Toxocara Treatments
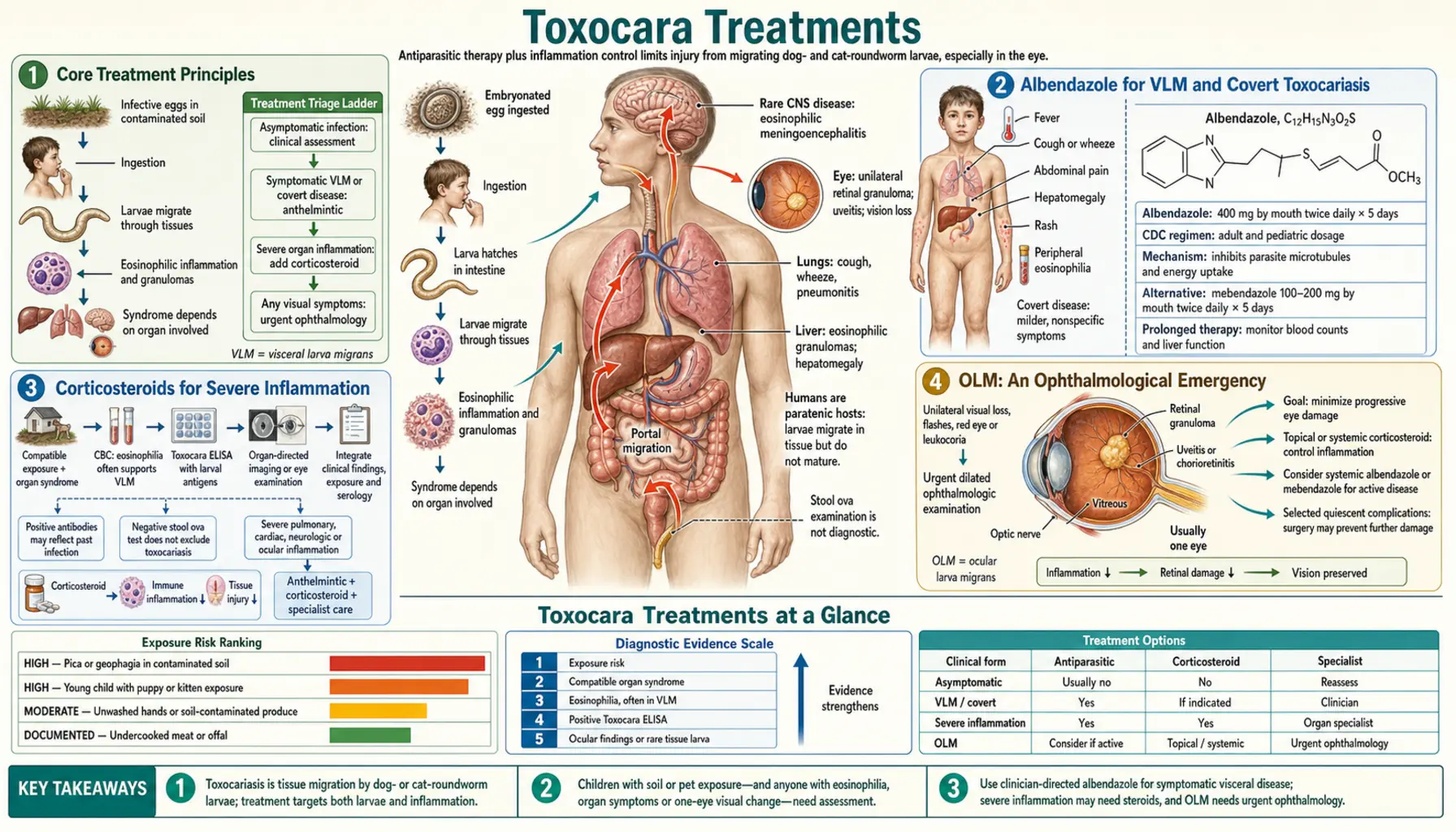
Toxocariasis treatment depends on which syndrome is present: visceral larva migrans (VLM), ocular larva migrans (OLM), covert toxocariasis, or neurotoxocariasis. Albendazole is the antiparasitic of choice for systemic disease. OLM is an ophthalmological emergency managed primarily with steroids and surgical intervention — antiparasitic drugs play a limited and carefully timed role. Prevention through regular pet deworming is the most impactful intervention at the population level.
