Barrett's Esophagus
Interactive Visualization Stomach Acid & PPIs — run the proton pump Drive your stomach to pH 2, activate pepsin and free your B12 and iron — then take a PPI and watch the pH climb while the nutrients stop being released. Launch →
Table of Contents
- What Is Barrett's Esophagus?
- Specialized Intestinal Metaplasia
- Causes and Risk Factors
- Symptoms
- Diagnosis and Prague Classification
- Dysplasia Grading
- Surveillance Intervals
- Treatment: Endoscopic and Medical
- Dietary and Lifestyle Approaches
- Prognosis and Cancer Risk
- Key Research Papers
- Connections
- Featured Videos
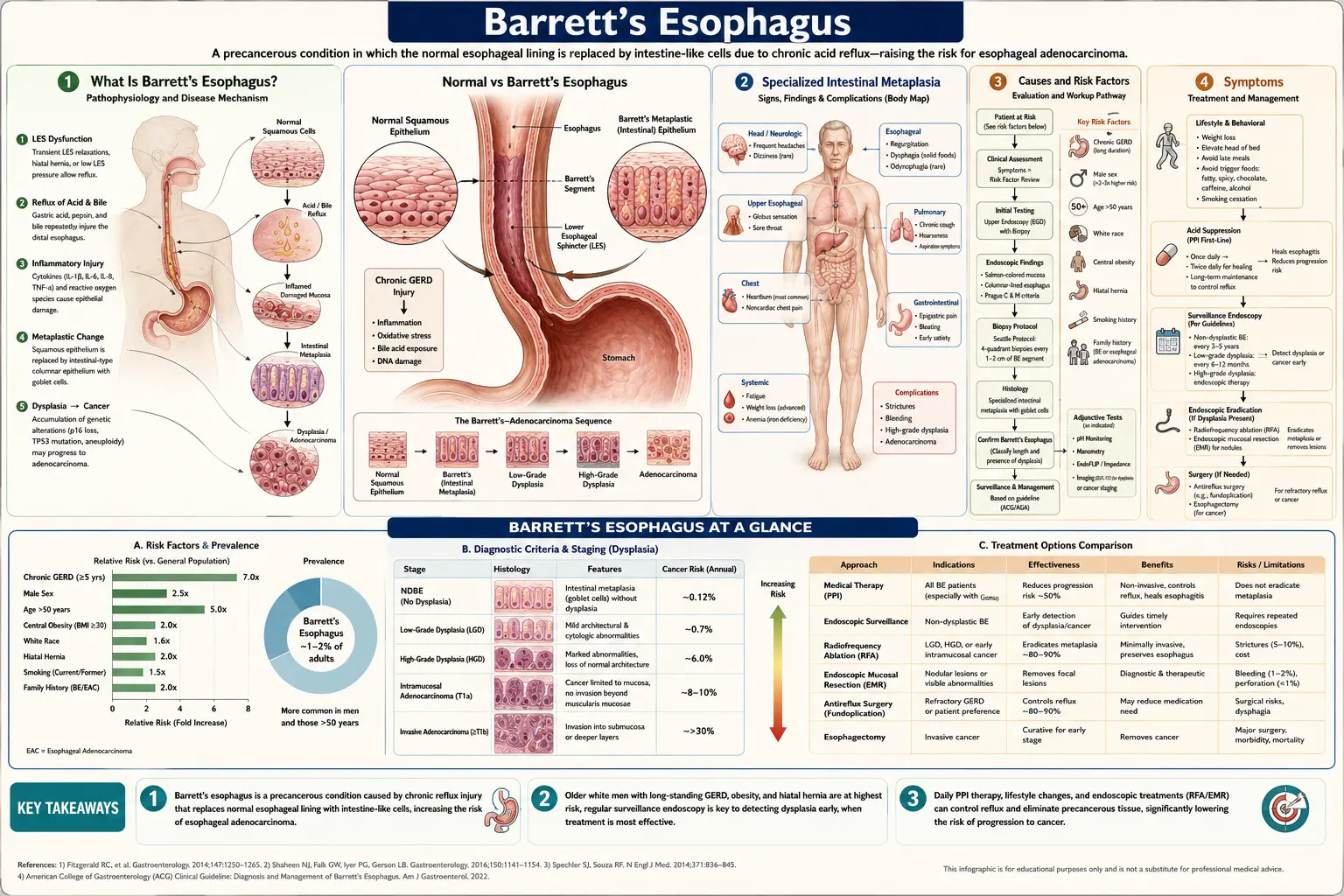
What Is Barrett's Esophagus?
