Celiac Disease: History and Discovery
The story of celiac disease spans nearly two thousand years — from a Greek physician of the second century who named "the coeliac affection," through a London doctor's prescient Victorian lecture, to a Dutch pediatrician who solved the puzzle by watching starving children recover during a wartime famine. Its modern chapters — the biopsy view of a flattened intestine, the discovery of the autoantigen, and the mapping of the genes — turned an ancient mystery of "the belly" into one of the best-understood autoimmune diseases. This page traces that history with care, distinguishing who first described the illness from who later discovered its cause.
Table of Contents
- The Name: "Koiliakos" and the Belly
- Aretaeus of Cappadocia and the Ancient Description
- Samuel Gee and the First Modern Clinical Description (1888)
- Searching for the Cause: The Diet Theories
- Willem-Karel Dicke, Gluten, and the Hunger Winter
- Seeing the Damage: Villous Atrophy and the Biopsy Capsule
- An Autoimmune Disease: Transglutaminase and the Genes
- From Rare Childhood Illness to Common Diagnosis
- Research Papers and References
- Connections
- Featured Videos
The Name: "Koiliakos" and the Belly
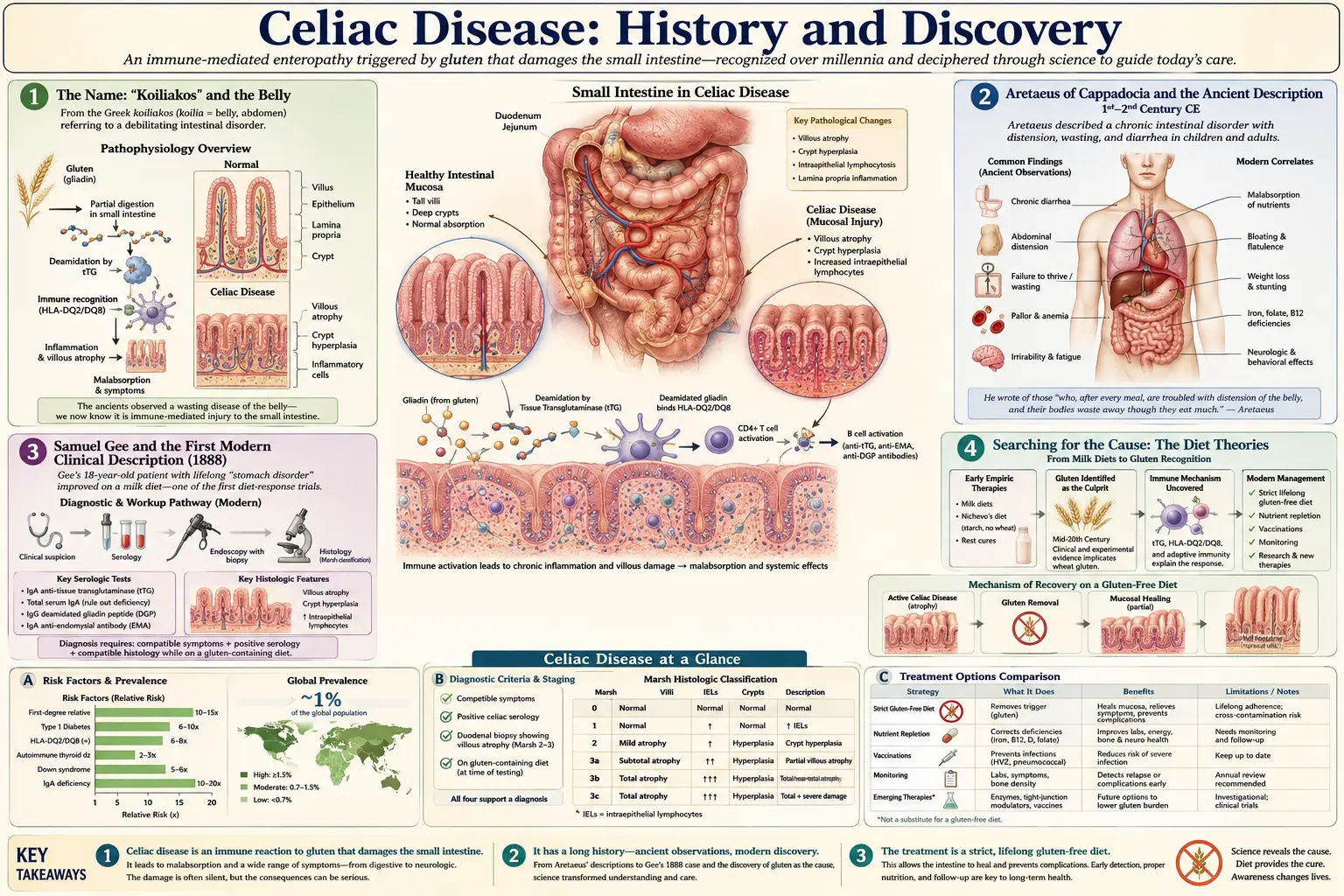
The word celiac (British spelling coeliac) is one of the oldest disease names still in everyday medical use, and it carries its origin on its surface. It descends from the ancient Greek koiliakos (κοιλιακóς), an adjective formed from koilia (κοιλια), meaning "belly," "abdomen," or "bowel." A koiliakos person was, quite literally, someone "suffering in the bowels." The term is purely descriptive: it names the seat of the symptoms — the abdomen — and makes no claim about cause, which would remain unknown for roughly eighteen more centuries.
