Eosinophilic Esophagitis
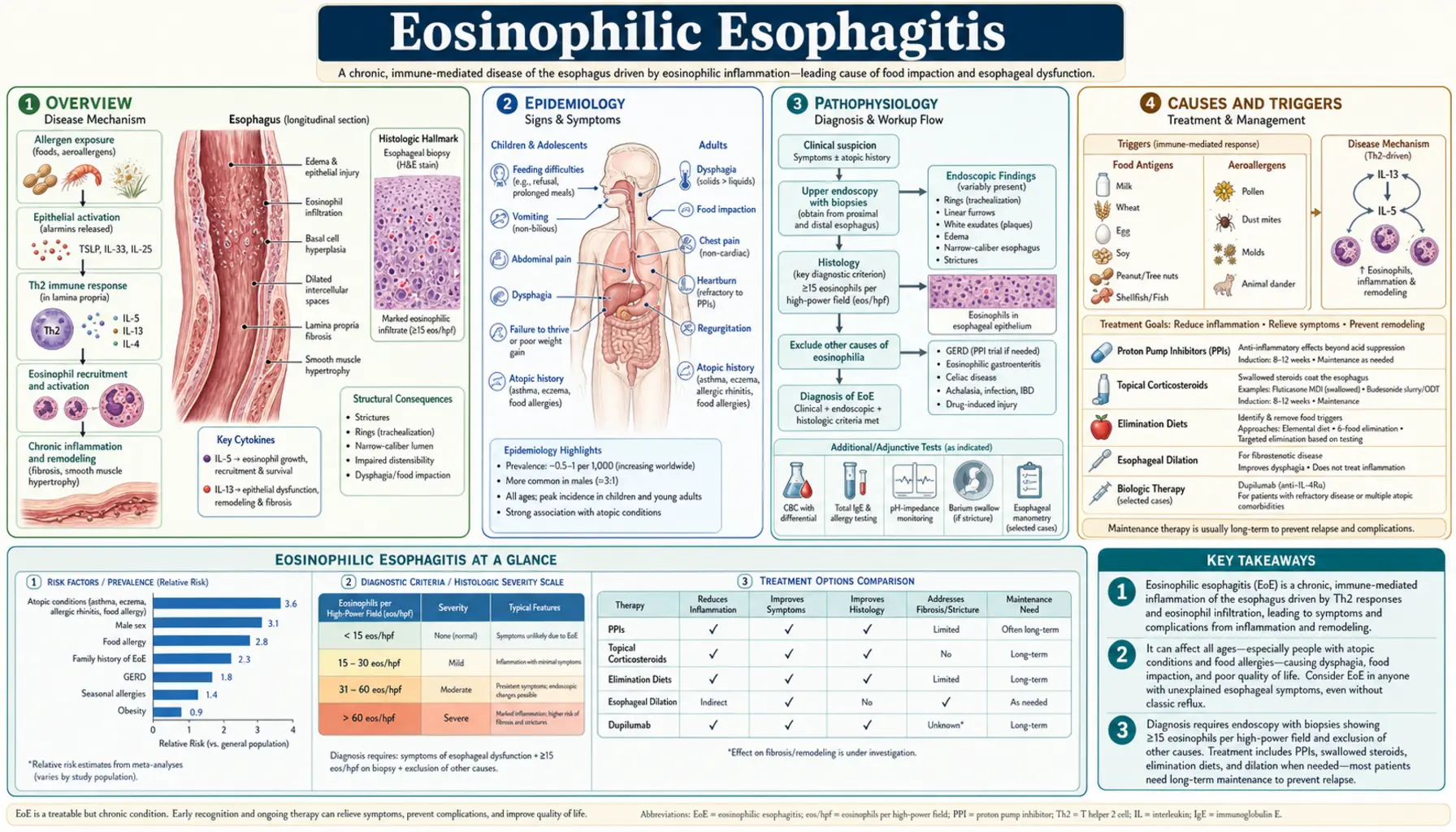
Table of Contents
- Overview
- Epidemiology
- Pathophysiology
- Causes and Triggers
- Clinical Presentation
- Diagnosis
- Treatment — Medications
- Treatment — Dietary Approaches
- Esophageal Dilation
- Living with EoE
- Recent Research and Advances
- References & Research
- Connections
- Featured Videos
1. Overview
Eosinophilic esophagitis — abbreviated EoE — is a chronic, immune-mediated, antigen-driven disease of the esophagus (the muscular tube that carries food from your mouth to your stomach). The defining feature is an abnormal buildup of a type of white blood cell called an eosinophil in the lining of the esophagus. The diagnostic standard established by international consensus: 15 or more eosinophils per high-power field (eos/hpf) on a biopsy sample, along with symptoms of esophageal dysfunction, and exclusion of other causes of esophageal eosinophilia.
