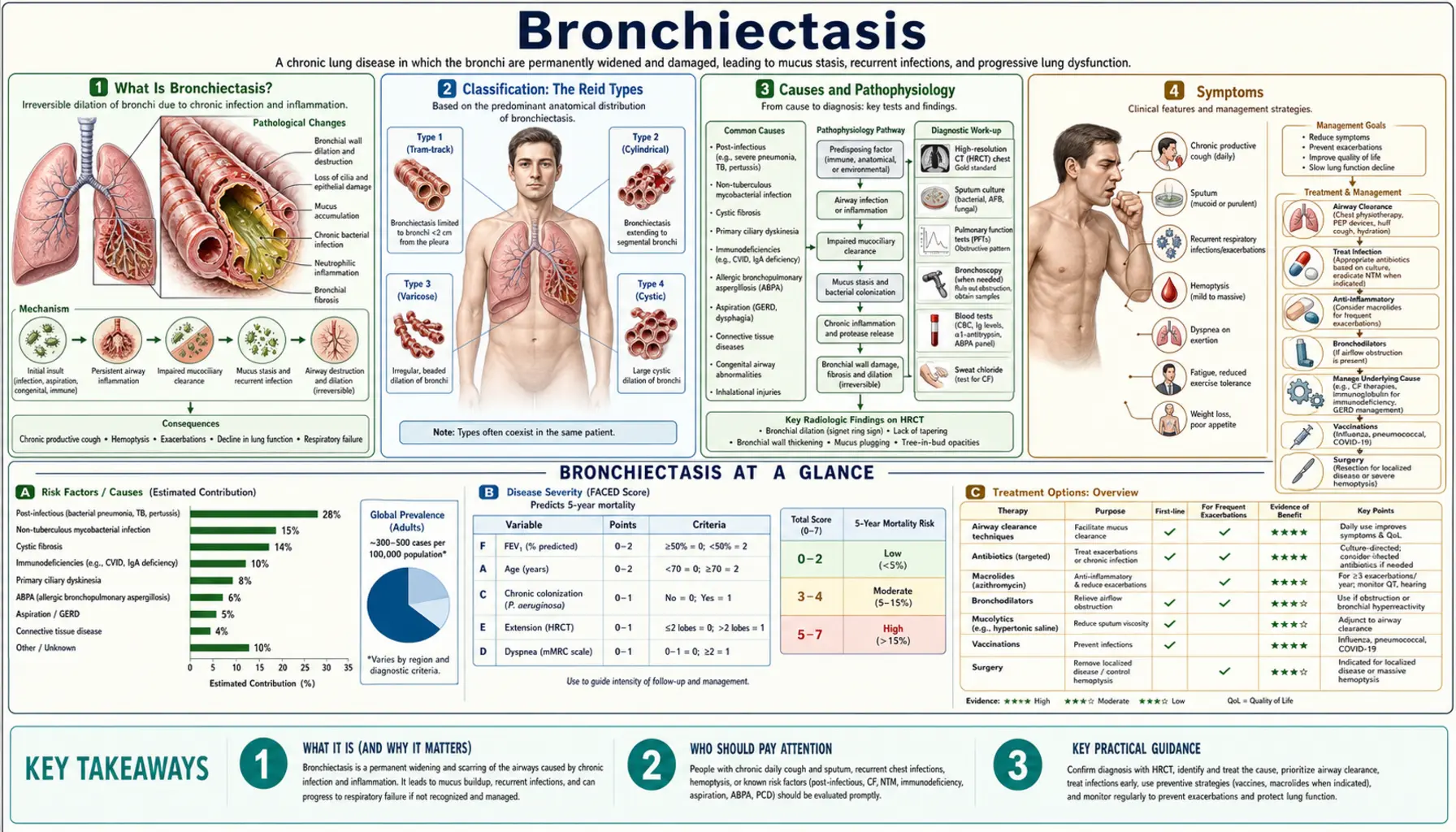
Table of Contents
- What Is Bronchiectasis?
- Classification (Reid Types)
- Causes and Pathophysiology
- Symptoms
- Diagnosis and Imaging
- Treatment
- Airway Clearance Therapy
- Natural and Lifestyle Approaches
- Complications
- Prognosis
- Key Research Papers
- Connections
- Featured Videos
What Is Bronchiectasis?
Bronchiectasis is a chronic lung condition in which the airways (bronchi) become permanently widened, thickened, and scarred — making it difficult or impossible for the lungs to clear mucus normally. The result is a vicious cycle: mucus pools in the dilated bronchi, bacteria colonize the stagnant secretions, repeated infections inflame the airway walls further, and the damage deepens. Patients typically have a daily productive cough, recurrent chest infections, and progressive breathlessness.
