Anaphylaxis
- What is Anaphylaxis?
- Most Common Triggers
- How It Feels: Recognizing an Attack
- The Biphasic Reaction
- Diagnostic Criteria
- First Response: Epinephrine
- Hospital Treatment
- Living with Anaphylaxis Risk
- Special Populations
- Complications and Prognosis
- Key Research Papers
- Connections
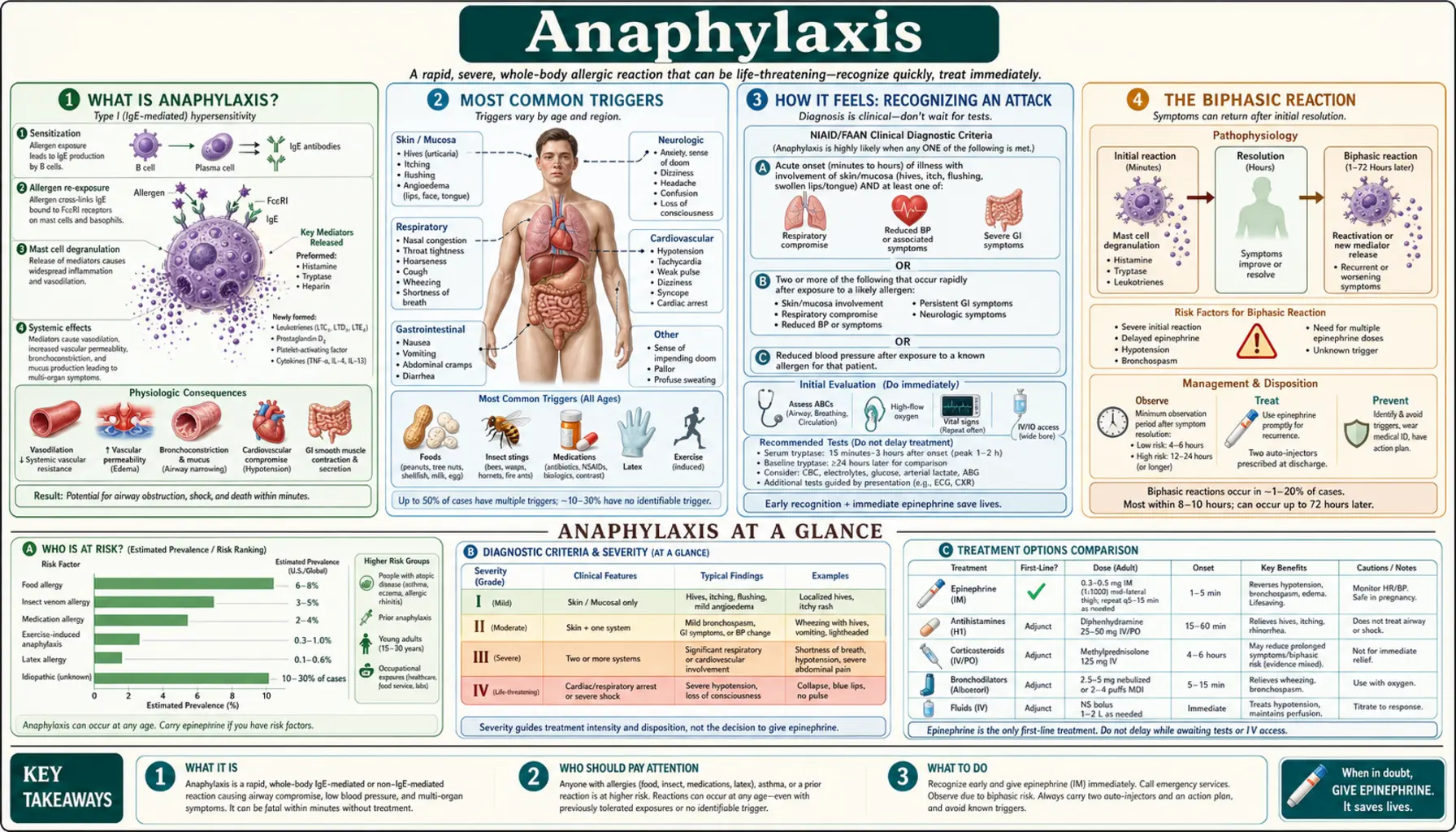
What is Anaphylaxis?
Anaphylaxis is a severe, life-threatening allergic reaction that occurs rapidly and involves multiple body systems simultaneously. It is the most extreme end of the allergic spectrum. The immune system — usually via IgE antibodies — responds to a trigger (allergen) by releasing massive amounts of chemical mediators from mast cells and basophils: histamine, tryptase, leukotrienes, prostaglandins, platelet-activating factor. This triggers vasodilation, increased vascular permeability (fluid leaks from blood vessels), bronchoconstriction, and mucus overproduction — all at once.