That ancient root reminds us how the disease first presented itself to physicians: as a stubborn, wasting disorder of the gut marked by chronic diarrhea, pale and greasy stools, bloating, and a slow failure to thrive despite eating. For most of recorded history this cluster of symptoms could only be observed and named, not explained. The continuity of the word from a second-century Greek text to a twenty-first-century blood test is itself a small marvel of medical history — the label survived intact while everything underneath it was rewritten.
Aretaeus of Cappadocia and the Ancient Description
The earliest surviving description that physicians traditionally identify with celiac disease comes from Aretaeus of Cappadocia, a Greek physician usually dated to the second century CE (sometimes placed in the first century). In his writings on chronic diseases, Aretaeus devoted a chapter to what is rendered in Greek as the koiliakos condition — "the coeliac affection" — and it is from this text that the modern disease name is conventionally traced. Aretaeus described patients with a chronic diarrhea in which the food passed through undigested, accompanied by weakness, wasting, pallor, and thirst, and he noted that the condition was worse in adults, tended to be lasting, and was difficult to cure.
It is important to be precise about what Aretaeus did and did not accomplish. He was the first known describer of a chronic malabsorptive bowel disorder fitting the celiac picture, and he gave it the name we still use; he was emphatically not the discoverer of its cause. He had no concept of wheat, gluten, the immune system, or the small-intestinal lining. His account is a clinical portrait drawn from careful bedside observation, valuable precisely because it shows that this pattern of illness is ancient and was recognized as a distinct entity long before anything about its mechanism could be understood. The text was later edited and translated — Francis Adams's nineteenth-century English translation for the Sydenham Society is the version most often cited — which is part of why Aretaeus became firmly attached to the disease's history in the English-speaking medical world.
For many centuries after Aretaeus the trail goes largely cold. Scattered references to chronic diarrhea and "fluxes" appear in the medical literature, but no clearly recognizable, dedicated account of celiac disease as a defined entity reappears in a way that historians treat as a true advance until the late nineteenth century. The ancient name waited, in effect, for a modern observer to give it modern meaning.
Samuel Gee and the First Modern Clinical Description (1888)
That modern observer was Samuel Gee (1839–1911), an English physician at St Bartholomew's Hospital and the Hospital for Sick Children, Great Ormond Street, in London. Gee delivered a lecture on the condition that was published in 1888 in the St Bartholomew's Hospital Reports under the title "On the Coeliac Affection" — deliberately echoing Aretaeus, whose work Gee knew. His account is widely regarded as the first modern clinical description of celiac disease, and it is strikingly accurate. Gee described "a kind of chronic indigestion which is met with in persons of all ages, yet is especially apt to affect children between one and five years old," characterized by stools that were "loose, not formed, but not watery; more bulky than the food taken would seem to account for; pale in colour, as if devoid of bile; yellowish, frothy, stinking."
