PQQ for Sleep, Mood & Mental Fatigue
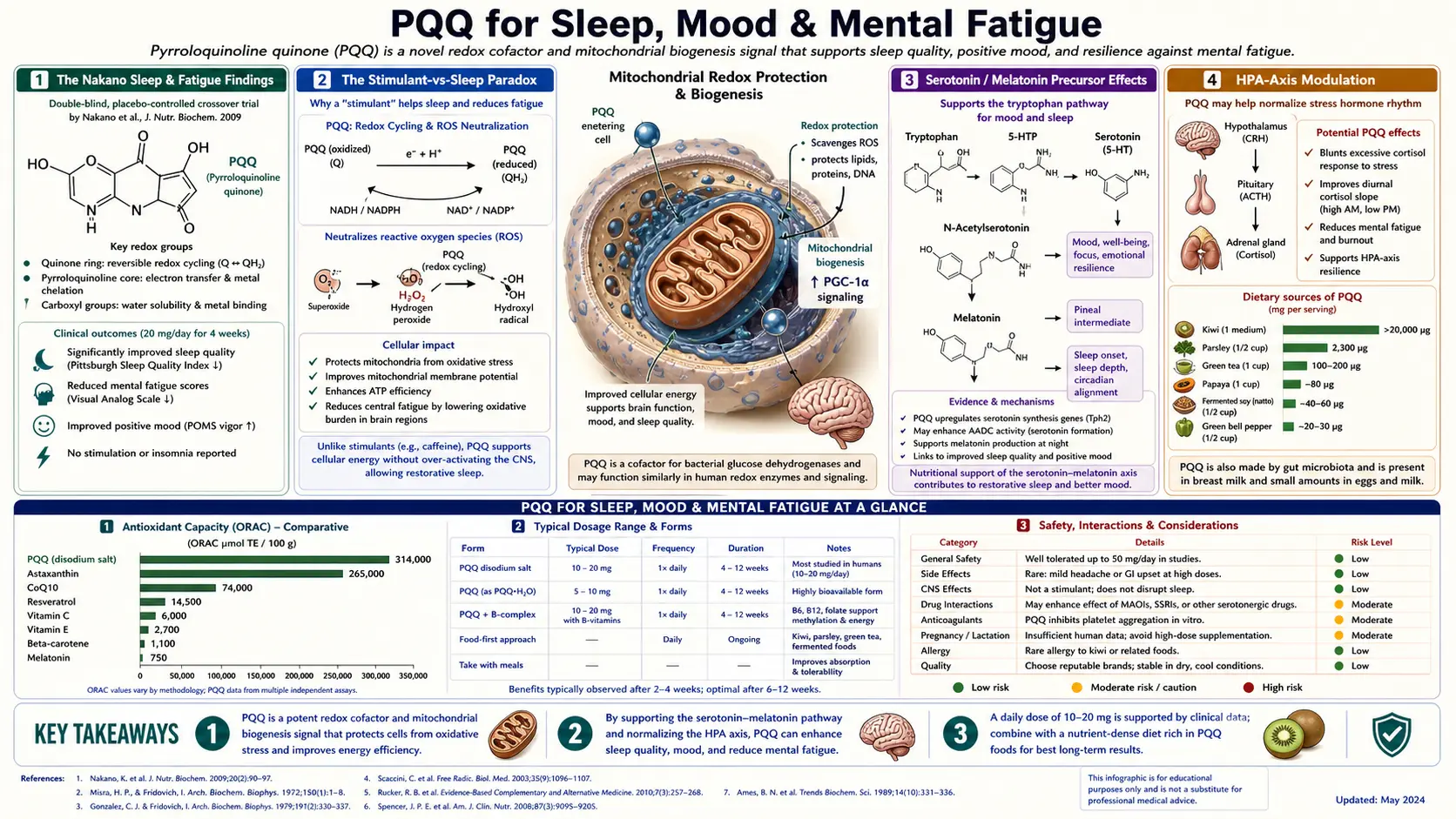
The Nakano 2009 trial reported significant reductions in sleep-onset latency and subjective mental fatigue after 8-24 weeks of 20 mg/day PQQ — a counterintuitive pair of findings given that PQQ also has a mild stimulant effect in the morning. The resolution is that PQQ's long-term mitochondrial-restoration effect in hypothalamic and brainstem nuclei normalizes circadian function, while its acute biogenesis signaling produces transient morning alertness. The clinical implication is morning-only dosing for sleep protection, paired with magnesium glycinate at night, and a particular role in chronic fatigue, brain fog, and post-viral fatigue syndromes where mitochondrial dysfunction is documented.