Without prompt treatment, anaphylaxis can cause distributive shock, respiratory arrest, and death within minutes. In the United States, anaphylaxis causes roughly 1,500–2,000 deaths per year. Incidence is rising, particularly food-triggered anaphylaxis in children.
Most Common Triggers
- Food (most common in children): Peanuts, tree nuts, milk, eggs, wheat, soy, fish, shellfish — the "Big Eight" account for more than 90% of food-allergic reactions. Peanuts and tree nuts are leading causes of fatal anaphylaxis.
- Medications (most common in adults): Penicillin and related beta-lactam antibiotics; NSAIDs; aspirin; ACE inhibitors; monoclonal antibodies; contrast dye; anesthetics; opioids.
- Insect stings: Hymenoptera venom (bees, wasps, hornets, yellow jackets, fire ants) — accounts for approximately 100 deaths per year in the US.
- Latex: Particularly in healthcare workers and children with spina bifida.
- Exercise-induced anaphylaxis: Rare but real; can occur with or without a food cofactor (eating wheat then exercising is a classic pattern).
- Idiopathic anaphylaxis: No identifiable trigger despite thorough evaluation; accounts for approximately 30–40% of anaphylaxis in adults.
- Alpha-gal syndrome: Delayed IgE-mediated reaction to mammalian meat 3–6 hours after ingestion.
- Mast cell disorders: MCAS or mastocytosis amplifies severity and lowers the reaction threshold.
How It Feels: Recognizing an Attack
Anaphylaxis typically develops within seconds to minutes of allergen exposure (or up to 30 minutes for food). Early warning signs — which patients learn to recognize — include: tingling or itching in the mouth, lips, tongue, or throat; a warm flushing sensation over the skin; hives appearing suddenly; and a feeling of dread or that "something is very wrong."
As the reaction progresses, symptoms escalate: throat tightening, hoarseness, stridor (a high-pitched breathing sound); difficulty swallowing or speaking; chest tightness, wheezing; stomach cramps, nausea, vomiting; lightheadedness or feeling faint; a rapid, weak pulse; and loss of consciousness. The most dangerous signs are throat and airway swelling and cardiovascular collapse (shock). Even patients who have had prior mild reactions can experience a severe or fatal reaction on the next exposure.
The Biphasic Reaction
In 4–23% of cases (estimates vary widely), patients experience a biphasic reaction — a second wave of anaphylaxis occurring 1–72 hours after the initial reaction resolves, even without additional allergen exposure. This is why emergency department observation is recommended for 4–8 hours after apparent recovery, and why epinephrine auto-injectors come in two-packs.
Protracted anaphylaxis (lasting more than 6 hours) is a distinct and more dangerous variant requiring intensive monitoring. Risk factors for a biphasic reaction include: a severe initial reaction; delayed administration of epinephrine; and needing multiple doses of epinephrine during the initial event. Corticosteroids are commonly given to reduce biphasic risk, though the evidence for this practice is weaker than historically believed.
Diagnostic Criteria
The World Allergy Organization (WAO) and NIAID/FAAN diagnostic criteria define anaphylaxis as highly likely when any one of these three criteria is met:
- Acute onset of illness (minutes to hours) with involvement of skin or mucosal tissue plus respiratory compromise or cardiovascular symptoms.
- Two or more of the following after allergen exposure: skin or mucosal symptoms; respiratory compromise; cardiovascular collapse; persistent GI symptoms.
- Reduced blood pressure after exposure to a known allergen for that patient.
Serum tryptase level (drawn 15–180 minutes after onset) can confirm mast cell activation but is not required for clinical diagnosis. A normal tryptase does not rule out anaphylaxis — food-triggered anaphylaxis in particular often shows normal or minimally elevated tryptase.
First Response: Epinephrine
Epinephrine (adrenaline) is the only first-line treatment for anaphylaxis — all other medications are second-line adjuncts. It works by reversing vasodilation (causing vasoconstriction), reducing airway swelling (bronchodilation and decreased mucus production), and supporting cardiac function. There is no absolute contraindication to epinephrine in anaphylaxis.
Dose: 0.3–0.5 mg (adult) or 0.01 mg/kg (child, max 0.5 mg) of 1:1000 solution injected intramuscularly into the outer thigh. Auto-injectors (EpiPen, Auvi-Q, Symjepi) — push firmly into the outer thigh and hold for 10 seconds. Can be given through clothing. Position the patient flat with legs elevated (unless breathing is worse lying flat). Call 911 immediately. If there is no improvement in 5–15 minutes, give a second dose.
Delay in epinephrine administration is the leading cause of preventable anaphylaxis death. Antihistamines and steroids do not work fast enough to treat anaphylaxis — they are secondary measures only and must never be used instead of epinephrine.