Gee's most prescient insight was about treatment. Without any knowledge of the cause, he reasoned from observation that diet was central, famously writing that "if the patient can be cured at all, it must be by means of diet." He even sensed that starchy, farinaceous foods were part of the problem — advising that "the allowance of farinaceous food must be small" — and he recorded a case of a child who thrived on a diet that included mussels but relapsed when the season for them ended. He had, in essence, glimpsed the right answer (food is the key, and the cereal-rich part of the diet is suspect) without being able to identify the specific culprit. It is worth stating plainly that this was an inspired clinical hypothesis, not a proven mechanism: Gee did not isolate gluten, and the precise dietary offender remained unidentified in his lifetime.
In the decades after Gee, physicians proposed and tested a series of dietary regimens for what was increasingly called "celiac disease" or "the celiac syndrome," especially in children. The best known is the American pediatrician Sidney V. Haas, who in 1924 reported apparent success with a "banana diet" that excluded most starches. The banana diet helped some children, and Haas became a strong advocate for it, but its rationale was mistaken — it worked, when it did, largely because it incidentally removed wheat and other gluten grains, not because of any special property of bananas. These early diets show medicine circling the correct conclusion for decades: that something in ordinary cereal foods was driving the illness.
Searching for the Cause: The Diet Theories
By the first half of the twentieth century, celiac disease was a recognized and feared diagnosis in pediatrics, but its cause remained genuinely unknown, and several competing theories were taken seriously. Some clinicians blamed fats; others blamed carbohydrates broadly; still others suspected an unidentified infection or a constitutional defect of the child. Treatment was largely a matter of trial and error with restrictive diets, and outcomes were often poor — severe celiac disease in children could be fatal, and "celiac crisis," a state of acute dehydration and collapse, was a real and dangerous event.
The key conceptual obstacle was that the offending substance was hidden inside one of the most basic and universal foods: bread. Wheat was so fundamental to the European and American diet that it was difficult to imagine, let alone test, the idea that ordinary flour was a poison to these patients. Isolating that single variable would have required either an extraordinarily controlled experiment or an accident of history that removed wheat from a population's diet while doctors watched. As it happened, the Second World War supplied exactly such an accident.
Willem-Karel Dicke, Gluten, and the Hunger Winter
The person who finally identified the cause was the Dutch pediatrician Willem-Karel Dicke (1905–1962). Dicke had a long-standing interest in childhood celiac disease and, working in the Netherlands through the 1930s and 1940s, had already come to suspect — partly from parents' reports that symptoms flared after bread or biscuits — that wheat flour was the trigger and that removing it helped. What he lacked was decisive proof. That proof was supplied, tragically, by the Dutch "Hunger Winter" of 1944–1945, a famine in the German-occupied western Netherlands during which bread and flour became extremely scarce.
Dicke observed something that ran exactly counter to ordinary expectation: during the famine, his celiac patients improved even as the general population starved, because the food they could no longer get — wheat bread — was the very thing harming them. When Allied relief restored bread to the diet after liberation, those same children relapsed. This natural experiment, layered on top of his earlier clinical suspicion, gave Dicke the evidence he needed. It is fair to call the Hunger Winter the moment that confirmed the wheat hypothesis, while crediting Dicke's prior decade of careful observation for the hypothesis itself; the popular telling that he "discovered the cause during the famine" compresses a longer story, but its core is true.
Dicke and his collaborators then did the rigorous work. In his 1950 doctoral thesis (Utrecht) and in subsequent studies around 1952–1953 — including foundational work with J. H. van de Kamer and H. A. Weijers using careful measurement of fecal fat to quantify the effect — he demonstrated that it was specifically the wheat protein (gluten) fraction, not the starch or carbohydrate, that caused the malabsorption and damage, and that removing gluten reversed it. This is the origin of the modern gluten-free diet, still the only established treatment for celiac disease today. Dicke is therefore correctly remembered as the discoverer of the cause (gluten) and the founder of dietary therapy — a separate and later achievement from Aretaeus's naming of the disease and Gee's clinical description of it.
Seeing the Damage: Villous Atrophy and the Biopsy Capsule
Knowing that gluten caused the illness still left a physical question: what was gluten actually doing inside the patient? The answer came from the small intestine. In 1954, the British physician John W. Paulley reported that full-thickness intestinal specimens obtained at surgery (laparotomy) from patients with celiac-type malabsorption showed a striking abnormality of the lining — the normally tall, finger-like villi that absorb nutrients were flattened and atrophied, with inflammation beneath. Paulley's work is generally credited as the first clear description of the characteristic intestinal lesion of celiac disease. This finally tied the dietary cause to a visible tissue injury: gluten was flattening the absorptive surface of the gut.