EoE is a food-antigen-driven disease. The immune system misidentifies proteins from certain common foods as threats and mounts a sustained inflammatory attack on the esophageal lining. Over time, that chronic inflammation causes the wall of the esophagus to thicken, stiffen, and sometimes narrow — producing the hallmark symptom in adults: food getting stuck while swallowing (dysphagia). In children the picture is often more vague: feeding problems, persistent vomiting, and failure to thrive can all be presenting signs.
EoE is an emerging disease in the truest sense. It was first described as a distinct clinical entity in the early 1990s. Before that, the condition either went unrecognized or was lumped in with gastroesophageal reflux disease. Incidence has been rising steadily in Western countries — now estimated at roughly 10 new cases per 100,000 people per year — and EoE is now the most common cause of both esophageal eosinophilia and food bolus impaction in young adults. Whether this represents a true increase in disease occurrence or improved recognition (or both) remains an active research question.
The good news is that EoE is genuinely manageable. Proton pump inhibitors, swallowed topical steroids, carefully structured elimination diets, esophageal dilation, and — since 2022 — a targeted biologic medication have all been shown to reduce esophageal inflammation, relieve symptoms, and prevent the structural damage that accumulates when the disease is left uncontrolled. This page explains all of those options in plain language.
2. Epidemiology
EoE affects approximately 0.5 to 1.0 per 1,000 people in Western populations, with prevalence continuing to rise. It is distinctly more common in males — the male-to-female ratio is approximately 3:1 — and peaks diagnostically in two windows: childhood and early adulthood (20s and 30s), though it can present at any age including middle age and beyond. EoE is not equally distributed geographically: it is more common in cold, dry climates, in urban environments, and in industrialized countries generally, consistent with an “old-friends hypothesis” — the idea that reduced early-life microbial exposure skews immune development toward atopic reactivity.
The atopic connection is one of EoE’s most consistent epidemiological features. At least 70% of EoE patients have one or more co-existing atopic conditions: asthma, allergic rhinitis (hay fever), atopic dermatitis (eczema), or IgE-mediated food allergy. This is not coincidence. EoE shares the same Th2-skewed immune architecture as all of these conditions, and treating one atopic condition (as dupilumab now does) can simultaneously address others. The atopic overlap also means that diagnosing one condition in a patient should prompt consideration of EoE, and vice versa.
There is meaningful family clustering. First-degree relatives of someone with EoE have approximately a tenfold elevated risk of developing the condition themselves. This familial aggregation likely reflects both shared genetic susceptibility (variants in genes like TSLP, desmoglein-1, and calpain-14 that affect epithelial barrier function and eosinophil biology) and shared environmental exposures such as diet and allergen exposure in the home.
Seasonal and geographic variation adds further texture. In some patients, symptoms and esophageal eosinophilia worsen during pollen seasons, pointing to a role for aeroallergens (not just food antigens) in modulating disease activity. This has practical implications: a patient who seems to be “failing” dietary therapy during spring or fall may actually be experiencing pollen-driven inflammation that the dietary intervention was never designed to address.
3. Pathophysiology
In a healthy esophagus, eosinophils are essentially absent. The esophageal epithelium (inner lining cells) forms a tight physical barrier against food proteins, and the local immune environment is tolerant. In EoE, this system breaks down at two levels simultaneously.
