Cluster Headaches
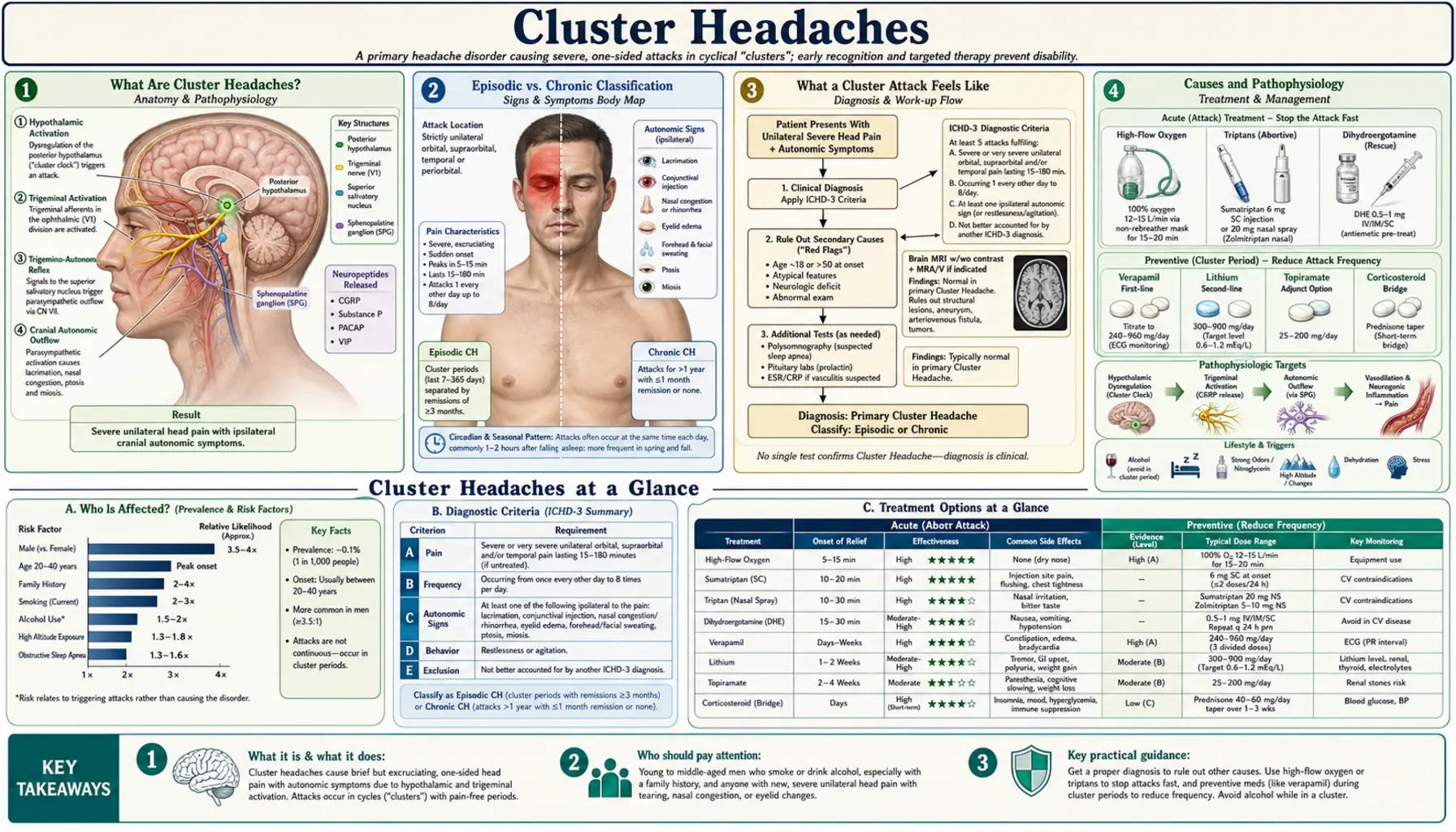
Table of Contents
- What Are Cluster Headaches?