Table of Contents
- Core Treatment Principles
- Albendazole for VLM and Covert Toxocariasis
- Corticosteroids for Severe Inflammation
- OLM: An Ophthalmological Emergency
- Neurotoxocariasis Treatment
- Treating Asymptomatic Seropositive Individuals
- Follow-Up and Monitoring
- Prevention Overview
- Key Research Papers
- Connections
- Featured Videos
1. Core Treatment Principles
Treatment of toxocariasis is guided by two overarching principles:
- Kill the larvae — antiparasitic drugs (primarily albendazole) target migrating larvae to halt tissue damage and systemic inflammation
- Control the inflammatory response — corticosteroids are added when inflammation itself threatens organ function, because a dying larva can trigger an intensified eosinophilic reaction that may cause more harm than the living larva
These two principles sometimes conflict — in OLM, the decision about whether and when to give antiparasitic drugs requires careful ophthalmological judgment, because killing a larva in or near the fovea may trigger a destructive inflammatory flare. The treating approach therefore differs substantially between VLM (treat antiparasitically, add steroids if severe) and OLM (steroids first, antiparasitic drugs used selectively).
Most uncomplicated VLM is self-limited and resolves without treatment over weeks to months. Treatment is recommended for all symptomatic VLM and for asymptomatic cases with eosinophilia exceeding 1,000/µL. OLM always requires specialist management.
2. Albendazole for VLM and Covert Toxocariasis
Albendazole is the preferred antiparasitic agent for VLM, covert toxocariasis, and neurotoxocariasis. It is a benzimidazole carbamate that inhibits tubulin polymerization in nematode cells, disrupting microtubule assembly and killing larvae. Key advantages over the alternative (mebendazole) include superior tissue penetration and higher oral bioavailability when taken with a fatty meal.
Standard regimen for VLM and covert toxocariasis:
- Albendazole 400 mg orally twice daily for 5 days
- Children under 20 kg: 7.5 mg/kg twice daily (max 400 mg per dose)
- Take with food (fat enhances absorption of albendazole)
Response to treatment: eosinophilia typically begins to fall within 1–2 weeks of completing the course. Liver lesions on ultrasound resolve over weeks to months. A second course may be given if symptoms persist after 4–6 weeks or if eosinophilia rebounds. For detailed dosing, drug interactions, side effects, and extended regimens for neurotoxocariasis, see the Albendazole Treatment page.
3. Corticosteroids for Severe Inflammation
Corticosteroids are added to antiparasitic therapy when inflammation poses a risk to critical organs:
- Pulmonary VLM with hypoxia or extensive infiltrates — prednisone 0.5–1 mg/kg/day to reduce airway inflammation
- Neurotoxocariasis — high-dose steroids (IV methylprednisolone in severe cases) alongside albendazole
- Cardiac toxocariasis — steroids to reduce myocardial inflammation
- Severe hepatic VLM with significant transaminase elevation
In VLM, corticosteroids and albendazole can be given simultaneously. The concern about inflammatory surge from larval death (relevant in OLM) is less critical in systemic VLM because larvae are scattered across multiple organs, and the systemic immune response is already highly active. Standard prednisone dosing is 0.5–1 mg/kg/day (max 40–60 mg/day), tapered over 2–4 weeks as symptoms resolve.
4. OLM: An Ophthalmological Emergency
Ocular larva migrans requires urgent referral to an ophthalmologist experienced in managing intraocular parasitic disease. The goals of OLM treatment are:
- Control intraocular inflammation to preserve vision
- Eliminate the larva when possible (laser, surgery)
- Manage structural complications (retinal detachment, cataract, vitritis)
Antiparasitic drugs (albendazole) are NOT given routinely for OLM and should only be used with ophthalmological guidance. If the larva is already dead when the patient presents, antiparasitic drugs serve no purpose. If the larva is alive, killing it pharmacologically may trigger an acute inflammatory surge that worsens vision. The decision requires specialist judgment based on larva viability assessment.
For comprehensive OLM management including laser photocoagulation, pars plana vitrectomy, intravitreal treatments, and the critical leukocoria/retinoblastoma distinction, see the Ocular Toxocariasis Treatment page.