First, the epithelial barrier becomes leaky. Genetic variants in desmoglein-1 (a protein that holds esophageal cells tightly together) and calpain-14 (a protease that influences barrier integrity) appear to lower the threshold at which food antigens can penetrate into the tissue. Once inside, those antigens are presented to immune cells that have been primed, likely by early-life exposures or aeroallergen sensitization, to respond with a Th2 immune reaction.
Second, the immune system launches a Th2-driven inflammatory response. Dendritic cells and epithelial cells release thymic stromal lymphopoietin (TSLP) and IL-33, which activate Th2 T-cells. These cells then produce three critical cytokines:
- IL-5: a powerful survival and recruitment signal for eosinophils; drives their accumulation in the esophageal tissue
- IL-13: promotes epithelial barrier dysfunction, fibrosis, and directly induces eotaxin-3 production by epithelial cells
- IL-4: amplifies the Th2 response and shares receptor signaling with IL-13 (both use the IL-4 receptor alpha chain, which is why dupilumab blocking that chain addresses both)
Eotaxin-3, released by esophageal epithelial cells in response to IL-13, is the principal chemokine that draws eosinophils into the esophageal mucosa from the circulation.
Eosinophils that accumulate in the esophageal wall are not passive bystanders. They degranulate, releasing toxic granule proteins (major basic protein, eosinophil cationic protein, eosinophil peroxidase) that damage tissue directly and perpetuate the inflammatory cycle. Over months and years, this chronic inflammation drives remodeling of the esophageal wall: thickening of the epithelium, deposition of fibrous tissue (fibrosis) in the lamina propria, and hypertrophy of the smooth muscle. It is this fibrotic remodeling — not just the acute inflammation itself — that leads to the concentric rings, longitudinal furrows, and strictures that trap food.
This pathophysiology explains the pharmacology of EoE’s most effective treatments. Swallowed topical steroids broadly suppress the Th2 inflammatory cascade. Dupilumab, the FDA-approved biologic, blocks both IL-4 and IL-13 signaling simultaneously by targeting the shared IL-4 receptor alpha chain — cutting two of the three key cytokines driving chronic inflammation and barrier dysfunction at their source.
4. Causes and Triggers
EoE is caused by an abnormal immune response to food proteins. Critically, this is not IgE-mediated allergy — it is a Th2 T-cell and eosinophil-driven response. This distinction matters because it means standard allergy skin-prick tests and blood IgE tests identify the food triggers of EoE less reliably than they do in classic food allergy. The only validated way to identify which foods are driving a patient’s EoE is a structured elimination diet followed by step-wise food reintroduction with endoscopic confirmation.
The “big six” food triggers account for the overwhelming majority of EoE cases:
- Cow’s milk — the single most common trigger, implicated in approximately 50% of cases. Eliminating milk alone produces histologic remission in a substantial proportion of patients.
- Wheat / gluten — the second most common trigger; about 30% of patients are wheat-responsive
- Eggs
- Soy
- Tree nuts and peanuts
- Seafood and shellfish
Aeroallergens also play a role in some patients. Seasonal variation in EoE activity — with worsening in spring and fall pollen seasons in some patients — suggests that airborne allergens (tree pollen, grass pollen) can either trigger or amplify esophageal eosinophilia. This has been demonstrated experimentally in mouse models and supported by epidemiological observations in humans.
Genetic susceptibility shapes who develops EoE. Three loci have been replicated across genome-wide association studies:
- TSLP (5q22): thymic stromal lymphopoietin is a central driver of Th2 sensitization; variants here are associated with EoE susceptibility and are shared with asthma and atopic dermatitis
- DSG1 (desmoglein-1): reduced expression of this epithelial junction protein is found in EoE biopsies and drives barrier dysfunction
- CAPN14 (calpain-14): a protease expressed almost exclusively in the esophagus; its variants are among the most EoE-specific genetic findings, suggesting a unique esophageal vulnerability distinct from other atopic tissues
5. Clinical Presentation
EoE presents very differently depending on patient age, and recognizing these age-specific patterns matters because the disease is frequently misdiagnosed — as GERD, functional dysphagia, or behavioral feeding problems in children — sometimes for years before the correct diagnosis is made.