Table of Contents
- The Nakano Sleep & Fatigue Findings
- The Stimulant-vs-Sleep Paradox
- Serotonin / Melatonin Precursor Effects
- HPA-Axis Modulation
- Morning-vs-Evening Dosing Rationale
- Pairing With Magnesium Glycinate
- Use in Chronic Fatigue & Brain Fog
- Post-Viral Fatigue Syndromes
- Mental Fatigue & Work Productivity
- Practical Protocol
- Cautions
- Key Research Papers
- Connections
- Featured Videos
The Nakano Sleep & Fatigue Findings
The most concrete sleep and fatigue data on PQQ come from the Nakano 2009 trial, which followed 71 Japanese adults on 20 mg/day BioPQQ for 24 weeks. The trial's primary cognitive endpoints are covered in the Cognition deep-dive; the secondary sleep and fatigue endpoints are the focus here.
Key sleep findings:
- Sleep-onset latency reduction — subjects fell asleep faster on PQQ vs. placebo at the 12-week and 24-week timepoints. The effect was modest in absolute terms but statistically significant.
- Subjective sleep quality improvement — subjects reported feeling more rested on waking, with reduced sleep disturbance during the night.
- Reduced daytime drowsiness — consistent with improved sleep architecture or improved daytime energy capacity, both plausible mechanisms.
Key fatigue findings:
- Reduced subjective mental fatigue — on standardized fatigue measures, the PQQ group showed significant improvement
- Improved stress tolerance — subjects reported feeling less worn down by daily stressors
- Improvements emerged gradually — not visible at 4 weeks, partially visible at 8 weeks, fully visible at 12-24 weeks
These findings have not been independently replicated as cleanly as the cognitive endpoints, but they are consistent with the broader pattern of "improved cellular energy state" effects across the PQQ literature. The Hwang 2018 trial documented reduced d-ROMs (oxidative stress marker), which is mechanistically related to both reduced mental fatigue and improved sleep quality.
The Stimulant-vs-Sleep Paradox
A puzzle in the PQQ literature: many users report a mild stimulant or alertness-enhancing effect within hours of taking PQQ, particularly during the first 1-2 weeks of use. Yet the long-term trials (Nakano in particular) document improved sleep quality and reduced sleep-onset latency. How can both be true?
The resolution involves two separate timescales of PQQ action:
- Acute effect (hours to days): CREB phosphorylation begins within hours of PQQ exposure. The downstream PGC-1α cascade and mitochondrial assembly take days to weeks, but the acute signaling itself appears to produce a transient alertness effect, possibly through cAMP-mediated effects on locus coeruleus or hypothalamic arousal nuclei. This is the "mild stimulant" some users notice.
- Chronic effect (weeks to months): As new mitochondria are assembled in cells throughout the brain, including hypothalamic and brainstem nuclei that regulate sleep-wake cycles, overall energy capacity normalizes. Better daytime energy translates into better daytime function (less napping, more activity, more time outside), which itself improves sleep at night. Improved mitochondrial function in the suprachiasmatic nucleus and pineal gland plausibly improves circadian rhythm regulation. The net effect is improved sleep, despite the acute mild stimulant character.
The practical consequence is timing-dependent: morning PQQ allows the acute stimulant effect to dissipate before bedtime, while still delivering the long-term mitochondrial benefit to sleep-regulating circuits. Evening PQQ traps the acute stimulant effect in the sleep-onset window, defeating the long-term sleep-quality benefit.
This is the same logic that applies to acute vs. chronic caffeine effects, with one important difference: caffeine has an entirely acute mechanism (adenosine receptor antagonism) and does not produce long-term benefits to sleep architecture. PQQ has both acute and chronic mechanisms, and the chronic effect is the more clinically valuable one.
Serotonin / Melatonin Precursor Effects
One proposed mechanism for PQQ's sleep effect involves the serotonin / melatonin precursor pathway. The biology runs:
Dietary tryptophan → 5-hydroxytryptophan (5-HTP) → serotonin (5-HT) → N-acetylserotonin → melatonin.
Each step requires specific enzymes and cofactors. The conversion of tryptophan to 5-HTP requires tryptophan hydroxylase, a tetrahydrobiopterin-dependent enzyme. The conversion of serotonin to N-acetylserotonin requires acetyl-CoA. Melatonin synthesis is most active during darkness in the pineal gland.