Hospital Treatment
Emergency department care focuses on supporting the airway, breathing, and circulation while reversing the allergic cascade:
- IV epinephrine infusion for refractory or cardiovascular-dominant cases
- IV fluid resuscitation (1–2 liters normal saline) for anaphylactic shock
- Supplemental oxygen; nebulized albuterol for bronchospasm
- H1 antihistamines (diphenhydramine) and H2 antihistamines (famotidine) — adjuncts to reduce skin symptoms, not primary treatment
- Systemic corticosteroids (methylprednisolone or prednisone) to reduce late-phase reactions — though evidence for preventing biphasic reactions is weaker than historically believed
- Intubation or emergency cricothyrotomy for complete airway obstruction
- Glucagon (1–5 mg IV) for patients on beta-blockers, who have a blunted epinephrine response and may require higher doses or alternative agents
Discharge planning must include: a prescription for two epinephrine auto-injectors; referral to an allergist for trigger identification and immunotherapy evaluation; and a written anaphylaxis action plan.
Living with Anaphylaxis Risk
Always carry two epinephrine auto-injectors — at school, work, travel, the gym, everywhere. Store them at room temperature; heat and freezing degrade the medication. Replace before expiration. Wear medical alert identification (bracelet, wallet card, or digital app).
Create a written anaphylaxis action plan with your allergist. For food-allergic patients: read ingredient labels carefully on every purchase — formulations change without obvious notice. "May contain" labeling is voluntary in the US; manufacturing cross-contact is a real risk that varies by brand and facility. When dining out, speak directly with kitchen staff and communicate the severity of your allergy.
Allergen immunotherapy for insect venom allergy (allergy shots) can dramatically reduce reaction severity and is curative in many patients — 97% maintain protection long-term. Peanut oral immunotherapy (Palforzia, FDA-approved 2020) raises the reaction threshold in peanut-allergic children from roughly 100 mg to 1,000 mg (about 10 peanuts), but does not eliminate risk and requires continued maintenance dosing.
Special Populations
Children: Food is the dominant trigger; children are at heightened risk during school meals, birthday parties, and social events. Schools must keep epinephrine available and train staff — 47 US states now mandate school epinephrine policies. Teens are a particularly high-risk group due to risk-taking behavior and delayed epinephrine use.
Pregnant women: Anaphylaxis during pregnancy is rare but dangerous. Epinephrine remains the recommended treatment — the fetal risk from untreated maternal anaphylaxis (hypoxia, shock) far exceeds any medication risk. Maternal cardiovascular collapse reduces uteroplacental blood flow acutely.
Older adults: More likely to have underlying cardiac disease and to be taking beta-blockers (which blunt the epinephrine response and require glucagon rescue); higher latex allergy risk from repeated medical procedures; greater risk of fatal outcomes from cardiovascular compromise.
Mastocytosis and MCAS: Patients with systemic mastocytosis or mast cell activation syndrome have amplified anaphylaxis, lower reaction thresholds, and may require pre-medication protocols before medical procedures or surgeries. They often benefit from standing daily antihistamines and in some cases daily omalizumab.
Complications and Prognosis
With prompt epinephrine, the vast majority of anaphylaxis cases resolve fully within hours. Fatal anaphylaxis risk factors include: underlying asthma (the single most important risk factor); delayed epinephrine administration; peanut or tree nut allergy; lack of an anaphylaxis action plan; exercise as a cofactor; advanced age with cardiac comorbidity; and use of beta-blockers or ACE inhibitors.
Psychological sequelae are common and underrecognized: anxiety, post-traumatic stress, hypervigilance about food, and fear-driven dietary restriction can significantly impair quality of life. Patients — particularly children — benefit from psychological support as part of comprehensive allergy care. Some patients develop agoraphobia or social withdrawal out of fear of exposure.
With allergen avoidance, a solid emergency action plan, and appropriate immunotherapy where indicated, most people at risk for anaphylaxis lead full, active lives. The goal is not a life lived in fear, but a life lived prepared.
Key Research Papers
- Search PubMed
- Search PubMed
- Lieberman P, et al. The diagnosis and management of anaphylaxis practice parameter: 2010 update. J Allergy Clin Immunol. 2010. PMID: 20692689
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
PubMed Topic Searches
- Anaphylaxis epinephrine treatment
- Anaphylaxis biphasic reaction
- Food allergy anaphylaxis children
- Peanut oral immunotherapy
- Insect venom anaphylaxis immunotherapy
- Anaphylaxis prevention management
Connections
- Pain & Allergy
- Anaphylaxis & the EpiPen: An Allergy Emergency — interactive animation
- Histamine, Mast Cells & Allergy — interactive animation
- Allergies
- Mast Cell Activation Syndrome
- Alpha-Gal Syndrome
- Food Intolerance
- Eosinophilic Esophagitis
- Irritable Bowel Syndrome
- Total IgE Testing
- Tryptase Test
- Alpha-Gal Anaphylaxis Emergency Plan — step-by-step EpiPen, 911, and ER protocol for delayed alpha-gal reactions.