Adults and older adolescents
The dominant symptom in adults is dysphagia — difficulty swallowing solid foods. Patients describe the sensation of food “sticking” or “not going down” after swallowing, typically with solid foods (meat, bread, rice) and rarely with liquids. A critical feature: many adults develop adaptive eating behaviors over years before ever receiving a diagnosis — eating very slowly, chewing food far more thoroughly than others, washing every bite down with large amounts of liquid, cutting food into tiny pieces, or quietly avoiding certain textures altogether. These adaptations mask how severely swallowing is impaired and dramatically delay diagnosis, sometimes by a decade or more.
The most dramatic acute presentation is a food bolus impaction: a piece of food (most commonly meat or bread) becomes completely lodged in a narrowed segment of the esophagus and cannot pass in either direction. The patient cannot swallow at all, may drool because saliva cannot pass, and experiences severe chest discomfort or pressure. This is a medical emergency requiring urgent endoscopic removal. Approximately 50% of EoE patients experience at least one food impaction episode, and a first impaction presenting to the emergency department is how a large proportion of adults receive their initial EoE diagnosis.
Other adult symptoms include heartburn and regurgitation (which is why EoE is so often initially misdiagnosed as GERD), non-cardiac chest pain, and — importantly — anxiety around eating. Many adults restrict their social lives because of fear of impaction in restaurants or at gatherings.
Infants, toddlers, and young children
Young children cannot articulate dysphagia, so their disease shows up as feeding difficulties: refusing solid foods, gagging or choking during meals, prolonged mealtimes, persistent vomiting beyond typical infant reflux, food aversion, irritability specifically during and after feeding, and in some cases failure to thrive due to inadequate caloric intake. Heartburn and abdominal pain become reportable complaints once children are old enough to describe them.
Because all of these symptoms overlap heavily with common childhood conditions (GERD, cow’s milk protein allergy, functional abdominal pain, behavioral feeding aversion), diagnosis in this age group is particularly challenging. Any child with persistent feeding difficulties, frequent vomiting, or failure to gain weight appropriately despite standard management deserves gastroenterological evaluation that includes consideration of EoE.
6. Diagnosis
The diagnosis of EoE rests on three elements used together: compatible symptoms of esophageal dysfunction, characteristic endoscopic findings, and confirmatory biopsy histology. No single element alone is sufficient.
Upper endoscopy (EGD)
Upper endoscopy (esophagogastroduodenoscopy) allows direct visualization of the esophageal lining. Classic endoscopic findings in EoE, scored using the EoE Endoscopic Reference Score (EREFS), include:
- Rings (trachealization / “feline esophagus”) — concentric rings that give the esophagus a corrugated appearance; reflect subepithelial fibrosis and remodeling
- Longitudinal furrows — vertical grooves running lengthwise; among the most sensitive endoscopic signs
- White exudates / plaques — small whitish specks on the mucosa representing eosinophilic microabscesses
- Edema / decreased vascularity — loss of the normal transparent submucosal vascular pattern; pale, hazy appearance
- Strictures or narrow-caliber esophagus — fixed narrowing that can cause food impaction
- Mucosal fragility (“crepe-paper mucosa”) — the lining tears easily on contact with the scope
Importantly, the esophagus can appear completely normal in up to 10% of biopsy-confirmed EoE cases. Biopsies must be taken even when the esophagus looks grossly normal if the clinical suspicion is present.
Biopsy and histology
A minimum of 6 biopsies from at least two locations (proximal and distal esophagus) are required. The diagnostic threshold is 15 or more eosinophils per high-power field in at least one biopsy specimen. Biopsies from the stomach and duodenum are also taken to rule out eosinophilic gastroenteritis and other causes of esophageal eosinophilia. Peripheral blood eosinophilia is present in only about 50% of patients; total IgE is often elevated but neither finding is diagnostic.
PPI trial — no longer a diagnostic requirement
Historically, guidelines required patients to complete an 8-week proton pump inhibitor trial before confirming EoE, because “PPI-responsive esophageal eosinophilia” was considered a separate entity. Current guidelines (AGA 2020, AGREE 2017) have retired this distinction. PPI-responsive disease is now classified as EoE. PPIs are a treatment option for EoE, not a diagnostic discriminator. This change streamlines diagnosis and has real-world implications: patients no longer need to delay potentially effective therapy while undergoing a diagnostic PPI trial.
