Peripheral Arterial Disease
Interactive Visualization Nitric Oxide — make an artery relax Watch the endothelium turn L-arginine into nitric oxide and widen the artery — then let oxidative stress uncouple eNOS and stiffen it, or pour in beet nitrate to rescue the flow. Launch →
Table of Contents
- Overview
- Epidemiology
- Pathophysiology
- Risk Factors
- Clinical Spectrum
- Ankle-Brachial Index (ABI)
- Classification Systems
- Diagnosis
- Medical Management
- Supervised Exercise and Lifestyle
- Revascularization and Critical Limb Ischemia
- Research Papers
- Connections
- Featured Videos
1. Overview
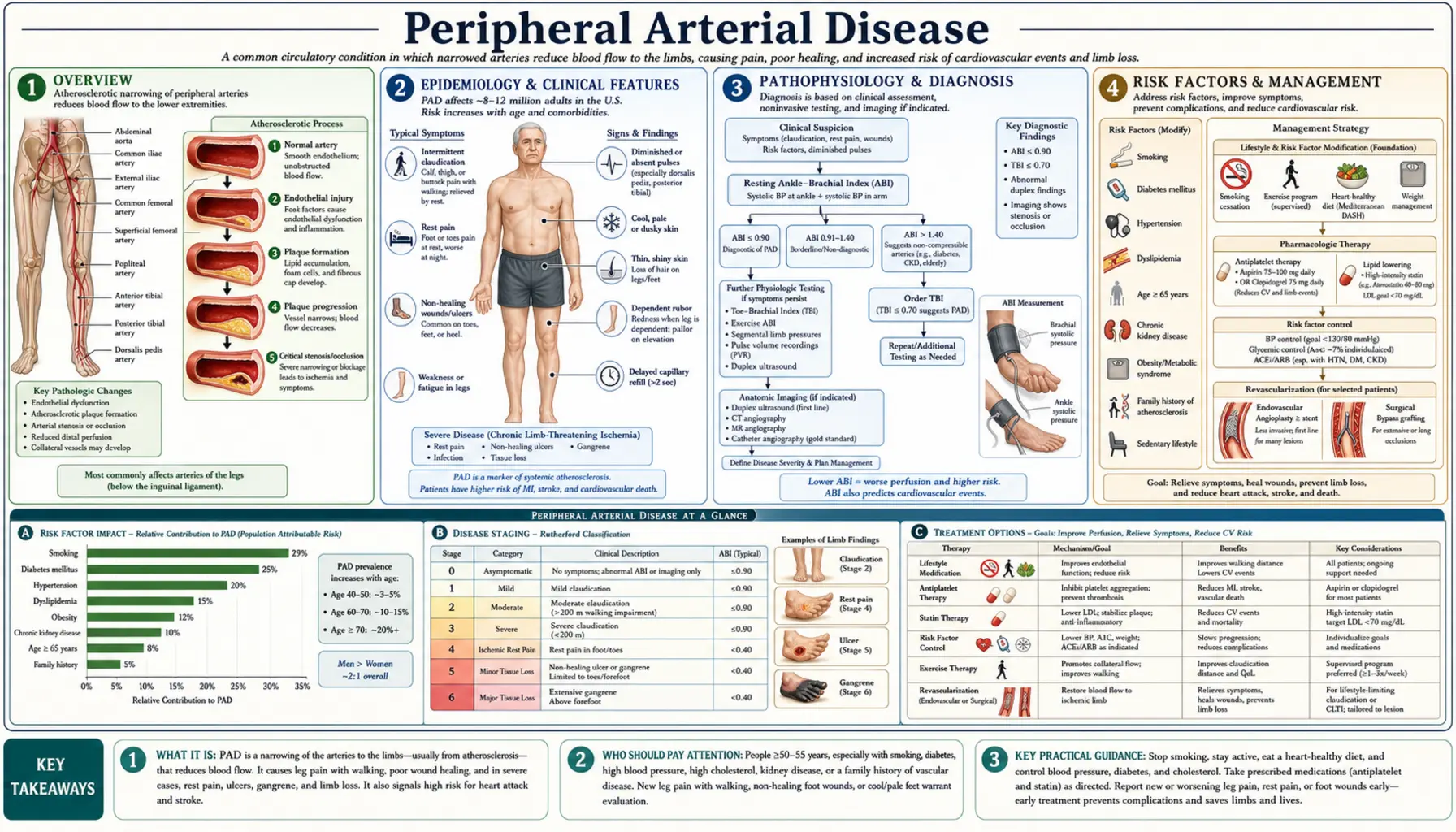
Peripheral arterial disease (PAD) is a manifestation of systemic atherosclerosis in which plaque accumulation narrows the lumen of arteries supplying the extremities — predominantly the lower limbs — reducing blood flow and oxygen delivery to the muscles and tissues downstream. PAD is the third leading cause of atherosclerotic cardiovascular morbidity worldwide, after coronary artery disease and stroke, yet it remains substantially underdiagnosed and undertreated relative to those better-known conditions.
The defining pathological process is atherosclerotic stenosis or occlusion of the aortoiliac, femoropopliteal, or tibial/peroneal arterial segments. As plaques enlarge and calcify over decades, the cross-sectional lumen narrows until blood flow can no longer meet the metabolic demands of exercising muscle — producing the hallmark symptom of intermittent claudication. In its most severe form, PAD reduces flow so critically that even resting tissues cannot receive adequate oxygen, causing critical limb-threatening ischemia (CLTI) — rest pain, non-healing wounds, and gangrene that may necessitate limb amputation.