- Episodic vs. Chronic Classification
- What a Cluster Attack Feels Like
- Causes and Pathophysiology
- Triggers
- Diagnostic Criteria (ICHD-3)
- Acute Treatment
- Preventive Treatment
- Natural and Lifestyle Approaches
- Complications
- Key Research Papers
- Connections
- Featured Videos
What Are Cluster Headaches?
Cluster headaches are one of the most painful conditions known to medicine — often called "suicide headaches" by patients because of the intensity. They occur in bouts (clusters) lasting weeks to months, separated by remission periods that can last months to years. Each individual attack is brief (15 minutes to 3 hours) but excruciatingly intense, striking one side of the head around or behind one eye.
About 1 in 1,000 people are affected; men are affected 3–5 times more often than women. Despite being classified as a primary headache disorder by the International Headache Society (IHS), cluster headaches are far less researched than migraine. Many patients wait years before receiving an accurate diagnosis, often being told they have migraines, sinus infections, or dental problems.
Episodic vs. Chronic Classification
Cluster headaches fall into two main types based on how remission periods behave:
- Episodic cluster headaches (most common, ~85%): Cluster periods typically last 6–12 weeks, often occurring at the same time of year — spring and autumn are common. Remission periods last at least 3 months between clusters. Many patients develop a reliable seasonal pattern over years.
- Chronic cluster headaches (~15%): Attacks occur for more than 1 year without a remission period of 3 months or longer. The chronic form is harder to treat and associated with greater disability. A small number of episodic patients transition to chronic over time.
The distinction matters for treatment planning. Episodic patients may be managed with short-course prevention during each cluster period. Chronic patients typically require long-term preventive therapy.
What a Cluster Attack Feels Like
The pain of a cluster headache is excruciating, unilateral, and strictly one-sided — centered in or around the eye, temple, or forehead. Patients most commonly describe it as a hot poker or ice pick being driven behind the eye. It builds rapidly to peak intensity within 15 minutes (unlike migraine, which builds over hours) and lasts anywhere from 15 minutes to 3 hours.
Several distinguishing features set cluster attacks apart:
- Restlessness and agitation: Patients pace, rock, or bang their head. This is the opposite of migraine, where lying still in a dark room helps. A person writhing in pain despite the severity is a strong diagnostic clue.
- Autonomic symptoms on the same side as the pain: drooping eyelid (ptosis), small pupil (miosis), tearing and red eye, nasal congestion or runny nose, forehead and facial sweating.
- Circadian pattern: Attacks frequently occur at the same time of day, often 1–2 hours after falling asleep. This "alarm clock" quality is a hallmark of cluster headaches.
- During a cluster period: 1–8 attacks per day are typical. Between attacks, patients feel completely normal — there is no migraine-like prodrome, postdrome, or ongoing sensitivity.
Causes and Pathophysiology
The exact cause of cluster headaches is not fully understood, but research has identified the key players:
- Hypothalamus as pacemaker: The posterior hypothalamus is implicated as the "biological clock" driving cluster headaches, explaining their remarkable circadian and circannual periodicity. Deep brain stimulation of this region reduces attack frequency in medically refractory patients. Neuroimaging during attacks consistently shows hypothalamic activation.
- Trigeminal nerve and autonomic arc: The trigeminal nerve (cranial nerve V) generates the intense pain, while its connection to the pterygopalatine ganglion via the cranial autonomic reflex arc produces the ipsilateral autonomic symptoms — tearing, nasal congestion, ptosis.
- Circadian hormone disruption: Changes in melatonin and cortisol secretion timing correlate with cluster periods. Melatonin levels are blunted during active cluster periods.
- Genetic predisposition: Family history increases risk approximately 14-fold. Variants in the HCRTR2 gene (orexin receptor 2) have been implicated, linking the disorder to the same hypothalamic wake-sleep signaling system.
Triggers
An important distinction: triggers only precipitate individual attacks during an active cluster period. They do not cause a cluster period to begin, and they do not trigger attacks during remission. This is a key diagnostic clue — a patient who drinks alcohol freely without headache during remission but gets an attack within 30 minutes of one drink during a cluster period almost certainly has cluster headaches.