Barrett's esophagus is a condition in which the normal squamous epithelium lining the lower esophagus is replaced by columnar epithelium containing specialized intestinal metaplasia (SIM) — cells that resemble the lining of the small intestine. This transformation, called metaplasia, is the body's response to chronic acid and bile reflux injury. While the metaplastic cells are more resistant to acid damage than normal squamous cells, they carry a significantly elevated risk of progressing to esophageal adenocarcinoma.
Named after British surgeon Norman Barrett, who described the condition in 1950 (though early accounts date to Philip Rowland Allison in 1946), Barrett's esophagus affects an estimated 5–15% of patients with chronic GERD. It is most common in middle-aged and older white men who have had heartburn symptoms for more than five years. In the United States, roughly 3.3 million adults have been diagnosed with the condition, though many more remain undiagnosed.
Barrett's esophagus matters primarily because it is the only known precursor lesion for esophageal adenocarcinoma — one of the fastest-rising cancers in the Western world. Understanding Barrett's, getting appropriately surveilled, and treating dysplasia before it becomes invasive cancer is one of gastroenterology's most important cancer prevention opportunities.
Specialized Intestinal Metaplasia
The hallmark of Barrett's esophagus is specialized intestinal metaplasia (SIM) — columnar epithelium containing goblet cells. Goblet cells are mucus-secreting cells normally found in the small and large intestine; their presence in the esophagus is abnormal and defines true Barrett's metaplasia (as opposed to simple cardiac-type columnar epithelium, which lacks goblet cells and carries unclear malignant potential).
The molecular changes underlying Barrett's metaplasia involve shifts in transcription factor expression (CDX2, a master regulator of intestinal differentiation, becomes aberrantly expressed in the metaplastic cells) and epigenetic alterations that progressively accumulate over time. These molecular changes prime the cells for the additional mutations — particularly in TP53 and cell-cycle regulators — that drive progression to dysplasia and invasive cancer.
The extent of Barrett's segment is measured by the Prague C&M classification, introduced in 2006 and now standard worldwide. "C" refers to the circumferential extent of visible metaplastic mucosa (in centimeters above the gastroesophageal junction), and "M" refers to the maximum extent (including any tongues or islands extending further). For example, C3M5 indicates 3 cm of circumferential Barrett's with a maximum extent of 5 cm. Longer segments generally carry higher cancer risk, though short-segment Barrett's (C0M<3) is more common and causes the majority of cancers in absolute numbers.
Causes and Risk Factors
- Chronic GERD — the dominant risk factor; weekly heartburn for 5+ years confers a 3–4-fold increased risk of Barrett's compared to individuals without GERD. Both acid and bile components of reflux are injurious.
- Male sex — men are 2–3 times more likely to develop Barrett's than women with equivalent GERD severity. The reason is not fully understood; hormonal differences (estrogen may be protective) and differences in bile composition have been proposed.
- Age over 50 — Barrett's is uncommon before age 40; peak diagnosis is in the 60s.
- Obesity, especially central adiposity — visceral fat increases intra-abdominal pressure, promotes hiatal hernia, and independently drives adipokine signaling that may promote metaplasia.
- White ethnicity — Barrett's and esophageal adenocarcinoma are markedly more common in non-Hispanic whites than in Black, Hispanic, or Asian populations.
- Cigarette smoking — doubles the risk; smoking impairs lower esophageal sphincter pressure and promotes mucosal injury.
- Hiatal hernia — allows the gastroesophageal junction to ride above the diaphragmatic crura, impairing the natural anti-reflux barrier.
- Family history — familial Barrett's esophagus or esophageal adenocarcinoma increases risk 2–3-fold, suggesting genetic susceptibility loci.
- Possible protective factors — aspirin and other NSAIDs, H. pylori infection (paradoxically, H. pylori reduces GERD by decreasing acid secretion), and high intake of fruits and vegetables have all been associated with reduced Barrett's risk in observational data.
