Normal Pressure Hydrocephalus
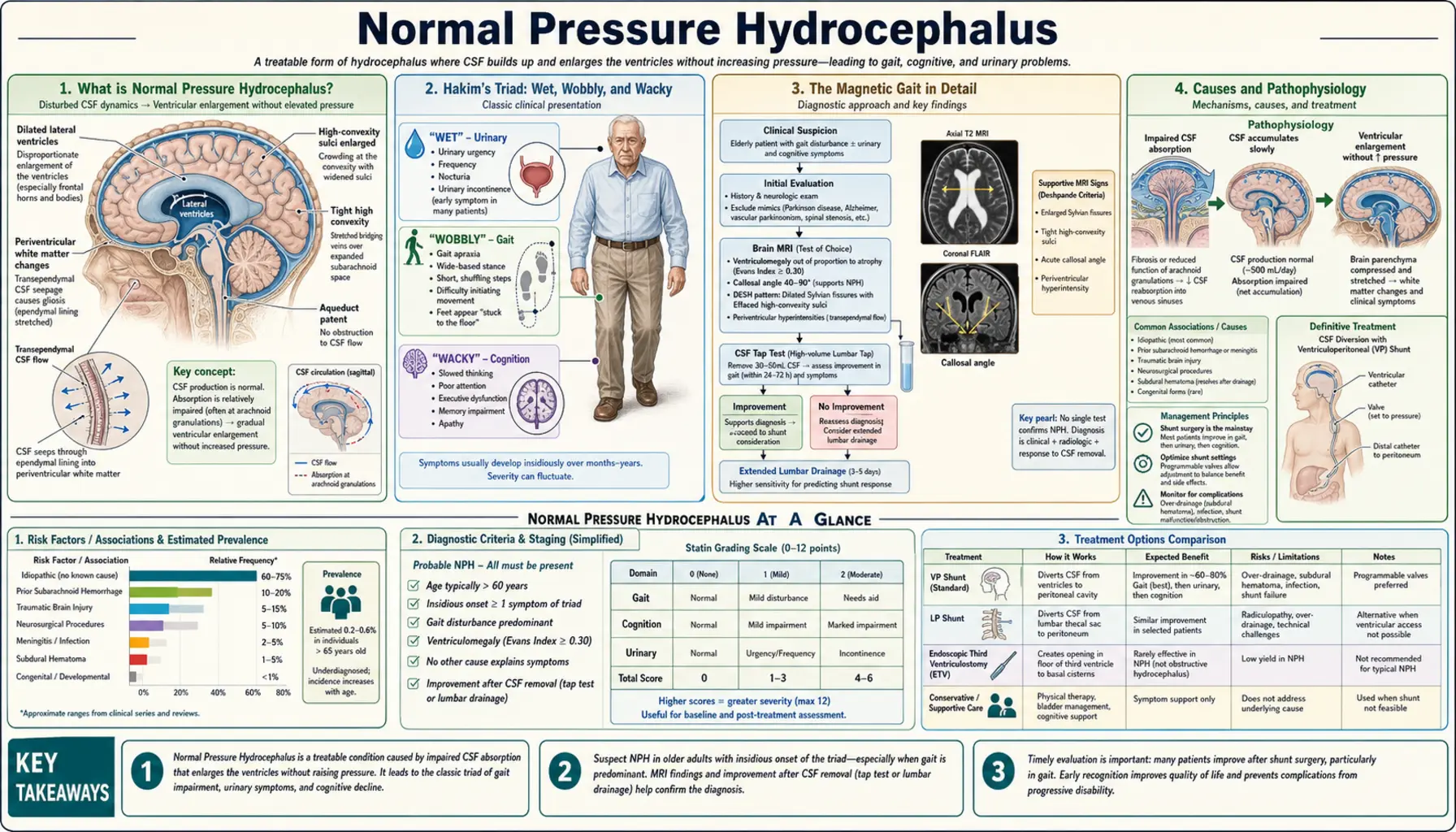
Table of Contents
- What is Normal Pressure Hydrocephalus?
- Hakim's Triad: Wet, Wobbly, and Wacky
- The Magnetic Gait in Detail
- Causes and Pathophysiology
- Diagnosis and Imaging
- Tap Test and Lumbar Drain Trial
- Treatment: VP Shunt Surgery
- Distinguishing From Other Dementias
- Prognosis and Outcomes
- Research Papers
- Connections
- Featured Videos
What is Normal Pressure Hydrocephalus?
