Visceral Larva Migrans (Toxocara)
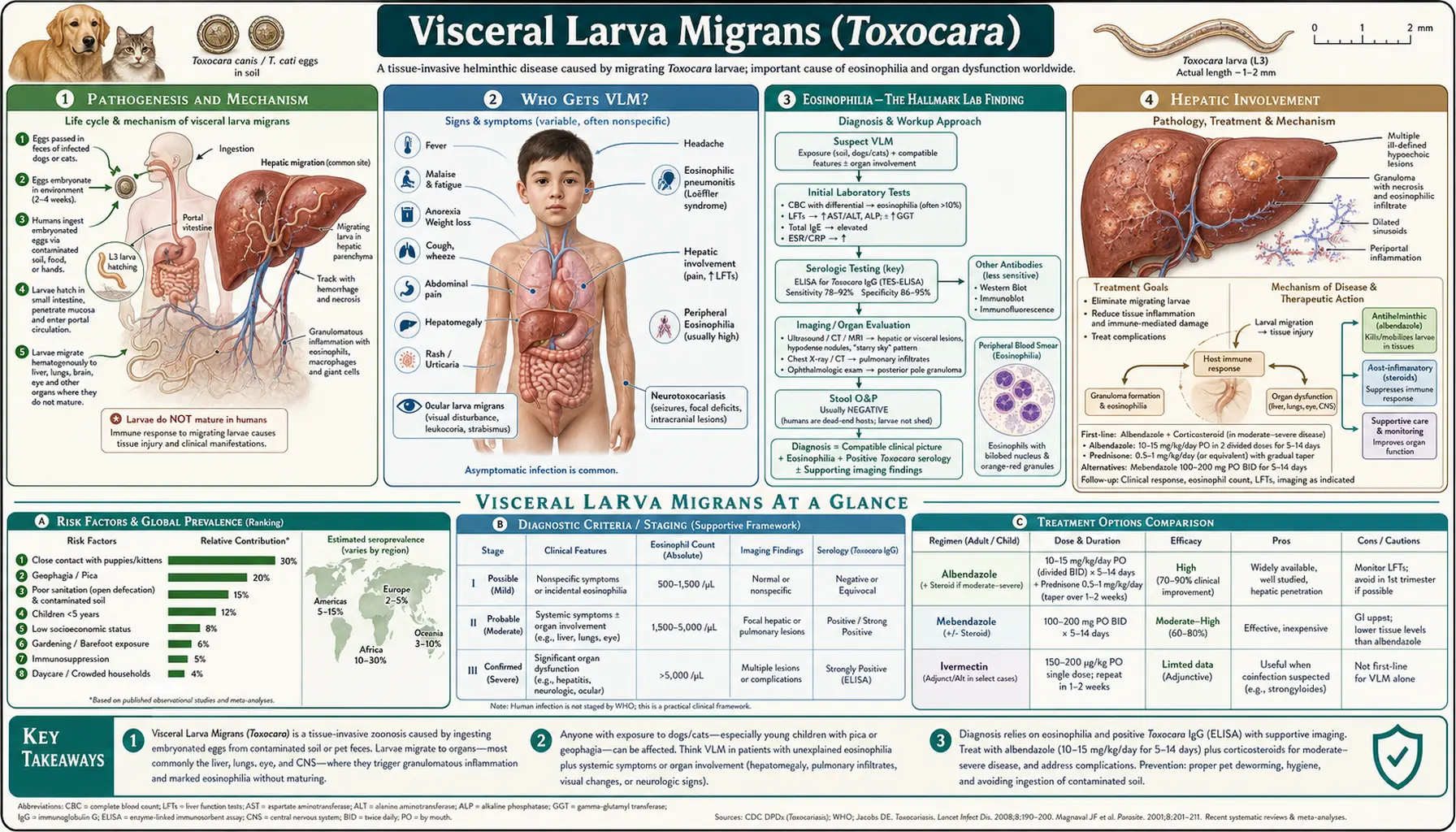
Visceral larva migrans (VLM) is the most common clinical form of toxocariasis, occurring predominantly in young children aged 1–7 after ingestion of large numbers of Toxocara eggs from contaminated soil or sandboxes. Larvae hatch, penetrate the gut wall, and migrate through the liver, lungs, and other organs, triggering intense eosinophilic granulomatous inflammation. The hallmark is profound persistent eosinophilia, sometimes reaching 30–80% of the white blood cell differential.