Allergy testing
Skin prick testing and atopy patch testing have limited and unreliable predictive value for identifying the specific food triggers of EoE. They should not be used alone to guide dietary decisions without endoscopic confirmation of response. The only validated method of identifying food triggers remains structured elimination with endoscopic re-evaluation during reintroduction.
7. Treatment — Medications
EoE is a chronic disease that is manageable but not curable by current therapies. The goals of treatment are to reduce esophageal inflammation (inducing histologic remission), relieve symptoms, and prevent the progressive structural damage that accumulates with uncontrolled disease. Medications and dietary approaches are the two primary treatment categories, and they can be used alone or in combination.
Proton pump inhibitors (PPIs)
PPIs are a legitimate first-line pharmacologic treatment. Standard adult doses are 40–80 mg per day (e.g., omeprazole 20–40 mg twice daily or equivalent). Approximately 35–50% of EoE patients achieve histologic remission on PPI therapy alone. PPIs work in EoE via two mechanisms: they reduce acid-driven epithelial permeability (making it harder for food antigens to cross the esophageal lining) and they have direct anti-inflammatory effects through pathways independent of acid suppression. For patients who respond, PPI therapy is typically continued long-term because inflammation reliably recurs when it is stopped.
Swallowed topical corticosteroids
Steroids delivered topically to the esophageal mucosa achieve histologic remission in roughly 70–80% of treated patients and are the most studied pharmacologic treatment for EoE. Two formulations are in clinical use:
- Fluticasone propionate MDI, swallowed: the patient actuates a standard asthma inhaler into the mouth and swallows immediately (does not inhale); typical adult dose 880–1760 mcg/day divided. The inhaler is not rinsed after actuating; swallowing the mist delivers it to the esophageal mucosa.
- Budesonide orodispersible tablet (Jorveza / budesonide oral suspension): specifically formulated for EoE; dissolves in the mouth and coats the esophagus as it is swallowed; FDA approved 2023 in the US. Superior mucosal contact compared to the swallowed MDI approach. Standard adult dose 1 mg twice daily for 12 weeks.
Topical steroids are not absorbed systemically in significant amounts when used correctly, making them much safer than systemic steroids for long-term maintenance. The main adverse effect is oropharyngeal or esophageal candidiasis (thrush) in about 10% of patients; rinsing the mouth with water after each dose substantially reduces this risk. Use for 8–12 weeks to induce remission, then reassess with endoscopy.
Dupilumab (Dupixent) — FDA-approved biologic
Dupilumab, which blocks the receptor shared by IL-4 and IL-13 (the IL-4 receptor alpha chain), was approved by the FDA in May 2022 for EoE in patients aged 12 years and older — the first biologic ever approved specifically for this condition. In the pivotal Phase 3 PART B trial, approximately 47% of patients on dupilumab 300 mg every 2 weeks achieved histologic remission (<6 eos/hpf) versus 6% on placebo, with significant simultaneous improvements in symptoms of dysphagia and chest pain.
Dupilumab is given as a subcutaneous injection every two weeks. It is particularly beneficial for patients who also have atopic dermatitis, asthma, or chronic rhinosinusitis, because it treats all of these Th2-driven conditions simultaneously. Most common adverse effects are injection-site reactions and conjunctivitis. Dupilumab is the preferred option for patients who have not responded adequately to PPIs, topical steroids, and dietary modification, and it represents a meaningful advance for patients with severe or refractory disease.
Emerging biologics in clinical trials for EoE include cendakimab (anti-IL-13) and lirentelimab (anti-Siglec-8, targeting eosinophil and mast cell activity). These may offer additional options for patients who do not respond to dupilumab.
8. Treatment — Dietary Approaches
Because EoE is driven by food antigens, removing the triggering foods can eliminate the inflammatory stimulus entirely without any medication. Dietary therapy has no drug side effects and can produce durable histologic remission when the correct triggers are identified. The challenge is that it requires multiple endoscopies during the reintroduction phase, strict adherence, and ideally the support of a registered dietitian familiar with elimination diets.