Normal Pressure Hydrocephalus (NPH) is a potentially reversible neurological syndrome caused by the abnormal accumulation of cerebrospinal fluid (CSF) in the brain's ventricles. Unlike other forms of hydrocephalus, the CSF pressure measured on lumbar puncture is within the normal range — hence "normal pressure" — even though the ventricles are markedly enlarged.
NPH predominantly affects people over 60 and is significantly underdiagnosed. Estimates suggest it accounts for 5–10% of all dementia cases, making it one of the most common causes of treatable dementia in older adults. The condition was first described by Salomón Hakim and Raymond Adams in 1965.
The key importance of NPH is that it is one of the few causes of dementia where surgical treatment — inserting a shunt to drain the excess CSF — can produce substantial improvement, particularly in gait and urinary symptoms. Recognizing the classic triad early, before irreversible neuronal damage occurs, is essential.
Hakim's Triad: Wet, Wobbly, and Wacky
The classical presentation of NPH is captured in the Hakim's triad, memorably summarized as "wet, wobbly, and wacky" — referring to the three cardinal features:
1. Wet — Urinary Incontinence
Urinary incontinence in NPH is typically urge incontinence — the patient feels a sudden, compelling urge to urinate and may not make it to the bathroom in time. It results from compression of the periventricular fibers that carry signals between the frontal lobes and the micturition center in the brainstem. Unlike stress incontinence (leakage with coughing or sneezing), this is about urgency and frequency. The patient often has preserved awareness of the need to void but lacks the motor control to respond in time. In advanced NPH, true overflow incontinence or frank indifference to voiding can occur.
2. Wobbly — Gait Disturbance
Gait impairment is typically the first and most prominent symptom of NPH and the feature most likely to improve with treatment. The characteristic gait has been called the "magnetic gait" because the feet appear to be stuck to the floor. (See the next section for a detailed description.)
3. Wacky — Cognitive Impairment
The cognitive changes of NPH are a subcortical dementia pattern — characterized by psychomotor slowing (bradyphrenia), difficulty with executive function and attention, reduced motivation, and mild memory impairment. Language is typically preserved. This contrasts with Alzheimer's disease, which features prominent early language difficulties and severe memory impairment from cortical involvement.
Patients may appear apathetic, forgetful, or "slowed down." Families often describe the person as "not themselves" or "losing their spark." Depression is common. Unlike Alzheimer's, patients with NPH often have insight into their difficulties.
Important: All three features of the triad do not need to be present simultaneously for the diagnosis. The triad is complete in only about 50–60% of patients at presentation; gait disturbance alone (the most sensitive feature) should raise suspicion in the right demographic.
The Magnetic Gait in Detail
The magnetic gait of NPH is distinctive and, once seen, is usually recognizable. Understanding what it is — and what it is not — helps distinguish NPH from other common movement disorders in older adults.
Characteristics of the Magnetic Gait
- Wide-based stance: Feet are held wider apart than normal, increasing the base of support.
- Short steps with reduced height: Steps are small and shuffling. The feet barely clear the floor ("shuffle") but unlike Parkinson's, the step height is reduced rather than the step length being rhythmically shortened (festination).
- Reduced foot clearance — "magnetic" quality: The feet seem glued to the floor; patients have difficulty initiating steps and turning. The gait looks like the person is walking on ice and trying not to slip.
- Upright posture: Trunk is relatively upright, often with slight backward lean. This differentiates NPH from Parkinson's, where there is a characteristic stooped forward flexion of the trunk.
- En bloc turns: Turning is done in multiple small steps rather than pivoting smoothly.
- Normal arm swing: Arm swing is typically preserved in NPH — an important distinction from Parkinson's disease, where arm swing is reduced (often asymmetrically). This is a useful clinical discriminating feature.
What It Is NOT
- Not Parkinsonian gait: Parkinson's features resting tremor, rigidity, masked facies, festination (involuntary quickening of steps), stooped posture, and dramatically reduced arm swing — usually asymmetric at onset. NPH does not have resting tremor and arm swing is preserved.
- Not cerebellar ataxia: Cerebellar gait is wide-based and lurching with irregular step rhythm; the feet do clear the floor. Cerebellar ataxia also has dysmetria and intention tremor on examination.
- Not spastic gait: Spastic gait from upper motor neuron lesions features leg stiffness, circumduction (swinging the leg outward), and scissoring. Spasticity on examination and hyperreflexia are present.