Table of Contents
- Pathogenesis and Mechanism
- Who Gets VLM
- Eosinophilia — The Hallmark Lab Finding
- Hepatic Involvement
- Pulmonary Involvement
- Systemic Symptoms
- Covert Toxocariasis — The Mild Adult Form
- Neurotoxocariasis and Cardiac Involvement
- Key Research Papers
- Connections
- Featured Videos
1. Pathogenesis and Mechanism
After a child ingests embryonated Toxocara eggs — typically from contaminated sandbox sand, garden soil, or dirty hands — the eggs hatch in the small intestine, releasing second-stage larvae (L2). These larvae, roughly 400 µm long, penetrate the intestinal mucosa and enter the portal circulation.
From the portal vein, larvae enter the liver sinusoids and lodge in hepatic tissue, where they begin their migratory path through parenchyma. Many larvae are trapped in the liver; others escape into the hepatic veins and reach the right heart, then the pulmonary circulation, where some are trapped in capillaries while others traverse the lung and spread systemically via the arterial circulation to virtually any organ — brain, eye, heart, muscles, kidneys.
As larvae migrate, they leave behind a trail of eosinophilic granulomas: aggregations of eosinophils, macrophages, lymphocytes, and multinucleated giant cells surrounding the dying or encapsulated larva. These granulomas are the histological hallmark of VLM. The immune response also produces massive peripheral eosinophilia, elevated IgE, and hypergammaglobulinemia as hallmarks of the systemic response.
2. Who Gets VLM
VLM requires ingestion of a substantial egg burden — the disease is generally associated with heavy exposure. The typical patient is:
- A child aged 1–7 years with pica (compulsive soil or non-food ingestion), or regular play in contaminated sandboxes or yards
- Living in close contact with dogs, particularly puppies, which carry the heaviest Toxocara canis egg burdens
- Residing in low-income communities where veterinary deworming is inconsistent and environmental contamination is higher
- Occasionally adults who consumed raw or undercooked animal liver (associated with VLM outbreaks in Japan from raw chicken liver)
Boys may be more commonly affected than girls due to higher likelihood of outdoor soil play and pica behaviors. African American children in the southeastern US have the highest documented seroprevalence, reflecting environmental and socioeconomic exposure gradients.
3. Eosinophilia — The Hallmark Lab Finding
The single most important laboratory clue to VLM is persistent eosinophilia. In VLM:
- Eosinophil percentage typically ranges from 30–80% of the white blood cell differential
- Absolute eosinophil counts may reach 5,000–30,000 cells/µL (normal <500/µL)
- Eosinophilia persists for weeks to months, distinguishing VLM from transient reactive eosinophilia
- Elevated total serum IgE (often markedly elevated, sometimes >1,000 IU/mL)
- Hypergammaglobulinemia — particularly elevated IgG and IgM
- Isohemagglutinin titers (anti-A and anti-B) are characteristically elevated due to cross-reactive antigens
Eosinophilia is a reactive response to larval excretory-secretory products and is driven by IL-5 produced by Th2-polarized T cells. The degree of eosinophilia roughly correlates with worm burden. Crucially, eosinophilia is characteristically absent or mild in ocular larva migrans (OLM), which helps distinguish the two syndromes clinically.
4. Hepatic Involvement
The liver is the primary target organ in VLM because larvae from the portal circulation first traverse the liver before escaping systemically. Hepatic involvement produces:
- Hepatomegaly — enlarged, sometimes tender liver on examination
- Elevated transaminases (AST, ALT) — reflecting hepatocyte damage from migrating larvae
- Abdominal pain — right upper quadrant or diffuse
- Liver ultrasound findings — hypoechoic nodules corresponding to eosinophilic granulomas; a characteristic "flower" or "target" pattern of multiple small nodules is considered pathognomonic when present
- CT scan — multiple low-density (hypodense) lesions, non-enhancing or with peripheral enhancement
Liver histology (when biopsy is performed) shows eosinophilic granulomas with central necrosis and larval remnants. In practice, biopsy is rarely necessary — clinical presentation plus serology and imaging is usually sufficient for diagnosis. Hepatic granulomas typically resolve completely over months as the inflammatory response subsides after larval death.
5. Pulmonary Involvement
Pulmonary VLM occurs when larvae traverse the liver and enter the pulmonary circulation. Symptoms and findings include:
- Cough — often prominent, persistent, sometimes nocturnal
- Wheeze and bronchospasm — mimicking asthma; larval migration causes airway hyperresponsiveness
- Dyspnea — in severe cases with extensive pulmonary infiltration
- Transient pulmonary infiltrates on chest X-ray — bilateral patchy opacities resembling Löffler syndrome (eosinophilic pneumonia); may migrate from day to day
- BAL eosinophilia — eosinophilic alveolitis on bronchoalveolar lavage
The pulmonary phase of VLM resembles Löffler syndrome, a pattern of transient pulmonary infiltrates with eosinophilia that can also be caused by other migrating helminths (Ascaris, Strongyloides, hookworm). The history of animal exposure and serology distinguish toxocariasis. Pulmonary VLM responds well to albendazole and typically resolves without permanent lung damage.