Unlike asthma or COPD, where airway narrowing is the central problem, bronchiectasis involves permanent structural destruction of airway walls — a distinction that shapes every treatment decision. Prevalence is rising worldwide, partly because better CT scanning is identifying cases that were previously missed or labeled as "recurrent bronchitis."
Classification: The Reid Types
The classic radiological classification comes from pathologist Lynne Reid (1950), who described three morphological patterns visible on bronchography and now identified by high-resolution CT (HRCT):
- Cylindrical (tubular): Airways are uniformly dilated with parallel walls. The mildest form; most amenable to treatment. Accounts for the majority of CT findings.
- Varicose: Irregular dilation with beaded, alternating narrowed and dilated segments — resembling a string of pearls on HRCT. Intermediate severity.
- Cystic (saccular): Severe ballooned dilation forming grape-like clusters at the airway ends. Associated with dense chronic infection and the poorest functional outcomes. Classic appearance in cystic fibrosis.
In practice, mixed patterns coexist within the same lung. The distribution (upper lobe, lower lobe, bilateral) provides diagnostic clues to the underlying cause.
Causes and Pathophysiology
Bronchiectasis is best understood as a final common pathway for many different insults to the airway wall. The key mechanism is a defect in mucociliary clearance: when mucus cannot be expelled, bacteria — especially Pseudomonas aeruginosa and Haemophilus influenzae — establish chronic colonies that trigger neutrophilic inflammation, releasing proteases (elastase, matrix metalloproteinases) that dissolve the structural proteins of the bronchial wall.
Known causes, grouped by frequency:
- Post-infectious (approx. 30%): Childhood pneumonia (especially pertussis, measles, tuberculosis, adenovirus), severe adult pneumonia. The most common identifiable cause globally.
- Cystic fibrosis (CF): CFTR gene mutation leading to thick, dehydrated mucus. CF causes bronchiectasis that is typically upper-lobe dominant.
- Immune deficiency: Common variable immunodeficiency (CVID), IgA deficiency, hypogammaglobulinemia — impaired antibody responses allow recurrent infections.
- Primary ciliary dyskinesia (PCD): Inherited defect in ciliary ultrastructure; impaired mucociliary clearance from birth. About 50% of PCD patients have situs inversus (Kartagener syndrome).
- Alpha-1-antitrypsin deficiency: Protease-antiprotease imbalance that directly damages airway walls.
- Allergic bronchopulmonary aspergillosis (ABPA): Hypersensitivity to Aspergillus species; causes central, upper-lobe bronchiectasis.
- Connective tissue disease: Rheumatoid arthritis (10–30% prevalence), Sjögren's syndrome, inflammatory bowel disease (especially ulcerative colitis).
- Idiopathic (up to 40%): No cause found despite thorough evaluation, particularly in older women — a phenotype sometimes called "Lady Windermere syndrome."
Symptoms
Symptoms range from mild daily cough in early disease to near-constant breathlessness and respiratory failure in advanced cases. Core features include:
- Chronic productive cough: Daily sputum production — the cardinal symptom. Volume often increases during exacerbations; color shifts from white/yellow to green or rust-brown with bacterial infection.
- Recurrent respiratory infections: Two or more chest infections per year requiring antibiotics is a common clinical threshold.
- Breathlessness: Initially only on exertion; becomes resting dyspnea in advanced disease.
- Wheeze and chest tightness: Particularly common in ABPA-related bronchiectasis and when CF coexists.
- Hemoptysis: Coughing blood — ranges from blood-streaked sputum to life-threatening massive hemoptysis from eroded bronchial arteries.
- Fatigue and reduced exercise tolerance: Chronic infection and hypoxia both contribute.
- Crackles and clubbing: Classic examination findings; digital clubbing suggests severe, long-standing disease.
Diagnosis and Imaging
Bronchiectasis is diagnosed by imaging — clinical symptoms alone are not sufficient. Standard spirometry showing FEV1/FVC obstruction does not reliably diagnose or exclude bronchiectasis; many patients have a normal or near-normal spirometry result.
- High-resolution CT (HRCT) of the thorax: The gold standard. Key findings:
- Signet-ring sign: Dilated bronchus (ring) appears larger than its accompanying pulmonary artery (stone) — the most reliable HRCT criterion for bronchiectasis.
- Bronchial wall thickening: Tram-track lines on axial cuts, indicating chronic inflammation.
- Mucus plugging: "Tree-in-bud" pattern of small-airway mucus filling.
- Lack of bronchial tapering: Normal bronchi narrow as they branch; dilated bronchi maintain their caliber.
- Sputum microbiology: Identify chronic colonizing organisms (especially Pseudomonas aeruginosa, which carries a worse prognosis). Send for culture and sensitivity at least annually and during every exacerbation.