What makes PAD particularly important beyond the limb itself is its role as a systemic vascular risk marker. Patients with PAD have a 3- to 6-fold increased risk of myocardial infarction and a 2- to 4-fold increased risk of stroke compared with people without PAD, because the same atherosclerotic process that narrows leg arteries is simultaneously advancing in the coronary and carotid circulations. Approximately 60% of symptomatic PAD patients have significant coronary artery disease (CAD), and a similar fraction have associated cerebrovascular disease. The 5-year cardiovascular mortality in patients with PAD exceeds that of many cancers — roughly 20–30% in symptomatic patients.
Despite this burden, PAD is often diagnosed late, partially because the majority of patients — an estimated 50–80% — are asymptomatic or have atypical symptoms misattributed to arthritis, lumbar radiculopathy, or normal aging. Systematic use of the ankle-brachial index (ABI), a simple, inexpensive, non-invasive hemodynamic test, can identify PAD long before limb-threatening complications develop. Earlier recognition enables aggressive cardiovascular risk-factor modification, supervised exercise therapy, antiplatelet and statin therapy, and — when required — timely revascularization to preserve the limb.
2. Epidemiology
PAD affects an estimated 8–12 million Americans and approximately 236 million people worldwide — making it one of the most prevalent cardiovascular conditions globally. A landmark 2013 analysis by Fowkes et al. ( — Search PubMed) estimated global PAD prevalence at 13.1% in high-income countries and 12.0% in low- and middle-income countries among adults aged 25 and older, with the total burden increasing by 23.5% from 2000 to 2010 as populations aged and diabetes rates rose.
Age is the dominant demographic predictor. PAD prevalence is under 3% in individuals below age 50, rises to 8–10% in those aged 60–69, and reaches 15–20% in adults over age 70. The dramatic age-dependence reflects the decades-long accumulation of atherosclerotic plaque — PAD is largely a disease of cumulative vascular injury. Men have a modestly higher overall prevalence than women in most high-income population studies, though sex differences attenuate at older ages. Notably, women with PAD are more likely to have atypical or absent claudication, leading to delayed diagnosis.
Racial and ethnic disparities are pronounced. Non-Hispanic Black Americans have a PAD prevalence approximately twice that of non-Hispanic White Americans — a disparity driven by higher rates of hypertension, diabetes, smoking, and chronic kidney disease, as well as possible genetic and social determinants of health. Hispanic Americans have intermediate prevalence. These disparities are compounded by differential access to vascular specialty care; Black patients with CLTI have substantially higher rates of major limb amputation and lower rates of revascularization compared with White patients, even after adjusting for disease severity.
Geographic variation is substantial. Prevalence is highest in South and Southeast Asia and sub-Saharan Africa in absolute numbers due to population size and rising diabetes epidemics. In the United States, the Southeast — the "Stroke Belt" — has disproportionately high PAD burden, correlating with regional patterns of smoking, obesity, and diabetes. Urban-rural disparities also exist, with rural populations having higher prevalence and lower access to vascular imaging and intervention.
Economic burden: PAD imposes enormous healthcare costs. In the US alone, PAD-related hospitalizations exceed 1 million annually, and the estimated direct and indirect costs exceed $21 billion per year. Patients with CLTI requiring hospitalization, endovascular or surgical revascularization, wound care, and amputation rehabilitation represent a disproportionate share of this cost. Amputation — the endpoint that PAD management aims to prevent — carries a 1-year mortality of 50–70% in CLTI patients, comparable to many advanced cancers.
3. Pathophysiology
The pathophysiology of PAD is fundamentally that of atherosclerosis in the peripheral circulation, with several features distinguishing it from coronary or cerebrovascular disease: the predominance of calcification, the central role of diabetes in accelerating tibial disease, and the unique physiology of skeletal muscle ischemia under exercise versus rest conditions.
Atherosclerotic Plaque Development
The process begins with endothelial dysfunction — a disruption of the normal anti-inflammatory, antithrombotic, and vasodilatory properties of the arterial endothelium. Shear stress disturbances at arterial bifurcations and curvatures (particularly the aortoiliac bifurcation, the femoral bifurcation in the groin, and the popliteal trifurcation behind the knee) promote the expression of adhesion molecules and chemokines, attracting monocytes into the subintimal space. There, monocytes differentiate into macrophages and engulf oxidized low-density lipoprotein (LDL) particles to form lipid-laden foam cells — the cellular hallmark of early atherosclerosis.
Over decades, foam cell accumulation, smooth muscle cell migration from the media, extracellular matrix deposition, and neovascularization build a progressively enlarging fibrous plaque that protrudes into the arterial lumen. The plaque's fibrous cap separates its lipid-rich, necrotic core from the flowing bloodstream. Plaque rupture or erosion exposes the prothrombotic core, triggering platelet aggregation and acute thrombus formation — a mechanism that, in the coronary circulation, produces myocardial infarction, and in the peripheral circulation, can produce acute limb ischemia.
Calcification and Medial Sclerosis
In the peripheral vasculature — particularly the tibial arteries of diabetic and CKD patients — medial calcification (Monckeberg's sclerosis) occurs alongside or instead of intimal atherosclerosis. In medial sclerosis, calcium deposits accumulate within the arterial media, hardening the wall without necessarily obstructing the lumen. This calcification renders vessels non-compressible and falsely elevates ankle pressures, producing spuriously normal or high ABI readings (>1.40) that underestimate true hemodynamic impairment. Toe-brachial index (TBI) measurement — using photoplethysmography at the toe, where digital arteries are less affected by medial calcification — is essential in these patients.