Six-food elimination diet (SFED)
The SFED removes all six major trigger foods simultaneously: milk, wheat, eggs, soy, tree nuts/peanuts, and seafood/shellfish. After 6–8 weeks, endoscopy with biopsy assesses whether inflammation has resolved. Foods are then reintroduced one at a time, with endoscopy after each reintroduction to confirm or exclude that food as a trigger. Effective in approximately 50–72% of patients, but demanding to follow and requires multiple endoscopy sessions during reintroduction. The payoff: identifying the exact trigger(s) allows most foods to be safely reintroduced once those specific triggers are removed.
Two-food elimination diet (milk + wheat)
Removing only milk and wheat — the two most common EoE triggers — achieves remission in approximately 40–45% of patients with far fewer dietary restrictions and fewer endoscopies. This simpler approach is increasingly favored as a first step in dietary therapy, with the option to expand to a broader elimination if two-food elimination does not achieve remission. For a large proportion of patients, milk alone or milk plus wheat will be the only dietary change needed for the rest of their lives.
Four-food elimination diet (4FED)
Removes milk, wheat, eggs, and soy (the four highest-yield triggers). Achieves histologic remission in approximately 54% of patients. A useful intermediate step when two-food elimination has failed but the full SFED seems too burdensome.
Elemental (amino acid-based) formula
The most effective dietary approach, achieving histologic remission in over 90% of patients, because it replaces all intact food proteins with individual amino acids that cannot trigger an immune response. Primarily practical in infants and young children; most adults find a liquid formula diet socially and practically unsustainable as long-term therapy. It can be used as a short-term diagnostic tool to confirm food-antigen-driven disease before beginning systematic food reintroduction.
Working with a dietitian
Any patient pursuing elimination dietary therapy should work with a registered dietitian experienced in food allergy elimination diets. Eliminating major food groups (especially milk and wheat simultaneously) requires careful nutritional planning to ensure adequate calcium, protein, fiber, and caloric intake. In growing children, poorly managed elimination diets can cause nutritional deficiencies that compound the effects of the disease itself.
9. Esophageal Dilation
For patients who have developed fixed strictures, rings, or a narrow-caliber esophagus from years of untreated or undertreated EoE, mechanical widening of the esophagus provides rapid relief of dysphagia. During an endoscopy, the gastroenterologist uses either a bougie (a tapered dilating instrument) or a through-the-scope balloon dilator to gradually stretch the narrowed segment of the esophagus to a target diameter. The procedure takes only a few minutes within the endoscopy suite.
Dilation treats the mechanical consequence of EoE — the narrowing that traps food — but it does not address the underlying inflammation. Without concurrent anti-inflammatory therapy (medications or dietary elimination), the esophagus re-strictures as the inflammatory damage continues. Dilation must therefore always be combined with ongoing EoE treatment, not used as a stand-alone intervention.
Contrary to earlier concerns that dilation might be dangerous in the fragile EoE esophagus, modern data are reassuring: the risk of esophageal perforation with careful technique is less than 0.5%. Patients experience some temporary chest discomfort or soreness for a day or two after the procedure, which resolves on its own. Dysphagia relief is typically immediate and can be dramatic — patients who could barely swallow soft foods before dilation are often eating normally within days. For patients with longstanding undiagnosed EoE who present with severe impaction or near-complete stricture, dilation is the fastest path back to comfortable eating while the anti-inflammatory treatment takes effect over weeks.
10. Living with EoE
EoE is a chronic condition that, with appropriate management, most people can live with well. But it is also a condition that touches every meal, every restaurant, every social event — and the practical and psychological dimensions of managing it deserve the same attention as the medical treatment.
Eating strategies to reduce impaction risk
Many patients with active or partially treated EoE adopt habits that reduce impaction risk. These include: chewing every bite thoroughly before swallowing; taking smaller bites than usual; never eating dry or very dense foods without liquid available; eating slowly and pausing between bites to confirm each bite has passed; avoiding rushing meals. None of these strategies treat the disease, but they reduce the likelihood of an impaction episode during the period when treatment is taking effect.