- Lung function testing: Spirometry characterizes severity (FEV1) and tracks decline over time. Many patients show mixed obstructive-restrictive patterns.
- Cause-finding investigations: Serum immunoglobulins (CVID/IgA), sweat chloride/CFTR genotype (CF), ciliary biopsy or nasal nitric oxide (PCD), serum IgE + Aspergillus precipitins (ABPA), autoimmune panel (RA, Sjögren).
- Bronchoscopy: Reserved for localized disease to rule out foreign body or endobronchial tumor; not routine.
Treatment
There is no cure for bronchiectasis; treatment aims to reduce exacerbation frequency, preserve lung function, improve quality of life, and identify and treat any underlying cause.
Antibiotic therapy
- Acute exacerbations: Empiric antibiotic choice depends on prior sputum cultures. Amoxicillin or doxycycline for mild exacerbations with sensitive organisms; ciprofloxacin or antipseudomonal antibiotics (piperacillin-tazobactam, meropenem) for Pseudomonas colonization.
- Azithromycin prophylaxis: A landmark 2013 NEJM trial by Wong et al. (PMID 23427595) showed that azithromycin 500 mg three times per week reduced exacerbation rate by approximately 38% in patients with two or more exacerbations per year. Macrolide prophylaxis is now a guideline recommendation for frequent exacerbators; NTM colonization must be excluded before starting (azithromycin monotherapy risks resistance if MAC is present).
- Inhaled antibiotics: Tobramycin, colistin, or aztreonam inhalation solution for chronic Pseudomonas colonization — reduces bacterial load and reduces exacerbations in CF; evidence in non-CF bronchiectasis is more limited.
Mucoactive therapy
- Hypertonic saline (7%): Inhaled hypertonic saline hydrates airway surface liquid and facilitates mucus clearance; well tolerated with a pre-dose bronchodilator.
- Mannitol dry powder (Bronchitol): FDA-approved for CF; limited evidence in non-CF bronchiectasis.
- Dornase alfa (DNase): Effective in CF (cleaves extracellular DNA from neutrophils that thickens sputum); evidence of harm in non-CF bronchiectasis — avoid outside CF.
Bronchodilators
SABA (salbutamol) before airway clearance sessions and hypertonic saline; LABA/LAMA if airway obstruction is confirmed on spirometry.
Airway Clearance Therapy
Mechanical airway clearance is the cornerstone of daily self-management. Patients who perform daily airway clearance have fewer exacerbations, better sputum expectoration, and improved quality of life. Techniques include:
- Active cycle of breathing technique (ACBT): A structured breathing sequence — breathing control, thoracic expansion exercises, and the forced expiratory technique ("huffing") — to loosen and move mucus centrally without causing airway collapse.
- Oscillating positive expiratory pressure (OPEP) devices:
- Flutter valve: A pipe-like device with a stainless steel ball that creates oscillating back-pressure (6–20 Hz) during exhalation, mobilizing mucus via high-frequency vibration of airway walls.
- Aerobika (oscillating PEP): Provides adjustable PEP with oscillation; can be used with nebulizers simultaneously.
- Acapella: Spring-loaded counterrotating valve; can be used in any position, including supine — particularly useful for patients unable to sit upright.
- High-frequency chest wall oscillation (HFCWO): The "Vest" therapy — an inflatable jacket connected to a generator that oscillates the chest wall at 5–25 Hz, loosening mucus throughout the lung. Particularly used in CF and patients unable to perform independent airway clearance.
- Postural drainage: Gravity-assisted positioning (head-down, side-lying) to drain specific lung segments; less commonly used now but effective for localized disease.
Recommended frequency: at least once daily; twice daily during exacerbations. Sessions typically last 15–20 minutes.
Natural and Lifestyle Approaches
- Smoking cessation: Non-negotiable. Smoking impairs ciliary function, increases infection risk, and accelerates lung function decline.
- Vaccination: Annual influenza vaccine and pneumococcal vaccine (PCV15/PCV20) reduce infective exacerbation triggers. Pertussis booster where appropriate.
- Exercise and pulmonary rehabilitation: Aerobic exercise improves mucociliary clearance, reduces systemic inflammation, and improves exercise tolerance. Supervised pulmonary rehab is guideline-endorsed.
- Hydration: Adequate fluid intake (≥2 L/day unless restricted) maintains thin, mobile secretions.
- Nutrition: Underweight patients have worse outcomes; high-protein, calorie-adequate diet supports immune function and respiratory muscle strength.
- Anti-inflammatory diet: Limited evidence in bronchiectasis specifically, but Mediterranean-pattern diets reduce systemic neutrophilic inflammation, which drives airway wall damage.