Common triggers during a cluster period:
- Alcohol — the most reliable trigger; even small amounts can precipitate an attack within 30–60 minutes
- Nitroglycerin — used in research to reliably provoke attacks for study purposes
- Strong smells — perfumes, gasoline, paint fumes
- High altitude — reduced oxygen availability appears to lower the threshold
- Overheating — hot showers, exercise, hot weather
- Disrupted sleep schedule — shift work, jet lag, daytime napping during a cluster period
Diagnostic Criteria (ICHD-3)
The International Classification of Headache Disorders, 3rd edition (ICHD-3) defines cluster headaches by the following criteria. All must be met:
- Severe or very severe unilateral orbital, supraorbital, and/or temporal pain lasting 15–180 minutes (if untreated)
- At least one of the following ipsilateral (same side as pain) autonomic features: conjunctival injection and/or lacrimation, nasal congestion and/or rhinorrhea, eyelid edema, forehead and facial sweating, forehead and facial flushing, sensation of fullness in the ear, miosis and/or ptosis — OR a sense of restlessness or agitation
- Attacks occur from 1 every other day to 8 per day for more than half of the time when the disorder is active
- Not better accounted for by another ICHD-3 diagnosis
Imaging: MRI brain with pituitary protocol is indicated at initial diagnosis to exclude secondary causes. Pituitary adenomas can cause pain and autonomic features that closely mimic cluster headaches — this diagnosis must be excluded before assuming the headaches are primary.
Acute Treatment
Because cluster attacks build to peak intensity within 15 minutes, oral medications are almost always too slow. Acute treatments must be fast-acting:
- High-flow oxygen (first-line): 100% O2 at 12–15 L/min via a non-rebreather mask for 15–20 minutes aborts attacks in approximately 70% of patients. It is safe, has no significant side effects, and can be used multiple times per day. It requires a prescription for a home oxygen concentrator or cylinder — advocating for this with your doctor is worthwhile.
- Sumatriptan 6 mg subcutaneous injection: The fastest pharmaceutical option, effective in 74–80% of attacks within 15 minutes. The auto-injector form is practical during attacks. Sumatriptan nasal spray (20 mg) is slower but still effective.
- Zolmitriptan nasal spray 5 mg: An alternative to sumatriptan nasal spray with good evidence.
- Intranasal lidocaine 4–10%: Applied with the head tilted back and toward the affected side; can abort attacks within minutes by blocking the sphenopalatine ganglion. Underused but effective for patients who cannot tolerate triptans.
- Avoid oral medications: Oral triptans, oral analgesics, and oral NSAIDs are too slow to be useful for attacks that peak in 15 minutes. This is a common reason cluster headache patients feel undertreated.
Preventive Treatment
Prevention is the cornerstone of cluster headache management — reducing attack frequency, shortening the cluster period, and in some cases preventing the next cluster period entirely:
- Verapamil (first-line prevention): 240–960 mg/day in divided doses; the most widely used preventive. Requires regular ECG monitoring for cardiac conduction side effects (PR interval prolongation). Takes 2–3 weeks to reach full effect, which is why bridging therapy is often needed.
- Lithium carbonate: Particularly effective for chronic cluster headaches; requires regular monitoring of lithium blood levels, renal function, and thyroid function. Narrow therapeutic window.
- Corticosteroids (bridge/transition treatment): Prednisone 60 mg tapered over 2–3 weeks provides rapid short-term reduction in attacks while verapamil takes effect. Not suitable for long-term use due to side effects, but very useful for episodic patients at the start of a cluster period.
- Melatonin 10–15 mg at night: Evidence-supported and well-tolerated; leverages the hypothalamic circadian mechanism directly. Useful adjunct, especially for nocturnal attacks.
- Galcanezumab (Emgality) 300 mg injection: A CGRP monoclonal antibody approved specifically for episodic cluster headaches — the first genuinely new treatment mechanism in decades. One injection at the start of a cluster period reduces weekly attack frequency significantly.