Exercise Physiology and Claudication
At rest, even significantly stenosed arteries may provide adequate blood flow to meet the low oxygen demands of resting muscle. During exercise, however, skeletal muscle oxygen demand increases 10- to 20-fold — a demand that requires a proportional increase in blood flow. Stenotic or occluded arteries cannot deliver this increment. Downstream, anaerobic metabolism increases, lactate and other metabolites accumulate in the interstitium, and pain receptors in the muscle are activated, producing the characteristic claudication pain — cramping or aching in the calf (most common), thigh, or buttock depending on the location of the occlusion.
Stopping exercise immediately relieves the ischemic demand; metabolites are cleared and pain resolves within 2–5 minutes of standing rest — a temporal pattern that distinguishes claudication from musculoskeletal or neurogenic causes of exertional leg pain. Walking uphill or faster shortens the distance to claudication onset; walking on flat ground more slowly extends it.
Collateral Circulation
The body responds to progressive arterial occlusion by arteriogenesis — the remodeling and enlargement of pre-existing collateral vessels stimulated by increased shear stress and local growth factors (VEGF, FGF). Effective collateral development can partially compensate for main-channel occlusion, explaining why some patients with complete femoral artery occlusion on imaging have only mild claudication while others with lesser stenoses have severe symptoms. Supervised exercise training is a potent stimulus for collateral development — it is the most effective intervention for claudication.
Critical Limb Ischemia
When stenoses progress to multiple-level disease with inadequate collateral compensation, resting blood flow falls below the threshold for tissue viability. The skin and subcutaneous tissues — especially of the toes and distal foot — begin to receive insufficient oxygen even without the added metabolic demand of exercise. The result is ischemic rest pain (typically burning, constant pain in the forefoot and toes, relieved partially by hanging the foot dependent to increase perfusion by gravity), ischemic ulceration at pressure points or minor trauma sites, and ultimately gangrene of digits or the foot. This stage — now termed CLTI (chronic limb-threatening ischemia) — represents end-stage PAD and carries the highest risk of amputation and death.
4. Risk Factors
PAD shares the classic atherosclerotic risk factor profile with coronary artery disease and cerebrovascular disease, but the relative magnitudes differ importantly. Tobacco use and diabetes exert particularly strong effects in the peripheral circulation.
Tobacco Use (Strongest Modifiable Risk Factor)
Smoking is the single most powerful modifiable risk factor for PAD, conferring a 2- to 4-fold increased risk of developing the disease. The risk is dose-dependent — heavier and longer-duration smokers have greater risk — and persists for years after cessation, though quitting substantially reduces progression and improves outcomes. Smoking accelerates atherosclerosis through endothelial dysfunction, oxidative stress, platelet activation, reduced prostacyclin production, and impaired fibrinolysis. Approximately 80% of patients with symptomatic PAD are current or former smokers. In patients who continue to smoke after PAD diagnosis, the risk of progressing to CLTI and requiring amputation is dramatically higher compared with those who quit.
Diabetes Mellitus (Strongest Risk Factor for Amputation)
Diabetes confers a 3- to 4-fold increased risk of PAD and is the most important risk factor for major limb amputation once PAD is established. Several mechanisms converge in diabetes to produce especially severe PAD: accelerated tibial artery disease (the below-knee vessels are preferentially affected, making revascularization more technically challenging), peripheral neuropathy (which impairs pain perception and delays presentation), impaired wound healing from reduced neutrophil function and growth factor signaling, and medial calcification that renders vessels non-compressible. Diabetic patients with PAD are 10 to 20 times more likely to require amputation than non-diabetic PAD patients — a stark inequality that underscores the need for aggressive foot surveillance and glycemic control.
Hypertension
Hypertension is strongly associated with PAD, with relative risk estimates of 1.5- to 2-fold in most population studies. The mechanism involves sustained wall stress, endothelial dysfunction from oxidative stress, and accelerated intimal plaque deposition. The association is particularly strong in African Americans, in whom hypertension is more prevalent, more severe, and more likely to be undertreated. Blood pressure control with a target below 130/80 mmHg reduces cardiovascular events in PAD patients, though aggressive lowering below 120 mmHg in patients with CLTI may paradoxically reduce distal perfusion pressure and worsen ischemia.
Dyslipidemia
Elevated LDL cholesterol promotes plaque formation in peripheral arteries through the same mechanisms as in the coronary circulation. High-intensity statin therapy reduces PAD progression, the rate of major adverse limb events (MALE), and systemic cardiovascular events. Low HDL cholesterol and elevated triglycerides (features of the metabolic syndrome) are independently associated with PAD risk. Beyond lipids, elevated Lp(a) — a genetically determined lipoprotein particle — is an emerging independent risk factor for PAD, and emerging targeted therapies (inclisiran, PCSK9 inhibitors) may specifically reduce Lp(a)-associated vascular risk.
Chronic Kidney Disease
CKD amplifies PAD risk substantially. Patients with an eGFR below 60 mL/min/1.73m² have a 2- to 3-fold higher PAD prevalence than those with normal renal function, and this risk rises steeply with worsening kidney function. CKD promotes vascular calcification (through phosphate retention and disordered mineral metabolism), endothelial dysfunction, and a chronically inflamed, prothrombotic state. The combination of CKD and diabetes is particularly devastating — such patients develop diffuse, heavily calcified tibial disease that is resistant to both endovascular and surgical revascularization.