6. Systemic Symptoms
Beyond the liver and lungs, VLM produces constitutional and systemic manifestations:
- Prolonged fever — low-grade to moderate, lasting weeks
- Malaise and fatigue — significant in many children, limiting activity
- Urticaria (hives) — recurrent skin rashes driven by IgE-mediated hypersensitivity and histamine release
- Lymphadenopathy — generalized or regional lymph node enlargement
- Splenomegaly — in some patients alongside hepatomegaly
- Anemia — mild normocytic anemia from chronic inflammation
- Elevated ESR and CRP — markers of systemic inflammation
The combination of fever, hepatomegaly, hypereosinophilia, and elevated IgE in a young child with pet or soil exposure is highly characteristic of VLM. The differential diagnosis includes other causes of hypereosinophilia with organ involvement: Löffler syndrome from other helminths, hypereosinophilic syndrome, drug reactions, and eosinophilic granulomatosis with polyangiitis (formerly Churg-Strauss).
7. Covert Toxocariasis — The Mild Adult Form
Covert toxocariasis is a subclinical or mildly symptomatic form seen in older children and adults with lower-level exposure. It does not meet the classic criteria for VLM but produces recognizable features:
- Mild eosinophilia (500–2,000/µL) without systemic disease
- Asthma or reactive airway disease — epidemiological studies document a link between Toxocara seropositivity and increased asthma risk
- Recurrent urticaria
- Chronic abdominal discomfort
- Headache and fatigue without a neurological diagnosis
The concept of covert toxocariasis is important because it may explain a proportion of chronic unexplained eosinophilia or atopic disease in adults with pet or soil exposure. Treatment with albendazole is generally recommended when eosinophilia exceeds 1,000/µL and symptoms are present, even without full VLM syndrome.
8. Neurotoxocariasis and Cardiac Involvement
Rare but serious manifestations of VLM occur when larvae reach critical organs:
Neurotoxocariasis presents as eosinophilic meningitis (headache, CSF pleocytosis with eosinophils), encephalitis, seizures, or behavioral changes. Brain MRI shows white matter lesions and migratory tracts. CSF serology for Toxocara antibodies supports diagnosis. Treatment requires extended albendazole (21 days) plus corticosteroids.
Cardiac toxocariasis produces eosinophilic myocarditis with arrhythmias, cardiomegaly, and in severe cases, heart failure. Troponin elevation and ECG changes may be present. Cardiac MRI with late gadolinium enhancement demonstrates myocardial involvement. Both neurotoxocariasis and cardiac involvement are markers of very heavy larval burden and require aggressive treatment. Fatal cases, while rare, have been reported with massive VLM and cardiac or neurological compromise.
Key Research Papers
- Rubinsky-Elefant G, et al. Human toxocariasis: diagnosis, worldwide seroprevalences and clinical expression. — Search PubMed
- Despommier D. Toxocariasis: clinical aspects, epidemiology, medical ecology, and molecular aspects. — Search PubMed
- Won KY, et al. National seroprevalence and risk factors for zoonotic Toxocara spp. infection. — Search PubMed
- Fillaux J, Magnaval JF. Laboratory diagnosis of human toxocariasis. — Search PubMed
- Beaver PC, et al. Chronic eosinophilia due to visceral larva migrans. — Search PubMed
- Magnaval JF, et al. Highlights of human toxocariasis. — Search PubMed
- Pawlowski Z. Toxocariasis in humans: clinical expression and treatment dilemma. — Search PubMed
- Woodhall D, et al. Neglected parasitic infections in the US: toxocariasis. — Search PubMed
- Iddawela DR, et al. Seroprevalence of toxocariasis. — Search PubMed
- Finsterer J, Auer H. Neurotoxocarosis. — Search PubMed
PubMed Searches
- VLM eosinophilia
- Toxocara hepatic granuloma
- Toxocara pulmonary Loeffler
- Neurotoxocariasis meningitis
- Covert toxocariasis asthma IgE
- Toxocara myocarditis cardiac
Connections
- Toxocara Symptoms Overview
- Ocular Larva Migrans
- Diagnosis: ELISA and Imaging
- Albendazole Treatment
- Prevention and Pet Hygiene
- Toxocara Overview
- Ascaris
- All Parasites