- Greater occipital nerve (GON) block: Ipsilateral corticosteroid injection at the base of the skull; rapid onset (within days), effective bridge therapy while oral preventives take effect.
- Deep brain stimulation (DBS): Reserved for medically refractory chronic cluster headache patients. Targets the posterior hypothalamus. Significant improvement in a meaningful proportion of otherwise untreatable patients.
Natural and Lifestyle Approaches
Several non-pharmaceutical strategies have meaningful evidence or strong patient-community support:
- Melatonin 10 mg nightly at bedtime: During cluster periods, nightly melatonin reduces nocturnal attack frequency by acting directly on the hypothalamic circadian disruption underlying cluster headaches. Well-tolerated with minimal side effects.
- Capsaicin intranasal cream: Daily application to the ipsilateral nostril desensitizes trigeminal nociceptors over time. Small clinical trials show reduction in attack frequency. The initial burning is uncomfortable but subsides with continued use.
- Complete alcohol avoidance during cluster periods: Non-negotiable during an active cluster — even small amounts reliably trigger attacks in most patients.
- Maintaining a strict sleep schedule: Stabilizing the sleep-wake cycle helps regulate the hypothalamic circadian disruption. Avoiding daytime naps and keeping consistent bed and wake times during a cluster period is recommended.
- Vitamin D: Anti-inflammatory; some cluster headache patients report correlation between low vitamin D levels and more severe or prolonged cluster periods. Supplementation is low-risk and worth considering, particularly in northern latitudes.
- Omega-3 fatty acids: Anti-inflammatory properties may modestly reduce neuroinflammatory burden. No cluster-specific trials, but general evidence for headache reduction.
- Psilocybin (research context only): Cluster headache patient communities have self-reported benefit for decades, predating mainstream psychedelic research. Emerging clinical trial evidence suggests sub-perceptual doses may interrupt cluster periods. The mechanism may involve serotonin 5-HT2A receptor modulation in the hypothalamus. This is not a recommendation to self-treat — psilocybin remains a controlled substance, and use outside formal medical supervision carries significant risks.
Complications
- Suicidal ideation during attacks: The "suicide headache" label is not hyperbole — a significant proportion of cluster headache patients report suicidal thoughts during attacks due to the extreme pain. This is a known, documented phenomenon. Patients need to hear that this reaction is understood and that effective treatments exist. Emergency support resources should be part of the management conversation.
- Depression and anxiety: Very high comorbidity rates, both as a consequence of recurrent severe pain and potentially sharing neurobiological mechanisms. Active screening and treatment are important.
- Medication overuse headache: Excessive reliance on acute treatments (particularly triptans) can paradoxically increase attack frequency and complicate the clinical picture.
- Cardiac effects from verapamil: High-dose verapamil (often required for prevention) carries real cardiac risks — bradycardia, heart block — requiring regular ECG monitoring.
- Occupational and social disability: Cluster periods lasting weeks to months with multiple daily attacks cause significant loss of productivity. The unpredictable, incapacitating nature of attacks makes sustained employment difficult for some patients.
- Social isolation from alcohol avoidance: During cluster periods, complete alcohol avoidance is necessary. For patients whose social lives involve alcohol, this creates meaningful social friction and isolation.
Key Research Papers
- Headache Classification Committee of the International Headache Society. ICHD-3. Cephalalgia. 2018. PMID: 29368949
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
PubMed Topic Searches
- cluster headache treatment
- cluster headache verapamil prevention
- cluster headache oxygen therapy
- trigeminal autonomic cephalalgias
- cluster headache pathophysiology hypothalamus
- galcanezumab cluster headache
Connections
- Pain & Allergy
- Migraine
- Chronic Pain
- Neuropathic Pain
- Trigeminal Neuralgia
- Depression
- Anxiety
- Insomnia
- Magnesium
- Vitamin D
- Headache — the symptom overview covering every head-pain type and its red flags.