Other Risk Factors
Additional established risk factors include age over 65 (or over 50 with one additional risk factor), male sex (though sex differences narrow at older age), elevated C-reactive protein (reflecting systemic inflammation), hyperhomocysteinemia (which impairs endothelial nitric oxide production), hypercoagulable states (antiphospholipid syndrome, factor V Leiden — relevant particularly for acute limb ischemia), and a personal or family history of coronary or cerebrovascular disease.
5. Clinical Spectrum
PAD presents across a wide clinical spectrum — from completely asymptomatic disease discovered incidentally, to classic intermittent claudication, to limb-threatening ischemia. Understanding this spectrum is essential for appropriate triage, counseling, and intervention decisions.
Asymptomatic PAD (50–80% of Cases)
The majority of individuals with PAD — estimated at 50–80% in population studies using ABI-based definitions — have no classic claudication symptoms. Many are truly asymptomatic, while others have reduced their activity level to below the ischemic threshold without recognizing the cause. Still others have peripheral neuropathy (as in diabetes) that blunts the pain signal of ischemia. Asymptomatic PAD still carries the full systemic cardiovascular risk of symptomatic disease — such patients have the same elevated rates of MI and stroke — and they warrant the same risk-factor modification and antiplatelet/statin therapy as symptomatic patients.
Intermittent Claudication
Intermittent claudication (IC) is the hallmark symptomatic presentation of PAD. The term derives from the Latin claudicare — to limp — reflecting the limping gait that develops as patients protect the ischemic limb during walking. Patients describe reproducible, predictable cramping, aching, tightening, or fatigue in specific muscle groups during walking, which resolves completely with 2–5 minutes of standing rest (not sitting, which is important diagnostically — true claudication does not require sitting).
The location of claudication symptoms maps to the level of arterial occlusion:
- Calf claudication (most common): occlusion in the superficial femoral or popliteal arteries.
- Thigh claudication: occlusion at the common femoral artery or proximal superficial femoral artery.
- Buttock and hip claudication (Leriche syndrome): aortoiliac occlusive disease; in men, this is classically accompanied by erectile dysfunction from reduced internal iliac artery flow.
- Foot claudication: tibial/peroneal disease, most common in diabetics.
The absolute claudication distance (ACD) — the distance walked before onset of pain — and the pain-free walking distance are key clinical metrics for monitoring symptom severity over time and assessing response to therapy. A standardized treadmill claudication test (typically 3.2 km/h at 12% grade) provides objective quantification.
Critical Limb-Threatening Ischemia (CLTI)
CLTI represents the severe end of PAD and is defined by the triad of ischemic rest pain, non-healing wounds (ischemic ulcers or gangrene), and hemodynamic evidence of severe arterial insufficiency (ABI <0.40, ankle pressure <50 mmHg, or toe pressure <30 mmHg). Approximately 1–3% of symptomatic PAD patients per year progress to CLTI; the annual incidence in the US is estimated at 150,000–200,000 patients.
Ischemic rest pain is a constant, burning, or gnawing pain in the toes and forefoot, typically worse at night when the foot is horizontal (gravity can no longer assist perfusion). Patients characteristically hang the foot dependently over the bed edge or sleep in a chair — this dependent position slightly increases hydrostatic pressure and marginally improves distal flow, providing partial relief.
Ischemic ulcers are a distinguishing feature of CLTI. They differ fundamentally from venous or neuropathic ulcers:
- Location: toes, toe web spaces, heel (pressure points), or sites of minor trauma. Venous ulcers occur at the medial malleolus; neuropathic ulcers at pressure points on the plantar surface.
- Appearance: pale, necrotic base with minimal or absent granulation tissue (reflecting absent perfusion); punched-out edges; minimal exudate. Venous ulcers have a moist, sloughy base with surrounding venous stasis changes (lipodermatosclerosis, hemosiderin staining).
- Pain: ischemic ulcers are typically very painful (unless neuropathy is present); venous ulcers are less painful and often relieved by leg elevation.
Without revascularization, CLTI carries a 1-year amputation rate of 25–30% and a 1-year mortality of 25% — a prognosis that rivals many advanced malignancies and underscores the urgency of expert vascular evaluation.
Acute Limb Ischemia
Acute limb ischemia (ALI) is a sudden reduction in limb perfusion that threatens tissue viability, classified as a separate syndrome from chronic PAD though often occurring on a background of pre-existing atherosclerotic disease. The causes include acute thrombosis of a stenotic native artery, embolism (usually from the heart — AF, LV thrombus — or proximal arterial aneurysm), or bypass graft occlusion. The clinical hallmarks are the "6 Ps": Pain, Pallor, Pulselessness, Paresthesias, Paralysis, and Poikilothermia (coldness). Paresthesias and paralysis signal impending irreversible ischemia and represent a vascular emergency requiring revascularization within hours to avoid permanent limb loss.
6. Ankle-Brachial Index (ABI)
The ankle-brachial index (ABI) is the gold-standard diagnostic and screening test for PAD — inexpensive, non-invasive, reproducible, and strongly predictive of both PAD severity and systemic cardiovascular prognosis. It is the single most valuable tool in the initial evaluation of any patient suspected to have PAD.
Measurement Technique
ABI is measured with the patient supine at rest for at least 5 minutes. A handheld Doppler probe (typically 8 MHz) is used to detect audible arterial flow signals while a standard blood pressure cuff is inflated and deflated above each measurement site. Systolic pressures are recorded at:
- Both brachial arteries (right and left)
- Both dorsalis pedis arteries (dorsum of foot)
- Both posterior tibial arteries (behind the medial malleolus)
The ABI for each leg is calculated as:
ABI = Highest ankle systolic pressure (dorsalis pedis or posterior tibial) / Highest brachial systolic pressure
The higher brachial pressure is used in the denominator to avoid falsely elevating ABI if one arm has a subclavian stenosis. Each leg is calculated separately; the lower of the two leg values is the diagnostic ABI for that patient.