- Vitamin D: Low serum 25(OH)D is associated with more frequent exacerbations; supplementation to maintain levels >50 nmol/L is reasonable.
- Avoiding respiratory irritants: Indoor air pollution, mold, chemical fumes all trigger bronchospasm and impair ciliary function.
Complications
- Massive hemoptysis: Erosion of enlarged bronchial arteries; can be life-threatening. Management: bronchial artery embolization (BAE) is preferred over surgery for acute massive bleeding.
- Respiratory failure: End-stage disease with hypoxemic and/or hypercapnic failure; may require long-term oxygen therapy or non-invasive ventilation (NIV).
- Cor pulmonale: Chronic hypoxia drives pulmonary vasoconstriction and right heart hypertrophy.
- Amyloidosis: Rare; chronic infection can deposit serum amyloid A protein in organs (kidneys, liver).
- Lung abscess: Localized suppuration within destroyed airway segments.
- Non-tuberculous mycobacteria (NTM) colonization: Mycobacterium avium complex (MAC) is a common opportunistic pathogen in bronchiectasis; it is both a complication and a potential cause of further airway damage.
Prognosis
Prognosis varies enormously by cause, severity, and whether the underlying condition is treatable. The BSI (Bronchiectasis Severity Index) scores FEV1, exacerbation history, chronic Pseudomonas colonization, BMI, and radiological extent to stratify patients into mild, moderate, and severe groups — with 4-year mortality ranging from 0–5% (mild) to >20% (severe).
Key prognostic factors:
- Pseudomonas aeruginosa chronic colonization: independently doubles mortality risk and triples exacerbation rate.
- Rate of FEV1 decline (normal ~30 mL/year; faster with frequent infections).
- Number of exacerbations per year (≥3 per year is high-risk).
- Underlying cause: CF and severe immune deficiency carry worst prognosis; post-infectious cylindrical bronchiectasis in otherwise healthy adults can be stable for decades.
- Response to treatment of the underlying cause: ABPA dramatically improves with antifungal + steroid therapy; immunoglobulin replacement in CVID markedly reduces exacerbation rate.
Lung transplantation remains an option for end-stage disease, particularly in younger patients with CF.
Key Research Papers
- Search PubMed — Azithromycin for prevention of exacerbations in non-cystic-fibrosis bronchiectasis (randomized trial); 3×/week azithromycin reduced exacerbation rate by 38%.
- Search PubMed — Validation of the Bronchiectasis Severity Index (BSI) across seven European cohorts; predicts 4-year mortality and hospitalisation.
- Search PubMed — ERS guidelines on management of adult bronchiectasis; comprehensive evidence synthesis.
- Search PubMed — Systematic investigation of causes of bronchiectasis in 150 adults; post-infectious 29%, immune deficiency 11%, ABPA 9%, idiopathic 41%.
- Search PubMed — Oscillating positive expiratory pressure (OPEP) vs active cycle of breathing for airway clearance in bronchiectasis; non-inferiority demonstrated.
- Search PubMed — Pseudomonas aeruginosa colonization in bronchiectasis independently predicts mortality; retrospective multicentre analysis.
- Search PubMed — Hypertonic saline improves sputum clearance and quality of life in non-CF bronchiectasis; randomized trial.
- Search PubMed — Spanish SEPAR guidelines on bronchiectasis etiology, diagnosis, and treatment.
- Search PubMed — Non-tuberculous mycobacteria in bronchiectasis: prevalence, clinical impact, and management challenges.
- Search PubMed — Original description of the cylindrical/varicose/saccular (cystic) classification of bronchiectasis based on pathological anatomy; foundation of all subsequent radiological classification.
- Search PubMed — European Respiratory Society clinical practice guidelines for the management of adult bronchiectasis.
- Search PubMed — British Thoracic Society guideline for bronchiectasis in adults (2019 revision); practical framework for diagnosis, monitoring, and treatment.
PubMed Topic Searches
- PubMed: bronchiectasis
- PubMed: bronchiectasis exacerbation treatment
- PubMed: bronchiectasis airway clearance
- PubMed: bronchiectasis Pseudomonas aeruginosa
- PubMed: azithromycin bronchiectasis prophylaxis
- PubMed: bronchiectasis HRCT imaging
- PubMed: bronchiectasis primary ciliary dyskinesia
- PubMed: non-cystic fibrosis bronchiectasis management
Connections
- Pulmonology
- COPD
- Cystic Fibrosis
- Pneumonia
- Asthma
- Bronchitis
- Interstitial Lung Disease
- Pulmonary Fibrosis
- Sarcoidosis
- Alpha-1-Antitrypsin Deficiency
- Pulmonary Embolism
- Influenza
- Pulmonary Hypertension
- Vitamin D3
- Magnesium
- Mullein