Causes and Pathophysiology
NPH is classified as idiopathic (no identifiable cause, the majority) or secondary (due to an identifiable prior event).
Secondary NPH Causes
- Subarachnoid hemorrhage — most common secondary cause; blood products impair CSF resorption at the arachnoid granulations
- Traumatic brain injury
- Meningitis or encephalitis (inflammation scars the arachnoid granulations)
- Prior brain surgery
Pathophysiology
The mechanism is incompletely understood. The leading theory is impaired CSF resorption at the arachnoid granulations (the structures that drain CSF back into the venous system). Despite normal opening pressure on a single lumbar puncture, continuous intracranial pressure monitoring often reveals intermittent B-waves (pressure waves up to 50 mmHg) and elevated mean pressure, particularly at night. Over time, ventricular enlargement compresses and stretches the periventricular white matter — particularly the corticospinal and frontocortical fibers running close to the ventricles — producing the triad of symptoms.
The reason gait responds better than cognition is anatomical: the corticospinal tract fibers serving the legs course closest to the ventricular walls (the fibers from the legs are medially placed) and are therefore most susceptible to periventricular compression. Cortical association fibers involved in memory and higher cognition are farther away and may sustain irreversible ischemic damage if the condition goes untreated long enough.
Diagnosis and Imaging
Diagnosis requires clinical features plus supporting neuroimaging, and is confirmed by a positive response to CSF drainage.
MRI Brain — DESH Pattern
The characteristic MRI finding is DESH — Disproportionately Enlarged Subarachnoid-Space Hydrocephalus. This pattern includes:
- Markedly enlarged lateral and third ventricles (Evans' index ≥0.3 — the ratio of the widest diameter of the frontal horns to the widest inner diameter of the skull)
- Tight high-convexity and medial subarachnoid spaces — the subarachnoid spaces over the top and inner surfaces of the brain appear compressed or effaced, in contrast to the enlarged Sylvian fissures laterally. This mismatch is the hallmark of DESH.
- Callosal angle: On a coronal MRI slice at the posterior commissure, an angle between the medial surfaces of the parietal lobes of less than 90° (normal is wider) indicates medial surface crowding from ventricular expansion — a specific marker for NPH.
- Periventricular white matter changes: Common but not specific.
On CT, the finding is simpler: enlarged ventricles disproportionate to any cortical atrophy.
Lumbar Puncture
Opening pressure on LP is normal (usually 70–200 mmH₂O) — this is what distinguishes NPH from high-pressure hydrocephalus. A normal opening pressure does not exclude NPH; it is a required feature of the diagnosis. CSF analysis should be sent to exclude infection and inflammatory causes.
Tap Test and Lumbar Drain Trial
Before committing to shunt surgery, most centers assess whether the patient will respond to CSF drainage — this predicts surgical outcome.
High-Volume Tap Test (Large-Volume LP)
The most widely used screening procedure: remove 30–50 mL of CSF by lumbar puncture in a single session. Gait is assessed quantitatively before and at 1–4 hours, 24 hours, and sometimes 48–72 hours after the tap.
- A positive tap test (improvement in gait speed, step length, or timed up-and-go test by ≥10–20%) predicts a good shunt response in approximately 60–80% of cases.
- A negative tap test does not exclude shunt responsiveness — up to 20–30% of tap-test-negative patients still respond to shunting.
External Lumbar Drain Trial
For patients with a negative or equivocal tap test who remain strong shunt candidates clinically, an external lumbar drain (ELD) trial offers greater diagnostic accuracy. A drain is placed in the lumbar subarachnoid space and 150–300 mL of CSF is removed over 72–96 hours (approximately 10 mL/hour), with continuous gait and cognitive monitoring.
- ELD has a higher sensitivity (85–90%) than the single tap test for predicting shunt response.
- Risks include headache, infection (meningitis), and catheter dislodgement; must be performed inpatient with neurosurgical coverage.
Treatment: VP Shunt Surgery
The definitive treatment for NPH is ventriculoperitoneal (VP) shunt insertion — a surgically implanted catheter that continuously drains excess CSF from the lateral ventricle to the peritoneal cavity, where it is absorbed.
Shunt Design
Modern VP shunts use programmable valves that can be adjusted non-invasively with a magnetic programmer applied to the scalp — allowing the drainage rate to be fine-tuned after surgery without reoperation. This is important because under-drainage leaves symptoms untreated while over-drainage causes subdural hematomas from the brain pulling away from the skull.