Interpretation
- Normal: 1.00–1.40 — no significant arterial obstruction.
- Borderline: 0.91–0.99 — possible early PAD; warrants repeat measurement or further evaluation especially with symptoms or risk factors.
- PAD: <0.90 — diagnostic of significant arterial obstruction. This is the accepted diagnostic threshold in all major guidelines (AHA/ACC 2016).
- Moderate PAD: 0.50–0.89 — corresponds clinically to most patients with claudication.
- Severe PAD: <0.50 — high risk of CLTI; rest pain and tissue loss are common at this level.
- Non-compressible vessels: >1.40 — indicates medial arterial calcification (common in diabetes and CKD); ankle pressure is falsely elevated and does not reflect true hemodynamics. Requires alternative testing.
ABI as a Cardiovascular Risk Marker
Even mildly reduced ABI values in the range of 0.70–0.89 are associated with substantially increased cardiovascular mortality. A 2012 meta-analysis ( — Search PubMed) of 48,294 participants across 16 cohorts confirmed that low ABI independently predicts cardiovascular events beyond traditional Framingham risk factors — an ABI below 0.90 essentially reclassifies patients to a higher cardiovascular risk category equivalent to a prior MI or stroke for prevention purposes.
Toe-Brachial Index (TBI)
When ankle vessels are non-compressible (ABI >1.40), the toe-brachial index (TBI) provides an accurate hemodynamic assessment ( — Search PubMed). Digital arteries of the toes are rarely affected by medial calcification. TBI is measured with small pneumatic cuffs at the base of the first or second toe and photoplethysmography (PPG) to detect digital pulse waveforms. A TBI below 0.70 is diagnostic of hemodynamically significant PAD. A toe pressure below 30 mmHg is a key threshold for CLTI.
Post-Exercise ABI
Patients with equivocal resting ABI (borderline range) may have normal resting pressures that fall significantly after exercise-induced ischemia. Post-exercise ABI (measured immediately after a standardized treadmill test) can unmask hemodynamically significant PAD in symptomatic patients with otherwise normal resting values — a drop of >20 mmHg or >15% after exercise confirms the diagnosis.
7. Classification Systems
Two major classification systems are used clinically and in research to describe PAD severity: the Fontaine classification (older, widely used in Europe) and the Rutherford classification (more granular, preferred in North America and most contemporary clinical trials).
Rutherford Classification
The Rutherford system grades PAD from Category 0 to Category 6, combining subjective symptoms with objective hemodynamic findings from treadmill testing and segmental pressure measurements:
- Category 0: Asymptomatic. ABI normal at rest; normal treadmill performance.
- Category 1 (Mild claudication): Completes standard treadmill; ankle pressure after exercise >50 mmHg but at least 20 mmHg below brachial pressure.
- Category 2 (Moderate claudication): Between categories 1 and 3.
- Category 3 (Severe claudication): Cannot complete standard treadmill; ankle pressure after exercise <50 mmHg.
- Category 4 (Ischemic rest pain): Resting ankle pressure <40 mmHg; flat or barely pulsatile ankle or metatarsal pulse volume recording.
- Category 5 (Minor tissue loss): Resting ankle pressure <60 mmHg; non-healing ulcer or focal gangrene with diffuse pedal ischemia.
- Category 6 (Major tissue loss): Major tissue loss extending above the transmetatarsal level; functional foot no longer salvageable.
Fontaine Classification
- Stage I: Asymptomatic.
- Stage IIa: Mild claudication (walking distance >200 m).
- Stage IIb: Moderate to severe claudication (walking distance <200 m).
- Stage III: Ischemic rest pain.
- Stage IV: Ulceration or gangrene.
WIfI Classification for CLTI
The WIfI (Wound, Ischemia, foot Infection) classification, developed by the Society for Vascular Surgery, provides a more nuanced three-dimensional staging system specifically for CLTI that better predicts 1-year amputation risk and guides revascularization decision-making. It grades each dimension (Wound severity 0–3, Ischemia severity 0–3, Infection severity 0–3) independently, producing a composite clinical stage (1–4) that guides management intensity — from medical optimization alone in Stage 1 to urgent revascularization in Stage 4.
8. Diagnosis
The diagnostic workup for PAD serves three goals: confirming the diagnosis, assessing anatomical disease extent and severity for revascularization planning, and evaluating systemic cardiovascular disease burden. Guidelines recommend a stepwise approach beginning with non-invasive testing.
History and Physical Examination
A thorough vascular history documents the presence, location, onset, and progression of claudication symptoms; risk factors (tobacco use, diabetes duration and control, hypertension, dyslipidemia, prior cardiovascular events); and functional status (maximum walking distance, activity limitations). Physical examination includes:
- Pulse examination: palpation of femoral, popliteal, dorsalis pedis, and posterior tibial pulses bilaterally. Absent or diminished pulses indicate significant proximal disease. However, pulse examination is insensitive and operator-dependent — normal pulses do not exclude PAD.
- Bruit auscultation: femoral bruits at the groin suggest aortoiliac or proximal femoral stenosis. Their absence does not exclude disease.