5. Neurotoxocariasis Treatment
CNS involvement requires more intensive treatment than uncomplicated VLM:
- Albendazole extended course — 21 days (vs. 5 days for VLM) to achieve adequate CNS penetration and sustained antiparasitic effect
- Corticosteroids — high-dose, often IV methylprednisolone initially, then oral prednisone taper; essential to control eosinophilic meningitis and prevent cerebral edema
- Seizure management — antiepileptic drugs as needed for seizure control
- Neuroimaging follow-up — repeat MRI to assess lesion resolution
- Repeat albendazole courses may be necessary for recurrent or persistent neurological disease
Prognosis is generally favorable with prompt treatment, but neurological sequelae (cognitive changes, behavioral problems) can persist after severe cases. Neurotoxocariasis in immunocompromised patients may follow a more aggressive course.
6. Treating Asymptomatic Seropositive Individuals
The decision to treat an asymptomatic seropositive individual is debated. Practical guidelines:
- Asymptomatic + eosinophilia >1,000/µL: treat with albendazole 5-day course; eosinophilia at this level suggests active larval migration with ongoing tissue injury
- Asymptomatic + eosinophilia <1,000/µL: watchful waiting is appropriate; most clinicians do not treat
- Asymptomatic seropositive with no eosinophilia: past infection with larval death; treatment is not indicated
- Seropositive + unexplained atopic symptoms (asthma, urticaria): consider treatment even with mild eosinophilia, given evidence linking toxocariasis to chronic atopic disease
Children with pica and high-risk exposures who are seropositive with any eosinophilia should receive treatment given the risk of ongoing heavy egg ingestion and escalating worm burden.
7. Follow-Up and Monitoring
After treatment of VLM or covert toxocariasis:
- Repeat CBC with differential at 4–6 weeks: eosinophil count should fall toward normal
- Repeat liver function tests if initially abnormal
- Repeat liver ultrasound at 3 months to document granuloma resolution
- Repeat Toxocara serology is not useful in the short term — antibody titers fall slowly over months to years and do not reliably reflect treatment success
- If eosinophilia persists or rebounds at 6–8 weeks, consider re-exposure (ongoing pet contact without pet deworming) and retreatment
For OLM, ophthalmological follow-up every 3–6 months is recommended for at least 2 years, as delayed inflammatory reactivation can occur. Children treated for OLM should have visual acuity monitoring and amblyopia treatment if strabismus or visual deprivation is present.
8. Prevention Overview
Prevention of toxocariasis is the highest-impact intervention, since the disease primarily affects children who cannot protect themselves. The cornerstone of prevention is regular anthelmintic deworming of pet dogs and cats, especially puppies and kittens, which eliminates the source of environmental egg contamination.
Key prevention measures:
- Deworm puppies starting at 2 weeks, every 2 weeks until 8 weeks, monthly until 6 months
- Deworm adult dogs and cats at least 4 times per year
- Pick up dog feces within 24 hours (before eggs embryonate)
- Cover sandboxes when not in use
- Teach children to wash hands after outdoor play
- Address pica in children (assess for iron deficiency)
For comprehensive guidance on pet deworming schedules, sandpit hygiene, community prevention strategies, and the biology of egg survival, see the Prevention and Pet Hygiene page.
Key Research Papers
- Rubinsky-Elefant G, et al. Human toxocariasis: diagnosis, worldwide seroprevalences and clinical expression. — Search PubMed
- Despommier D. Toxocariasis: clinical aspects, epidemiology, medical ecology, and molecular aspects. — Search PubMed
- Won KY, et al. National seroprevalence and risk factors for Toxocara spp. — Search PubMed
- Magnaval JF, et al. Highlights of human toxocariasis. — Search PubMed
- Fillaux J, Magnaval JF. Laboratory diagnosis of human toxocariasis. — Search PubMed
- Pawlowski Z. Toxocariasis in humans: clinical expression and treatment dilemma. — Search PubMed
- Beaver PC, et al. Chronic eosinophilia due to visceral larva migrans. — Search PubMed
- Woodhall D, et al. Neglected parasitic infections in the US: toxocariasis. — Search PubMed
- Iddawela DR, et al. Seroprevalence of toxocariasis. — Search PubMed
- Finsterer J, Auer H. Neurotoxocarosis. — Search PubMed
PubMed Searches
- Albendazole toxocariasis treatment
- Toxocara corticosteroids VLM
- Ocular toxocariasis management
- Neurotoxocariasis treatment
- Toxocara prevention deworming
- Asymptomatic toxocara eosinophilia treatment
Connections
- All Parasites
- Albendazole Treatment
- Ocular Toxocariasis Treatment
- Prevention and Pet Hygiene
- Toxocara Symptoms
- Visceral Larva Migrans
- Ocular Larva Migrans
- Toxocara Overview