Preparing for and responding to food impaction
Every EoE patient and their household members should understand what a food impaction feels like and what to do. Signs include: complete inability to swallow after eating, the sensation of food stuck in the chest that does not clear within a few minutes, inability to swallow saliva, drooling, significant chest pain or pressure after eating. A suspected food impaction is a medical emergency. Do not wait to see if it resolves on its own overnight; seek urgent care immediately. Emergency endoscopic removal is the treatment; attempting to force food down with carbonated drinks or by inducing vomiting is not recommended and carries risk.
Managing dietary restrictions in daily life
Patients on elimination diets face significant daily challenges. Milk and wheat are present in an enormous range of processed foods, restaurant dishes, and packaged products. Reading ingredient labels carefully, communicating dietary needs when eating out, identifying safe restaurant choices, and meal-prepping at home all become routine skills. Many patients find it helpful to connect with online EoE patient communities where others share practical tips, safe product lists, and restaurant strategies that are not covered in a clinical consultation.
Children with EoE at school
Children with EoE on elimination diets need a clear plan for school lunches, birthday parties, and school events involving food. A 504 accommodation plan (in the US school system) can formalize dietary accommodations so that the school environment supports the child’s medical needs. School staff should be aware of signs of food impaction and know to treat it as a medical emergency.
The psychological burden
Food anxiety, social isolation, and reduced quality of life are well-documented in EoE. Many patients report eating differently in social situations (avoiding certain foods, eating less, eating before events), anxiety at restaurants, and embarrassment about adaptive eating behaviors. These psychological effects are real and can be debilitating. If mealtime anxiety is significantly affecting quality of life, referral to a psychologist familiar with chronic illness or medically-complex eating disorders can be very helpful alongside the medical management.
11. Recent Research and Advances
The last five years have transformed EoE from a condition with few pharmacologic options into one with an approved biologic and multiple additional agents in late-stage clinical trials.
The approval of dupilumab (Dupixent) in May 2022 was the field’s most significant milestone. Post-approval real-world data have confirmed the pivotal trial findings across more diverse patient populations and extended them to younger adolescents. A key open question is whether dupilumab modifies the natural history of fibrosis — whether blocking IL-4/IL-13 not only reduces acute eosinophilic inflammation but actually reverses or halts the subepithelial fibrosis that drives long-term structural damage. Early data are encouraging, with some patients showing improved esophageal distensibility (flexibility) on functional lumen imaging probe studies.
Cendakimab (an oral IL-13 antagonist) completed Phase 3 trials in EoE with positive results announced in 2023. Its oral formulation, if approved, would offer a significant convenience advantage over dupilumab’s injections. Lirentelimab (anti-Siglec-8, targeting both eosinophils and mast cells) is in Phase 2/3 trials, potentially offering a different mechanism of action for patients who do not respond to IL-4/IL-13-axis targeting.
Research into non-endoscopic monitoring tools is a major priority. Requiring endoscopy and biopsy to assess treatment response is invasive, costly, and limits how often disease activity can be evaluated. Tools under active development include the esophageal string test (a swallowed capsule device that samples esophageal eosinophil granule proteins), blood biomarkers (eotaxin-3, eosinophil-derived neurotoxin), and transnasal unsedated endoscopy. Validated non-invasive monitoring would allow much more responsive treatment adjustment and would particularly benefit children who require repeated endoscopies.
The role of the gut microbiome in EoE is an emerging research area. Patients with EoE have a distinct esophageal microbiome compared with healthy controls, with relative depletion of commensal bacteria that may normally support epithelial barrier function. Whether dysbiosis causes or simply co-occurs with EoE remains unclear, and probiotic interventions in EoE have not yet been adequately studied to warrant clinical recommendation.