- Skin and tissue assessment: skin temperature (cooler in ischemic limbs), hair loss on the dorsum of the foot and toes, thickened dystrophic nails, muscle wasting, skin atrophy, pallor on elevation, and dependent rubor (a sign of advanced ischemia — the foot turns deep red when dependent as maximally dilated arterioles fill from gravity).
ABI and Duplex Ultrasound
After ABI confirmation of PAD, duplex ultrasound provides detailed anatomical mapping of disease extent and severity without radiation or contrast exposure. Duplex combines B-mode imaging with Doppler velocity measurements: a focal velocity ratio >2.0 at a stenosis corresponds to >50% diameter reduction. Duplex is highly accurate for femoropopliteal disease and is frequently sufficient for endovascular intervention planning, though its resolution decreases in heavily calcified vessels and in evaluating the aortoiliac segment in obese patients.
CT Angiography (CTA)
CTA of the aorta and lower extremity arteries provides high-resolution three-dimensional anatomical mapping across the full aortoiliac-tibial circuit in a single study. It is the preferred pre-operative imaging modality for complex CLTI cases requiring bypass surgery planning. Limitations include iodinated contrast (nephrotoxic — relevant in the CKD patients who constitute a large fraction of CLTI), radiation exposure, and artifact from heavy calcification that obscures lumen assessment in tibial vessels.
Magnetic Resonance Angiography (MRA)
MRA — particularly contrast-enhanced MRA with gadolinium — provides excellent anatomical resolution without radiation and with superior soft-tissue contrast. It is preferred in patients with contrast allergy or CKD (where gadolinium is used at lower doses than iodinated contrast). Limitations include lower availability, longer acquisition times, and inability to image patients with certain metallic implants (pacemakers, some stents).
Digital Subtraction Angiography (DSA)
Invasive angiography remains the gold standard for pre-intervention anatomical assessment, particularly when percutaneous revascularization is planned in the same session ("diagnostic and therapeutic" procedure). It provides real-time visualization of flow, collateral circulation, and distal runoff, and allows immediate pressure-gradient measurements across stenoses. Its limitation is procedural risk (access site complications, contrast nephropathy, radiation) and cost, restricting its use to cases where revascularization is being planned.
Systemic Cardiovascular Assessment
Given the high prevalence of concurrent CAD and cerebrovascular disease in PAD patients, diagnostic evaluation should include ECG, echocardiography if cardiac symptoms are present, and assessment for carotid disease (duplex ultrasound of carotids in patients with PAD and bruit or neurological symptoms). Serum biomarkers — fasting lipid panel, HbA1c, renal function (creatinine, eGFR), CBC, and hsCRP — characterize the systemic vascular risk profile.
9. Medical Management
Medical management forms the foundation of PAD care for all patients, regardless of symptom severity. Its goals are to reduce systemic cardiovascular event risk (MI, stroke, vascular death — the dominant causes of mortality in PAD), prevent PAD progression to CLTI, and improve walking function. Medical therapy has evolved substantially, with the addition of low-dose rivaroxaban to aspirin (the COMPASS regimen) representing the most significant advance in PAD pharmacotherapy in two decades.
Antiplatelet Therapy
Single antiplatelet therapy with aspirin (75–100 mg/day) or clopidogrel (75 mg/day) is recommended for all symptomatic PAD patients to reduce MI and stroke risk (2016 AHA/ACC PAD guideline; Search PubMed). The EUCLID trial ( — Search PubMed) compared clopidogrel directly with ticagrelor in 13,885 PAD patients and found no significant difference in the composite of cardiovascular death, MI, or ischemic stroke. Clopidogrel remains the preferred single antiplatelet agent (non-inferior to ticagrelor, better tolerated, less bleeding).
The landmark COMPASS trial ( — Search PubMed) demonstrated that the combination of low-dose rivaroxaban 2.5 mg twice daily plus aspirin 100 mg daily reduced major adverse cardiovascular events (MACE) and major adverse limb events (MALE) significantly more than aspirin alone in PAD patients, at the cost of increased non-fatal bleeding. The 2024 updated guidelines now give Class IIa recommendation to the rivaroxaban-aspirin combination for symptomatic PAD patients at low bleeding risk — this "vascular dose" rivaroxaban is the most important pharmacological advance in PAD in recent years.
Statin Therapy
High-intensity statin therapy (atorvastatin 40–80 mg or rosuvastatin 20–40 mg) is indicated for all PAD patients to reduce cardiovascular events and slow PAD progression. Statins reduce atherosclerotic plaque progression, stabilize existing plaques, improve endothelial function, and reduce systemic inflammation. In PAD-specific analyses, statin therapy reduces the risk of MALE (amputation, bypass graft failure, revascularization) by 25–35% and all-cause mortality. LDL-C targets are aggressive: below 55 mg/dL in very-high-risk PAD patients (those with CLTI or concurrent CAD) per current ACC/AHA guidelines.
Blood Pressure Control
A blood pressure target of <130/80 mmHg is recommended in PAD patients. ACE inhibitors and ARBs are first-line for patients with PAD and diabetes or CKD. The concern that antihypertensives might reduce distal perfusion pressure has been largely refuted — multiple trials show no significant worsening of PAD symptoms with beta-blockers or ACE inhibitors in claudication, and the cardiovascular risk reduction benefit clearly outweighs any marginal hemodynamic concern. The one exception is patients with CLTI and severely compromised ankle pressures — in this group, excessive blood pressure lowering may precipitate critical ischemia.