Outcomes by Symptom Domain
- Gait: Best outcomes. Over 60–80% of patients show meaningful improvement in gait speed and balance within weeks to months of shunting. Some patients return to independent walking.
- Urinary incontinence: Responds well, though slightly less predictably than gait. Most patients experience significant improvement.
- Cognitive impairment: Least reliable improvement. Approximately 30–50% show cognitive gains. The presence of concomitant Alzheimer's or vascular disease limits cognitive recovery. Early treatment (before extensive cortical damage) is associated with better cognitive outcomes.
Surgical Risks
- Subdural hematoma from over-drainage (5–10%)
- Shunt infection (2–5%)
- Shunt malfunction requiring revision (cumulative ~30–40% over 10 years)
- Intracerebral hemorrhage from catheter placement (<1%)
Ventriculoatrial Shunt
An alternative when the peritoneal cavity is unavailable (e.g., prior abdominal surgeries or adhesions): the shunt drains into the right atrium of the heart via the internal jugular vein. Cardiac risks and thromboembolic complications are higher.
Distinguishing From Other Dementias
NPH is frequently misdiagnosed as Parkinson's disease or Alzheimer's disease in the primary care setting. The following table summarizes key distinguishing features:
- NPH vs. Alzheimer's disease: AD has early, prominent memory impairment with cortical atrophy on MRI (hippocampal atrophy) and lacks the magnetic gait. NPH has relatively preserved memory early, no cortical atrophy pattern, and gait is the dominant early feature. CSF biomarkers (amyloid, tau) help — they are abnormal in AD.
- NPH vs. Parkinson's disease: PD has resting tremor (NPH does not), asymmetric rigidity, stooped posture, reduced arm swing, and excellent initial response to levodopa. NPH arm swing is preserved; levodopa has no benefit in NPH. FDG-PET or DaT-SPECT scanning shows dopaminergic deficit in PD, not in NPH.
- NPH vs. Vascular dementia: Both can show white matter changes and step-wise cognitive decline. Vascular dementia is associated with multiple lacunar infarcts and focal neurological signs; NPH's ventricle-to-sulcal pattern (DESH) is different. The tap test helps discriminate.
- NPH vs. Parkinson's plus syndromes (PSP, MSA): PSP features early falls backward, supranuclear gaze palsy (inability to look downward voluntarily), and axial rigidity. MSA features early severe autonomic failure. Neither responds to shunting.
Prognosis and Outcomes
NPH has a better prognosis than most other causes of dementia, particularly when diagnosed and treated early. Gait improvement after shunting is durable in many patients, though re-evaluation is needed if symptoms recur (suggesting shunt malfunction).
- Duration of symptoms before shunting matters: Patients treated within 2 years of symptom onset have substantially better outcomes than those treated after many years of disability. This is partly because prolonged compression causes irreversible periventricular ischemia.
- Coexisting Alzheimer's pathology: Present in up to 30–50% of NPH patients at autopsy. Its presence blunts cognitive — but not necessarily gait — improvement after shunting.
- Long-term: Without treatment, NPH progresses to severe disability. With shunting, many patients maintain improved function for years, though shunt revisions are eventually needed by most patients.
Research Papers
Curated PubMed topic searches on normal pressure hydrocephalus. Each link opens a live PubMed query so the result set stays current as new studies are indexed.
- PubMed: Normal pressure hydrocephalus Hakim triad
- PubMed: DESH pattern MRI normal pressure hydrocephalus
- PubMed: Ventriculoperitoneal shunt idiopathic NPH outcomes
- PubMed: Tap test large volume CSF removal NPH prediction
- PubMed: External lumbar drain trial hydrocephalus shunt
- PubMed: NPH magnetic gait analysis quantitative
- PubMed: Normal pressure hydrocephalus Alzheimer coexisting pathology
- PubMed: NPH cognitive outcomes shunt surgery dementia
- PubMed: NPH versus Parkinson disease differential diagnosis
- PubMed: iNPH cerebrospinal fluid biomarkers
- PubMed: NPH shunt complications programmable valve
- PubMed: Hydrocephalus arachnoid granulations CSF absorption
Connections
- Neurology
- Alzheimer's Disease
- Vascular Dementia
- Parkinson's Disease
- Stroke
- TIA
- Essential Tremor
- Cerebellar Ataxia
- Huntington's Disease
- ALS
- Myasthenia Gravis
- Wernicke-Korsakoff Syndrome
- Multiple Sclerosis