Symptoms
Barrett's esophagus itself causes no unique symptoms. Most patients present with the same symptoms as GERD:
- Heartburn — burning sensation in the chest, typically after eating or when lying down
- Regurgitation — sour or bitter fluid rising into the throat
- Dysphagia — difficulty swallowing, particularly if a stricture has developed
- Chest pain — can mimic cardiac pain; always evaluate cardiac causes first
- Chronic cough, hoarseness, or laryngitis — from laryngopharyngeal reflux
Paradoxically, some patients with Barrett's have less heartburn than those with uncomplicated GERD, possibly because the columnar mucosa is less sensitive to acid than squamous epithelium. This means absence of heartburn does not rule out Barrett's, and may explain why many cases are diagnosed only when adenocarcinoma has already developed.
Diagnosis and Prague Classification
Diagnosis requires both endoscopic visualization and confirmatory biopsy.
- Upper endoscopy (EGD) — the endoscopist identifies salmon-colored or pinkish columnar-appearing mucosa extending proximally from the gastroesophageal junction (GEJ), which normally presents as a sharp squamocolumnar junction (Z-line or SCJ). Suspicion is raised when the Z-line is irregular or when tongue-like projections extend above the GEJ.
- Prague C&M classification — the endoscopist measures and documents the circumferential (C) and maximal (M) extent of Barrett's mucosa in centimeters, using the GEJ and the diaphragmatic hiatus as landmarks. This standardized description facilitates communication between endoscopists and tracking of segment changes over time.
- Biopsy using the Seattle protocol — four-quadrant biopsies taken every 1–2 cm along the length of the Barrett's segment, plus targeted biopsies of any visible lesions, nodules, or mucosal irregularities. Random biopsies are critical because dysplasia is patchy and invisible to standard white-light endoscopy.
- Histopathology — the pathologist confirms the presence of goblet cells (SIM) and grades dysplasia: no dysplasia, indefinite for dysplasia, low-grade dysplasia (LGD), or high-grade dysplasia (HGD). Dysplasia grading should be confirmed by a second expert GI pathologist, as interobserver variability is high.
- Advanced imaging adjuncts — narrow-band imaging (NBI), chromoendoscopy with acetic acid spray, and confocal laser endomicroscopy can improve dysplasia detection beyond standard white-light endoscopy and are increasingly used in high-volume Barrett's centers.
Dysplasia Grading
The natural history of Barrett's esophagus follows a progression from metaplasia through increasing grades of dysplasia to invasive adenocarcinoma. Dysplasia grade is the single most important predictor of cancer risk and determines management:
- Non-dysplastic Barrett's (NDBE) — goblet cells present but no architectural or nuclear atypia. Annual cancer risk approximately 0.1–0.3%. The majority of Barrett's patients remain at this stage indefinitely.
- Indefinite for dysplasia — reactive atypia that cannot be confidently graded due to inflammation, ulceration, or poor tissue orientation. Optimize acid suppression and repeat endoscopy in 3–6 months.
- Low-grade dysplasia (LGD) — mild nuclear enlargement and crowding with preserved architecture. Annual cancer risk approximately 0.5–1.5% per year. Management has shifted toward endoscopic eradication for confirmed LGD due to high rates of under-staging and progression.
- High-grade dysplasia (HGD) — marked nuclear atypia with glandular architectural disarray. Annual cancer risk without treatment approximately 6–10% per year. Essentially all current guidelines recommend endoscopic eradication therapy for confirmed HGD.
Surveillance Intervals
Surveillance endoscopy detects dysplasia and early cancer at treatable stages. ACG, BSG, and AGA guidelines generally recommend:
- Non-dysplastic Barrett's — repeat endoscopy every 3–5 years (exact interval depends on segment length; shorter for long-segment Barrett's >3 cm)
- Indefinite for dysplasia — optimize PPI therapy, repeat in 3–6 months
- Low-grade dysplasia — confirmed by a second pathologist; either endoscopic eradication or enhanced surveillance every 6–12 months if eradication is declined
- High-grade dysplasia — endoscopic eradication therapy; post-treatment surveillance every 3 months for the first year, then annually if complete eradication is achieved
Surveillance should be performed in centers with experienced Barrett's endoscopists. The benefit of surveillance is greatest for patients with confirmed dysplasia; for non-dysplastic Barrett's, the absolute cancer reduction from surveillance remains debated, and shared decision-making accounting for patient health and preferences is appropriate.