PQQ's relevance to this pathway is largely indirect, through three mechanisms:
- Improved cellular energy state — ATP and acetyl-CoA availability supports the energy-dependent steps in serotonin and melatonin synthesis. Cells with more mitochondria have more substrate availability for these biosynthetic pathways.
- Reduced oxidative stress in the pineal gland — oxidative stress impairs melatonin synthesis. PQQ's antioxidant effects in pineal tissue plausibly support melatonin production.
- Improved tetrahydrobiopterin (BH4) regeneration — BH4 is the cofactor for tryptophan hydroxylase and is regenerated via NADPH-dependent reactions. Improved mitochondrial NADPH capacity (an indirect consequence of biogenesis) supports BH4 availability.
None of these mechanisms have been directly demonstrated in human PQQ trials. They are mechanistic plausibility arguments based on the broader biology of serotonin/melatonin synthesis. The direct trial evidence (Nakano) shows the clinical phenotype — better sleep, reduced fatigue — without specifying the molecular pathway.
The practical interpretation: if a user wants to specifically target the serotonin/melatonin pathway for sleep, dedicated interventions (5-HTP, melatonin itself, light exposure protocols) are more direct. PQQ supports the pathway indirectly through general cellular-energy improvement, which is real but diffuse.
HPA-Axis Modulation
The hypothalamic-pituitary-adrenal (HPA) axis regulates cortisol secretion in a diurnal pattern: high in the morning (driving wakefulness), declining through the day, lowest in the early night (allowing melatonin to rise). HPA dysregulation — flattened diurnal curve, elevated evening cortisol, blunted morning cortisol — is a common feature of chronic fatigue, depression, post-traumatic stress, and aging.
PQQ's effects on HPA axis function in humans are inferred indirectly. The Nakano trial reported improved stress tolerance and reduced subjective mental fatigue, which are clinical phenotypes consistent with improved HPA function. Direct measurement of cortisol curves in PQQ trials has not been published.
Mechanistic possibilities:
- Mitochondrial dysfunction in hypothalamic and pituitary cells contributes to HPA dysregulation; biogenesis-driven mitochondrial restoration in these cells plausibly normalizes function
- Adrenal cortex cells are exceptionally mitochondria-dense (steroid hormone synthesis is energy-intensive); supporting adrenal mitochondrial function may support cortisol response capacity
- Reduced oxidative stress reduces HPA tonic activation — chronic oxidative stress is itself a stressor that drives HPA upregulation
The clinical interpretation: PQQ is unlikely to be a dramatic HPA-axis intervention by itself, but it may be a useful supportive component of broader HPA-recovery protocols that also include sleep optimization, stress reduction, adaptogenic herbs (rhodiola, ashwagandha), and adrenal-supportive nutrients (vitamin C, B5, magnesium).
See Adrenal Fatigue for the broader HPA-dysfunction syndrome and integrative interventions.
Morning-vs-Evening Dosing Rationale
The morning-only PQQ dosing convention is one of the most consistent recommendations across the supplement and functional-medicine literature, and rests on three converging lines of evidence:
- The acute stimulant effect: users consistently report mild alertness within 1-3 hours of PQQ ingestion. Evening dosing pushes this alertness window into the bedtime period.
- Clinical trial design: all the major positive PQQ trials (Itoh, Nakano, Hwang) used morning dosing. Sleep-quality improvements are documented at that timing.
- Pharmacokinetics: plasma half-life of PQQ is approximately 1-3 hours. Morning dosing means plasma levels are minimal by evening, while cellular effects (biogenesis signaling) persist throughout the day and night because the downstream gene-expression effects long outlast the plasma concentration.
The recommendation: take PQQ with or shortly after breakfast. If splitting the dose (e.g., 20 mg morning + 20 mg midday for high-dose protocols), the second dose should be no later than early afternoon (1-2 PM).
For users who experience PQQ-related sleep disruption despite morning dosing, options include:
- Reduce the dose (10 mg may be sufficient for some users)
- Take with food rather than fasting (slower absorption, less peak stimulation)
- Discontinue for 1-2 weeks and restart at lower dose to assess tolerance
- Pair with evening magnesium glycinate (see next section)
Pairing With Magnesium Glycinate
The most rational evening complement to morning PQQ is magnesium glycinate. The combination addresses different parts of the sleep-energy-mitochondria axis:
- Morning PQQ — drives mitochondrial biogenesis, supports daytime energy and cognitive performance, has acute mild stimulant effect
- Evening magnesium glycinate — supports GABAergic neurotransmission, reduces neuromuscular excitability, improves sleep architecture (particularly slow-wave sleep), supports parasympathetic tone
Magnesium is also a cofactor for ATP — every molecule of ATP in the body is functionally bound to magnesium — so magnesium adequacy supports the cellular energy capacity that PQQ creates. The two interventions are mechanistically complementary rather than overlapping.