Surgery was far too drastic to use for routine diagnosis, however. The breakthrough that made the celiac lesion accessible was the development of peroral small-intestinal biopsy — a way to sample the gut lining through a swallowed instrument, without an operation. In 1956, the physician Margot Shiner (1923–1998), working in London, published in The Lancet a flexible biopsy tube that could be passed by mouth down into the small intestine to retrieve mucosal samples in living patients, including children. Shortly afterward, in 1957, the American physicians William H. Crosby and H. W. Kugler described the suction biopsy capsule that bears their name (the Crosby–Kugler capsule), a swallowed device that used suction and a spring-loaded blade to cut a small piece of intestinal lining.
These instruments transformed celiac disease from a condition diagnosed by guesswork and dietary response into one that could be confirmed by directly examining the intestinal lining for villous atrophy — and re-examining it to prove healing on a gluten-free diet. The intestinal biopsy became, for decades, the diagnostic gold standard, later refined by the Marsh classification (Michael Marsh, 1992) that graded the spectrum of mucosal change from mild lymphocyte infiltration to complete villous flattening. Endoscopic biopsy eventually replaced the swallowed capsule, but the principle Paulley, Shiner, Crosby, and Kugler established — look at the villi — remains central to diagnosis.
An Autoimmune Disease: Transglutaminase and the Genes
The final reframing of celiac disease in the late twentieth century was the recognition that it is not a simple food intolerance or allergy but a genuine autoimmune disease — one in which the immune system, provoked by gluten, attacks the body's own tissue. Two lines of evidence cemented this view: the genetics of the disease and the identification of its self-target (autoantigen).
On the genetic side, researchers established a strong association between celiac disease and specific human leukocyte antigen (HLA) immune-system genes. Beginning with HLA-B8 associations reported around 1972 and refined over the following two decades, the field converged on the class II genes HLA-DQ2 and HLA-DQ8: nearly everyone with celiac disease carries one or both, and their absence makes the disease extremely unlikely. This explained why celiac disease runs in families and provided, eventually, a genetic test that is most useful for ruling the disease out. (The HLA story is developed in the dedicated genetic-testing sub-article.)
The decisive molecular discovery came in 1997, when Walburga Dieterich, Detlef Schuppan, and colleagues in Germany (with Italian collaborators) identified the long-sought endomysial autoantigen of celiac disease as the enzyme tissue transglutaminase (tTG), publishing their result in Nature Medicine. They further showed that tissue transglutaminase chemically modifies gliadin (a gluten fraction), creating the very epitopes that drive the immune attack — an elegant link between the dietary trigger and the autoimmune response. This discovery did not just explain the disease; it created the modern anti-tTG antibody blood test, which made large-scale, non-invasive screening possible and is the main reason far more cases are now detected. (Antibody testing is covered in detail in the serology sub-article.)
From Rare Childhood Illness to Common Diagnosis
For most of its history, celiac disease was thought of as a relatively uncommon and mainly pediatric disorder — the wasting "celiac child" of the textbooks. The arrival of reliable blood tests in the 1990s and 2000s overturned that picture. Population screening using anti-tTG and related antibodies revealed that celiac disease is common, affecting roughly 1 in 100 people in many Western populations, that it frequently presents in adults, and that a large share of cases are "silent" or atypical — causing anemia, osteoporosis, fatigue, infertility, or neurological symptoms rather than the classic diarrhea. Most people with celiac disease, it turned out, had never been diagnosed at all.
The history of celiac disease is thus a model of how medical understanding accumulates in distinct, separable steps. Aretaeus named the pattern from the belly's symptoms; Samuel Gee described it precisely and guessed that diet was the cure; Willem-Karel Dicke, aided by the grim natural experiment of the Hunger Winter, proved that the cause was wheat gluten and built the gluten-free diet; Paulley, Shiner, Crosby, and Kugler made the intestinal damage visible; and Dieterich, Schuppan, and the HLA researchers revealed it as a gluten-driven autoimmune disease with a defined genetic basis and a specific self-target. Each contributor solved a different piece, and conflating "first describer" with "cause discoverer" obscures the real shape of the story.