12. References & Research
Key Research Papers
- Dellon ES, Hirano I. Epidemiology and Natural History of Eosinophilic Esophagitis. Gastroenterology. 2018;154(2):319–332. PMID: 28774845. DOI: 10.1053/j.gastro.2017.06.067
- Liacouras CA, Furuta GT, Hirano I, et al. Eosinophilic esophagitis: Updated consensus recommendations for children and adults. J Allergy Clin Immunol. 2011;128(1):3–20. PMID: 21477849. DOI: 10.1016/j.jaci.2011.02.040
- Dellon ES, Gonsalves N, Hirano I, et al. ACG clinical guideline: Evidenced based approach to the diagnosis and management of esophageal eosinophilia and eosinophilic esophagitis (EoE). Am J Gastroenterol. 2013;108(5):679–692. PMID: 23567357. DOI: 10.1038/ajg.2013.71
- Hirano I, Moy N, Heckman MG, et al. Endoscopic assessment of the oesophageal features of eosinophilic oesophagitis: validation of a novel classification and grading system. Gut. 2013;62(4):489–495. PMID: 22619368. DOI: 10.1136/gutjnl-2011-301817
- Kagalwalla AF, Sentongo TA, Ritz S, et al. Effect of six-food elimination diet on clinical and histologic outcomes in eosinophilic esophagitis. Clin Gastroenterol Hepatol. 2006;4(9):1097–1102. PMID: 16860614. DOI: 10.1016/j.cgh.2006.05.026
- Assa’ad AH, Gupta SK, Collins MH, et al. An antibody against IL-5 reduces numbers of esophageal intraepithelial eosinophils in children with eosinophilic esophagitis. Gastroenterology. 2011;141(5):1593–1604. PMID: 21854749. DOI: 10.1053/j.gastro.2011.07.044
- Lucendo AJ, Molina-Infante J, Arias Á, et al. Guidelines on eosinophilic esophagitis: evidence-based statements and recommendations for diagnosis and management in children and adults. United European Gastroenterol J. 2017;5(3):335–358. PMID: 28507746. DOI: 10.1177/2050640616689525
- Hirano I, Chan ES, Rank MA, et al. AGA Institute and the Joint Task Force on Allergy-Immunology Practice Parameters Clinical Guidelines for the Management of Eosinophilic Esophagitis. Gastroenterology. 2020;158(6):1776–1786. PMID: 32224803. DOI: 10.1053/j.gastro.2020.02.038
- Rothenberg ME, Spergel JM, Sherrill JD, et al. Common variants at 5q22 associate with pediatric eosinophilic esophagitis. Nat Genet. 2010;42(4):289–291. PMID: 20208534. DOI: 10.1038/ng.547
- Straumann A, Conus S, Degen L, et al. Budesonide is effective in adolescent and adult patients with active eosinophilic esophagitis. Gastroenterology. 2010;139(5):1526–1537. PMID: 20682320. DOI: 10.1053/j.gastro.2010.07.048
- Dellon ES, Collins MH, Rothenberg ME, et al. Dupilumab in Adults and Adolescents with Eosinophilic Esophagitis. N Engl J Med. 2022;387(25):2317–2330. PMID: 36515215. DOI: 10.1056/NEJMoa2205982
- Furuta GT, Liacouras CA, Collins MH, et al. Eosinophilic esophagitis in children and adults: a systematic review and consensus recommendations for diagnosis and treatment. Gastroenterology. 2007;133(4):1342–1363. PMID: 17919504. DOI: 10.1053/j.gastro.2007.08.017
PubMed Research Searches
The following PubMed searches link directly to current peer-reviewed literature on eosinophilic esophagitis. Each opens a live query in a new tab.
- Eosinophilic esophagitis overview
- EoE epidemiology and prevalence
- EoE Th2 pathophysiology (IL-5, IL-13)
- EoE food triggers and elimination diet
- EoE dysphagia and food impaction
- EoE endoscopy, biopsy, and EREFS scoring
- EoE and proton pump inhibitor therapy
- Swallowed topical steroids for EoE
- Dupilumab for EoE — clinical trials
- Esophageal dilation and strictures in EoE
- Pediatric EoE and feeding difficulties
- EoE quality of life and patient outcomes
Connections
- Pain & Allergy
- GERD / Acid Reflux
- Celiac Disease
- Crohn’s Disease
- Barrett’s Esophagus
- Gastritis
- SIBO
- Asthma
- Eczema (Atopic Dermatitis)
- All Conditions