Typical protocol:
- Morning: PQQ 20 mg + ubiquinol 100-200 mg with breakfast
- Evening (1-2 hours before bed): Magnesium glycinate 300-400 mg of elemental magnesium
- Optional addition: L-theanine 200-400 mg evening if sleep onset is the primary issue
For broader sleep optimization, see the magnesium and sleep article. Magnesium glycinate is preferred over magnesium oxide (poor absorption), magnesium citrate (can be laxative at sleep-relevant doses), and magnesium L-threonate (more expensive, with marginal evidence for the cognitive-specific benefit it's marketed for).
Use in Chronic Fatigue & Brain Fog
Chronic fatigue and brain fog are clinical syndromes with multiple possible causes (thyroid, anemia, sleep apnea, depression, post-viral, autoimmune). When mitochondrial dysfunction is part of the etiology — which is increasingly recognized in chronic fatigue syndrome, fibromyalgia, long-COVID, and post-EBV reactivation — PQQ is a reasonable component of broader mitochondrial-supportive protocols.
The clinical reality is that PQQ as monotherapy in established chronic fatigue syndromes produces modest effects. The mitochondrial dysfunction in ME/CFS is severe, multi-factorial, and partially refractory to single-nutrient interventions. PQQ is best used as one element of a layered approach:
- Mitochondrial nutrient stack: PQQ 20 mg + ubiquinol 200-400 mg + alpha lipoic acid 600 mg + acetyl-L-carnitine 1000-2000 mg + creatine 3-5 g + B-complex including methylated B12 + magnesium glycinate
- Address contributing factors: sleep optimization, treat dysautonomia if present, identify and address triggers (food sensitivities, toxin exposures, ongoing infections)
- Pacing and graded activity: for ME/CFS specifically, post-exertional malaise is the cardinal feature; aggressive exercise prescriptions worsen the condition. Pacing strategies are essential.
- Specialist input: functional medicine, integrative medicine, or specialized ME/CFS clinics if the syndrome is severe or refractory
For brain fog in milder presentations (post-illness recovery, stress-driven, post-anesthesia, perimenopause-associated), PQQ + CoQ10 often produces noticeable improvement over 4-8 weeks. The cognitive deep-dive provides more detail on the brain-fog application.
Post-Viral Fatigue Syndromes
Post-viral fatigue is increasingly recognized as a distinct clinical entity since the COVID-19 pandemic. Long-COVID, post-EBV reactivation, post-Lyme syndrome, and other post-infectious fatigue presentations share features with classic ME/CFS, including documented mitochondrial dysfunction in research populations.
Mechanistic features:
- Reduced mitochondrial membrane potential in peripheral blood cells
- Reduced PGC-1α expression in skeletal muscle biopsies
- Increased oxidative stress markers (8-OHdG, MDA, isoprostanes)
- Reduced exercise capacity with cardiopulmonary exercise testing showing abnormal patterns
The PGC-1α reduction is mechanistically interesting because PQQ directly targets that pathway. Whether PQQ supplementation reverses the PGC-1α deficit in post-viral fatigue patients has not been formally tested in randomized trials, but it is the most theoretically targeted intervention currently available for that specific abnormality.
Clinical use in post-viral fatigue typically combines PQQ with the broader mitochondrial stack listed above. Users frequently report subjective improvement in mental clarity and reduced post-exertional fatigue over 8-12 weeks, though the effect size is variable and not all users respond.
For long-COVID specifically, the Methylene Blue and Long-COVID article covers a related mitochondrial-rescue approach that some clinicians combine with PQQ in advanced cases.
Mental Fatigue & Work Productivity
Mental fatigue — the felt experience of cognitive effort becoming progressively harder over the working day — is a distinct clinical and research domain from sleep-related fatigue. It is driven by glutamate accumulation in prefrontal cortex, declining catecholamine availability, glucose depletion in cortical regions during sustained cognitive work, and (in the mitochondrial-dysfunction-related cases) declining ATP availability at synaptic terminals.
PQQ's rationale for mental fatigue is the synaptic-energy support mechanism. With more mitochondria available at cortical synapses, sustained cognitive work depletes ATP reserves more slowly. The clinical phenotype is "the afternoon doesn't feel as foggy as it used to" or "I can sustain focus through longer meetings."