Glycemic Management
For diabetic PAD patients, HbA1c target below 7.0% is the standard goal, with individualized targets (7.5–8.0%) in elderly or complex patients. Beyond glycemic control, the choice of glucose-lowering agent matters: SGLT2 inhibitors (empagliflozin, canagliflozin) and GLP-1 receptor agonists (liraglutide, semaglutide) reduce MACE independently of glucose lowering and are preferred in PAD patients with atherosclerotic cardiovascular disease. Some SGLT2 inhibitors have shown adverse signals for lower extremity amputation in high-risk PAD patients — canagliflozin in CANVAS — though subsequent data and meta-analyses have clarified this risk to be specific to already-severe PAD and largely offset by overall cardiovascular benefit.
Smoking Cessation
Smoking cessation is the single intervention with the greatest impact on PAD progression and limb salvage. Every clinical encounter should include structured cessation counseling. Pharmacological aids — varenicline (most effective), bupropion, and nicotine replacement therapy — are all appropriate. Even partial reduction in smoking improves PAD outcomes. Patients who quit have significantly better post-revascularization patency rates, fewer amputations, and better overall cardiovascular survival compared with those who continue to smoke.
Cilostazol for Claudication
Cilostazol (50–100 mg twice daily) is the only US FDA-approved pharmacological therapy specifically for claudication symptom relief. It is a phosphodiesterase-3 (PDE3) inhibitor that increases intracellular cAMP in platelets and vascular smooth muscle, producing vasodilation, antiplatelet effects, and reduced smooth muscle cell proliferation. A 2015 meta-analysis ( — Search PubMed) confirmed that cilostazol significantly increases maximum walking distance by approximately 40–50% and pain-free walking distance by approximately 67% compared with placebo. Cilostazol is contraindicated in heart failure of any severity — a critical prescribing caution, as PAD and HF co-occur frequently. Side effects include headache, diarrhea, and palpitations.
10. Supervised Exercise and Lifestyle
Supervised exercise therapy (SET) is the most effective treatment available for intermittent claudication — superior to cilostazol, comparable or superior to endovascular revascularization for walking distance improvement, and profoundly beneficial for systemic cardiovascular health. It is a Class I recommendation in all major PAD guidelines. Despite this evidence, SET remains dramatically underutilized, primarily because of lack of referral, insurance coverage gaps, and patient transportation barriers.
Mechanism of Benefit
SET improves claudication through multiple complementary mechanisms:
- Arteriogenesis: Repetitive ischemic stimulus drives collateral vessel remodeling through shear stress-mediated upregulation of VEGF, FGF, and monocyte chemoattractant protein-1 (MCP-1), enlarging native collateral channels and improving distal perfusion.
- Skeletal muscle adaptation: Exercise training improves oxidative enzyme capacity, mitochondrial density, and slow-twitch muscle fiber proportion, allowing the exercising muscle to extract more oxygen per unit of blood flow — effectively increasing the ischemic threshold.
- Hemorheological effects: Exercise reduces blood viscosity and fibrinogen levels, improving microcirculatory flow.
- Endothelial function: Regular aerobic exercise improves endothelial nitric oxide synthase (eNOS) activity and reduces oxidative stress, partially reversing endothelial dysfunction.
- Systemic cardiovascular conditioning: Aerobic fitness improvements reduce heart rate and blood pressure, improve insulin sensitivity, and reduce cardiovascular event risk.
Program Structure
Effective SET programs follow a structured treadmill protocol:
- Sessions 3 times per week for at least 12 weeks (most benefit accumulates by 24 weeks of consistent training).
- Each session: warm-up, then treadmill walking at a speed and grade that induces moderate claudication within 3–5 minutes.
- Walk-rest intervals: walk to moderate claudication (4–5 on a 1–10 pain scale), rest until pain resolves, repeat.
- Progressive overload: as claudication distance improves, speed and/or grade are increased to maintain the training stimulus.
- A Cochrane meta-analysis ( — Search PubMed) of 30 randomized trials confirmed that SET significantly improves maximal walking distance by a mean of 180 m and quality of life compared with usual care.
Home Exercise and Alternative Approaches
For patients unable to access supervised programs, structured home exercise programs with behavioral support (activity monitors, telehealth coaching) are a reasonable alternative, though outcomes are modestly inferior to supervised programs. Pole walking (Nordic walking) and cycling are alternative modalities for patients with severe claudication who cannot tolerate treadmill protocols. Upper body ergometry can provide cardiovascular conditioning for patients with severe bilateral disease or amputations.
Dietary Modification
A Mediterranean-pattern diet — rich in olive oil, vegetables, legumes, fish, and whole grains, low in red meat and processed foods — reduces atherosclerotic cardiovascular risk in PAD patients. Omega-3 fatty acids (EPA/DHA) reduce triglycerides and systemic inflammation. Sodium restriction (<2.3 g/day) supports blood pressure control. Weight reduction in obese patients reduces peripheral vascular resistance and insulin resistance, though very rapid weight loss should be avoided as it may worsen calf muscle wasting in claudicant patients.
11. Revascularization and Critical Limb Ischemia
Revascularization — restoring arterial blood flow — is indicated for patients with disabling claudication refractory to exercise therapy and medical management, and for all patients with CLTI (ischemic rest pain or tissue loss) in whom a revascularization target vessel and acceptable surgical/procedural risk exist. The choice between endovascular and surgical revascularization has been one of the central debates in vascular medicine, partially resolved by the BEST-CLI trial.