Today the gluten-free diet that Dicke pioneered remains the cornerstone of treatment, while research pushes toward enzyme therapies, immune-modulating drugs, and even vaccines that might one day let patients tolerate gluten. The ancient name endures, but the illness it labels is now understood from the level of a population statistic down to the chemistry of a single enzyme — a journey from "the coeliac affection" of the second century to molecular medicine in our own.
Research Papers and References
The references below combine landmark historical papers in the discovery of celiac disease with curated PubMed topic-search links into the historical and clinical literature. Where a specific peer-reviewed source is cited with confidence, a DOI or PMID link is given; broader topics link to a PubMed search. Historical primary texts — Aretaeus's account of "the coeliac affection," Samuel Gee's 1888 lecture "On the Coeliac Affection" in the St Bartholomew's Hospital Reports, and Dicke's 1950 Utrecht thesis — are named in the article as historical sources. Each link opens at its publisher or at PubMed (National Library of Medicine) in a new tab.
- Losowsky MS. A history of coeliac disease. Digestive Diseases. 2008;26(2):112-120. — doi:10.1159/000116768
- Dowd B, Walker-Smith J. Samuel Gee, Aretaeus, and the coeliac affection. British Medical Journal. 1974;2(5909):45-47. — doi:10.1136/bmj.2.5909.45
- Gee S. On the coeliac affection. St Bartholomew's Hospital Reports. 1888;24:17-20 (historical primary source). — PubMed: Gee and the coeliac affection
- van Berge-Henegouwen GP, Mulder CJ. Pioneer in the gluten free diet: Willem-Karel Dicke 1905-1962, over 50 years of gluten free diet. Gut. 1993;34(11):1473-1475. — doi:10.1136/gut.34.11.1473
- Dieterich W, Ehnis T, Bauer M, Donner P, Volta U, Riecken EO, Schuppan D. Identification of tissue transglutaminase as the autoantigen of celiac disease. Nature Medicine. 1997;3(7):797-801. — doi:10.1038/nm0797-797
- Paulley JW. Observation on the aetiology of idiopathic steatorrhoea; jejunal and lymph-node biopsies. British Medical Journal. 1954;2(4900):1318-1321. — doi:10.1136/bmj.2.4900.1318
- Shiner M. Duodenal biopsy. The Lancet. 1956;267(6906):17-19 (peroral small-intestinal biopsy). — PubMed: Shiner peroral intestinal biopsy
- Crosby WH, Kugler HW. Intraluminal biopsy of the small intestine; the intestinal biopsy capsule. American Journal of Digestive Diseases. 1957;2(5):236-241. — doi:10.1007/BF02231100
- Marsh MN. Gluten, major histocompatibility complex, and the small intestine. A molecular and immunobiologic approach to the spectrum of gluten sensitivity ("celiac sprue"). Gastroenterology. 1992;102(1):330-354. — doi:10.1016/0016-5085(92)91819-P
- Sollid LM. The roles of MHC class II genes and post-translational modification in celiac disease. Immunogenetics. 2017;69(8-9):605-616. — doi:10.1007/s00251-017-0985-7
- Yan D, Holt PR. Willem Dicke. Brilliant clinical observer and translational investigator. Discoverer of the toxic cause of celiac disease. Clinical and Translational Gastroenterology. 2010;1(1):e9. — doi:10.1038/ctg.2010.9
- Haas SV. The value of the banana in the treatment of celiac disease (historical). — PubMed: Haas banana diet and celiac history
- HLA-DQ2 and HLA-DQ8 association with celiac disease — PubMed: celiac disease HLA-DQ2 / DQ8 genetics
- History and discovery of celiac disease — from Aretaeus to molecular medicine — PubMed: celiac disease history (Aretaeus, Gee, Dicke)
External Authoritative Resources
- NIDDK (NIH) — Celiac Disease
- Celiac Disease Center at Columbia University
- PubMed — All research on the history of celiac disease
Connections
- Gastroenterology
- Celiac Disease (Main Article)
- Gluten-Free Diet: A Practical Guide
- Endoscopy, Biopsy, and Marsh Classification
- Celiac Serology Testing (tTG, DGP, EMA)
- HLA-DQ2 and HLA-DQ8 Genetic Testing
- Non-Celiac Gluten Sensitivity
- Irritable Bowel Syndrome
- Inflammatory Bowel Disease
- Hashimoto's Thyroiditis
- All Conditions