Treatment: Endoscopic and Medical
Endoscopic Eradication Therapy (EET)
Endoscopic therapies have largely replaced surgery for dysplastic Barrett's and are the standard of care for HGD and increasingly for confirmed LGD:
- Radiofrequency ablation (RFA) — the most widely used and best-studied ablative modality. A balloon-based or focal catheter delivers controlled radiofrequency energy to destroy the Barrett's epithelium to a depth of ~0.5–1 mm. Multiple sessions (typically 2–3) are needed. Complete eradication of intestinal metaplasia (CE-IM) is achieved in ~77–90% of patients. The squamocolumnar junction regrows with native squamous epithelium, provided acid suppression is maintained with high-dose PPIs.
- Endoscopic mucosal resection (EMR) — visible lesions, nodules, or areas suspicious for submucosal invasion should be removed by EMR first, before ablation, to obtain full histological staging. A saline cushion is injected submucosally, the lesion is suctioned into a cap, and a snare is used to resect it.
- Endoscopic submucosal dissection (ESD) — allows en-bloc resection of larger lesions for more accurate staging; technically demanding but increasing in use at expert centers.
- Cryotherapy — liquid nitrogen or carbon dioxide spray freezes and destroys the Barrett's epithelium; an alternative for patients in whom RFA has failed or for circumferential ablation in very long segments.
- Photodynamic therapy (PDT) — now largely replaced by RFA due to higher stricture rates and photosensitivity side effects.
Medical Therapy: PPIs and Chemoprevention
- High-dose PPIs — twice-daily PPI therapy (e.g., omeprazole 40 mg twice daily) is standard before and after endoscopic eradication to maximize acid suppression and support squamous re-epithelialization. PPIs also appear to reduce cancer progression risk in observational studies, though no randomized trial has definitively confirmed a chemoprevention benefit.
- Aspirin and NSAIDs — multiple observational studies and the AspECT trial (2018) found that daily aspirin 300 mg combined with high-dose esomeprazole significantly delayed disease progression and reduced all-cause mortality in Barrett's. The absolute benefit was modest; current guidelines do not universally recommend aspirin for chemoprevention but may consider it in patients already taking it for cardiovascular indications.
- Surgical fundoplication — laparoscopic Nissen fundoplication corrects GERD mechanically; it may reduce acid reflux more completely than PPIs but has not been shown to cause regression of established Barrett's or reduce cancer risk in randomized controlled trials.
Dietary and Lifestyle Approaches
- Weight loss — even modest weight reduction (5–10% of body weight) reduces intra-abdominal pressure and reflux frequency; the most impactful lifestyle change for obese patients with Barrett's.
- Elevate the head of the bed 6–8 inches — reduces nocturnal acid exposure, which is particularly relevant because esophageal acid clearance is slowest during sleep. Using a foam wedge under the mattress is more effective than extra pillows.
- Avoid late meals — eat at least 2–3 hours before lying down.
- Reduce dietary triggers — alcohol, fatty foods, chocolate, peppermint, coffee, and citrus relax the lower esophageal sphincter or directly irritate the mucosa. Individual tolerance varies; a food-symptom diary helps identify personal triggers.
- Increase fruits, vegetables, and fiber — epidemiological data consistently associate Mediterranean-style diets with reduced Barrett's progression risk, likely through antioxidant and anti-inflammatory effects.
- Avoid tight clothing and prolonged bending — increases intra-abdominal pressure and promotes reflux episodes.
- Stop smoking — smoking cessation is strongly recommended; tobacco use is associated with faster Barrett's progression in several cohort studies.
Prognosis and Cancer Risk
The overall risk of a patient with non-dysplastic Barrett's esophagus developing esophageal adenocarcinoma is approximately 0.1–0.3% per year — considerably lower than historical estimates of 0.5% per year that were derived from referral-center populations. This means that for most Barrett's patients, the condition is managed by surveillance rather than aggressive intervention, and the majority will never develop cancer.
Risk stratification is important:
- Longer segment (C>3 cm) carries 5-fold higher cancer risk than short-segment Barrett's.
- Dysplasia grade is the strongest predictor: LGD raises annual risk to ~0.5–1.5%, HGD to ~6–10%.