Endovascular Revascularization
Percutaneous transluminal angioplasty (PTA) with or without stenting is the first-line revascularization strategy for most anatomically suitable lesions. The procedural approach varies by lesion characteristics:
- Aortoiliac lesions (TASC A/B): Balloon-expandable stent placement is highly durable (5-year primary patency 70–80%) with minimal procedural risk. Now the preferred treatment even for total iliac occlusions in experienced centers.
- Femoropopliteal lesions: Drug-coated balloons (DCB) and drug-eluting stents (DES) incorporating paclitaxel or sirolimus have significantly improved patency over bare metal stents in the SFA. Long-segment total occlusions remain technically challenging with lower durability.
- Tibial lesions (CLTI): Angioplasty of tibial arteries for limb salvage — the "angiosome-directed" approach targets the specific tibial artery supplying the wound territory. Tibial intervention is technically demanding due to vessel size, calcification, and poor distal runoff.
Surgical Revascularization (Bypass Surgery)
Surgical bypass uses autologous vein (usually the great saphenous vein) or prosthetic graft (PTFE or Dacron) to reroute blood flow around an occluded arterial segment. Key bypass configurations include:
- Aortobifemoral bypass: Gold standard for aortoiliac occlusive disease; 10-year patency exceeds 80%. Requires major abdominal surgery with attendant cardiac and pulmonary risk.
- Femoropopliteal bypass: Above-knee with prosthetic graft (adequate for moderate-length occlusions) or below-knee with vein graft (superior patency, required for distal targets).
- Femorotibial (distal) bypass: Using reversed or in-situ saphenous vein to tibial or pedal arteries — the most demanding bypass, reserved for CLTI with no suitable proximal target.
BEST-CLI Trial: Endovascular vs. Surgical for CLTI
The landmark BEST-CLI (Best Endovascular vs. Best Surgical Therapy for CLTI) trial ( — Search PubMed) randomized 1,830 CLTI patients with suitable anatomy to endovascular-first versus surgical bypass-first strategy. Key findings: in patients with an adequate single-segment great saphenous vein available for bypass, surgical bypass produced superior outcomes (lower risk of major adverse limb events — MALE) compared with endovascular treatment. In patients without an adequate saphenous vein, endovascular and surgical strategies had comparable outcomes. These results suggest that CLTI patients with good vein conduit should be offered surgical bypass as the preferred revascularization strategy when surgically fit.
Global Vascular Guidelines for CLTI
The 2019 Global Vascular Guidelines ( — Search PubMed) provide a comprehensive framework for CLTI management, endorsing the WIfI classification for risk stratification and introducing the concept of limb staging to guide revascularization intensity. They emphasize that wound care, infection control, and nutritional optimization must accompany revascularization — isolated revascularization without multidisciplinary wound management yields inferior outcomes.
Amputation
When revascularization is not feasible (no suitable target vessels, prohibitive surgical risk) or has failed, major amputation — below-knee (transtibial) or above-knee (transfemoral) — may become necessary to control infection, remove non-viable tissue, and relieve uncontrollable pain. The level of amputation is guided by blood flow (transcutaneous oxygen pressure measurements), skin viability, and rehabilitation potential. Transtibial amputation preserves the knee joint and significantly improves prosthetic rehabilitation potential and long-term mobility compared with transfemoral amputation. A comprehensive multidisciplinary approach — vascular surgery, orthopedics, physical therapy, prosthetics, and pain management — is essential to maximize quality of life after amputation.
12. Research Papers
- Gerhard-Herman MD et al. 2016 AHA/ACC Guideline on the Management of Patients With Lower Extremity Peripheral Artery Disease. J Am Coll Cardiol. 2017. — Search PubMed
- Hiatt WR et al. Ticagrelor versus Clopidogrel in Symptomatic Peripheral Artery Disease (EUCLID Trial). N Engl J Med. 2017. — Search PubMed
- Anand SS et al. Rivaroxaban with or without Aspirin in Patients with Stable Peripheral or Carotid Artery Disease (COMPASS). N Engl J Med. 2018. — Search PubMed
- Fowkes FGR et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010. Lancet. 2013. — Search PubMed
- Ankle Brachial Index Collaboration. Ankle brachial index combined with Framingham Risk Score to predict cardiovascular events and mortality. JAMA. 2008. — Search PubMed
- Lane R et al. Exercise for intermittent claudication. Cochrane Database Syst Rev. 2014. — Search PubMed
- Stevens JW et al. Cilostazol for peripheral arterial disease (claudication): a meta-analysis. Int J Clin Pract. 2015. — Search PubMed
- Farber A et al. Surgery or Endovascular Therapy for Chronic Limb-Threatening Ischemia (BEST-CLI Trial). N Engl J Med. 2022. — Search PubMed
- Conte MS et al. Global Vascular Guidelines on the Management of Chronic Limb-Threatening Ischemia. J Vasc Surg. 2019. — Search PubMed
- Vogelberg KH et al. The significance of smoking as a risk factor for peripheral arterial occlusive disease. Dtsch Med Wochenschr. 1996. — Search PubMed
- Jude EB et al. Peripheral arterial disease in diabetic and nondiabetic patients: a comparison of severity and outcome. Diabetes Care. 2001. — Search PubMed
- Williams DT et al. The use of the toe brachial index in the assessment of peripheral vascular disease in people with diabetes. J Vasc Surg. 2005. — Search PubMed
13. Connections
- Nitric Oxide & Vessel Dilation — interactive animation
- Atherosclerosis
- Coronary Artery Disease
- Aortic Aneurysm
- Carotid Artery Stenosis
- Hypertension
- Diabetes Mellitus
- Peripheral Neuropathy
- Deep Vein Thrombosis