- Biomarkers under study — TP53 mutation in biopsies, DNA ploidy analysis, and methylation signatures may help identify which non-dysplastic Barrett's patients are at higher risk, but none are yet in routine clinical use.
Esophageal adenocarcinoma detected within a Barrett's surveillance program has a substantially better prognosis than cancer discovered symptomatically — 5-year survival rates are 50–60% for surveillance-detected stage I cancers vs. 15–20% overall. This is the rationale for surveillance programs despite the relatively low absolute cancer incidence.
Key Research Papers
- Barrett NR. Chronic peptic ulcer of the oesophagus and oesophagitis. Br J Surg. 1950;38(150):175-182. PMID: 14791960
- Shaheen NJ, Falk GW, Iyer PG, Gerson LB; American College of Gastroenterology. ACG Clinical Guideline: Diagnosis and Management of Barrett's Esophagus. Am J Gastroenterol. 2016;111(1):30-50. PMID: 26526079
- Sharma P, Dent J, Armstrong D, et al. The development and validation of an endoscopic grading system for Barrett's esophagus: the Prague C & M criteria. Gastroenterology. 2006;131(5):1392-1399. PMID: 17101315
- Shaheen NJ, Sharma P, Overholt BF, et al. Radiofrequency ablation in Barrett's esophagus with dysplasia (AIM Dysplasia trial). N Engl J Med. 2009;360(22):2277-2288. PMID: 19474425
- Phoa KN, van Vilsteren FG, Weusten BL, et al. Radiofrequency ablation vs endoscopic surveillance for patients with Barrett esophagus and low-grade dysplasia (SURF trial). JAMA. 2014;311(12):1209-1217. PMID: 24668104
- Jankowski JAZ, de Caestecker J, Love SB, et al. Esomeprazole and aspirin in Barrett's oesophagus (the AspECT trial). Lancet. 2018;392(10145):400-408. PMID: 30057104
- Spechler SJ, Sharma P, Souza RF, et al. American Gastroenterological Association technical review on the management of Barrett's esophagus. Gastroenterology. 2011;140(3):e18-52. PMID: 21376939
- Souza RF, Krishnan K, Spechler SJ. Acid, bile, and CDX: the ABCs of making Barrett's metaplasia. Am J Physiol Gastrointest Liver Physiol. 2008;295(2):G211-218. PMID: 18556418
- Hvid-Jensen F, Pedersen L, Drewes AM, et al. Incidence of adenocarcinoma among patients with Barrett's esophagus. N Engl J Med. 2011;365(15):1375-1383. PMID: 21995385
- Fitzgerald RC, di Pietro M, Ragunath K, et al. British Society of Gastroenterology guidelines on the diagnosis and management of Barrett's oesophagus. Gut. 2014;63(1):7-42. PMID: 24165758
- Wani S, Falk GW, Post J, et al. Risk factors for progression of low-grade dysplasia in patients with Barrett's esophagus. Gastroenterology. 2011;141(4):1179-1186. PMID: 21723214
- Corley DA, Mehtani K, Quesenberry C, et al. Impact of endoscopic surveillance on mortality from Barrett's esophagus-associated esophageal adenocarcinomas. Gastroenterology. 2013;145(2):312-319. PMID: 23333651
Live PubMed Searches
Curated PubMed topic searches of peer-reviewed literature on Barrett's esophagus. Each link opens a live PubMed query so you always see the most current studies.
- PubMed: Barrett's RFA ablation
- PubMed: Barrett's dysplasia progression
- PubMed: Barrett's surveillance guidelines
- PubMed: Specialized intestinal metaplasia
- PubMed: Esophageal adenocarcinoma Barrett's risk
- PubMed: Prague C&M criteria
- PubMed: PPI chemoprevention Barrett's
- PubMed: EMR for Barrett's esophagus
- PubMed: GERD obesity Barrett's risk
- PubMed: Aspirin Barrett's chemoprevention
Connections
- Gastroenterology
- Stomach Acid, pH & the PPI Trade-off — interactive animation
- GERD
- Gastritis
- Peptic Ulcer Disease
- Pancreatitis
- Gallbladder Disease
- Appendicitis
- Fatty Liver Disease (NAFLD/MASLD)
- Celiac Disease
- Ulcerative Colitis
- SIBO
- Irritable Bowel Syndrome
- Vitamin C (antioxidant mucosal protection)
- Licorice Root (DGL)