The Nakano trial documented subjective mental-fatigue improvement, and many users report this as the most noticeable PQQ effect even when cognitive tests show modest formal change. The phenomenology — "I have more left at the end of the day" — is hard to capture on standardized cognitive instruments designed for younger populations or for tracking neurodegenerative decline.
For users whose primary complaint is mental fatigue during sustained cognitive work (knowledge workers, students, mid-career professionals):
- PQQ 20 mg morning + ubiquinol 100-200 mg morning
- Consider adding creatine 3-5 g daily — trial evidence supports creatine for cognitive performance during sustained effort, complementing PQQ's biogenesis mechanism with ATP buffering
- Address sleep, exercise, and dietary basics before adding more supplements
- Expect 4-8 weeks for the effect to emerge; track subjective afternoon energy as the primary outcome
Practical Protocol
Standard sleep-and-fatigue-focused protocol
- Morning: PQQ 20 mg + ubiquinol 100-200 mg with breakfast
- Evening (1-2 hours before bed): Magnesium glycinate 300-400 mg elemental magnesium
- Duration: 12-week assessment window
Stronger protocol for chronic fatigue or post-viral fatigue
- Morning: PQQ 20-40 mg + ubiquinol 200-400 mg + acetyl-L-carnitine 1000 mg + B-complex with methyl-B12
- Midday (no later than 2 PM if splitting PQQ): Alpha lipoic acid 300-600 mg + creatine 3-5 g
- Evening: Magnesium glycinate 400 mg + optional L-theanine 200-400 mg
- Duration: 8-12 weeks for initial response; reassess and adjust
What to track
- Sleep-onset latency (time from lights-out to sleep onset) — many phone/watch apps track this
- Morning energy / refreshedness on waking (0-10 subjective scale)
- Afternoon mental energy / fatigue (0-10 subjective scale at 3 PM)
- Number of high-fatigue days per week
Timeline expectations
- Week 1-2: Possible mild morning alertness; sleep typically unchanged
- Week 3-4: Possible subtle improvement in afternoon mental energy
- Week 8: Sleep-onset latency improvement often noticeable
- Week 12: Full effect of the protocol typically apparent; matches trial assessment timing
- Month 6: Sustained maintenance; benefits typically persist as long as dosing continues
Cautions
- Strict morning dosing — evening PQQ can defeat the long-term sleep-quality benefit by trapping the acute mild stimulant effect in the bedtime window
- Sleep disorders need primary evaluation — if sleep problems are severe, evaluate for sleep apnea, restless legs, and primary insomnia before assuming a mitochondrial-supplement intervention will be sufficient
- Depression and mood disorders need primary treatment — PQQ is not a substitute for evidence-based depression treatment. Combination with antidepressants is safe but the antidepressant carries the primary therapeutic load.
- ME/CFS pacing is essential — PQQ supplementation does not justify pushing through post-exertional malaise. Pacing strategies remain the cornerstone of ME/CFS management.
- Iron, B12, folate, thyroid first — if fatigue is the primary complaint, basic lab workup (CBC, ferritin, B12, folate, TSH, free T4, free T3) should precede or accompany supplement interventions. Treating iron deficiency or hypothyroidism produces larger effect than any mitochondrial supplement.
- Pregnancy — lack of formal safety data for supplemental PQQ in pregnancy; avoid in absence of clinical guidance
- Stimulant interactions — if combining with caffeine or other stimulants, the additive alertness may be more than desired. Adjust dosing accordingly.
Key Research Papers
- Nakano M et al. (2009). Effects of oral supplementation with pyrroloquinoline quinone on stress, fatigue, and sleep. Food Style 21. — PubMed: Nakano 2009
- Itoh Y et al. (2016). PQQ disodium salt and cognitive functions (includes subjective fatigue endpoints). — PubMed: Itoh 2016 fatigue
- Hwang PS et al. (2018). PQQ supplementation and oxidative stress reduction (d-ROMs) in older adults. — PubMed: Hwang 2018 d-ROMs
- Harris CB et al. (2013). Dietary PQQ and inflammation / mitochondrial biomarkers in humans. J Nutr Biochem. — PubMed: Harris 2013
- Mitochondrial dysfunction in chronic fatigue syndrome — PubMed: ME/CFS + mitochondrial dysfunction
- Mitochondrial dysfunction in long-COVID — PubMed: long-COVID + mitochondrial dysfunction
- Mitochondrial dysfunction in fibromyalgia — PubMed: fibromyalgia + mitochondrial dysfunction
- Magnesium glycinate and sleep architecture — PubMed: magnesium glycinate + sleep
- Tryptophan, serotonin, melatonin pathway and sleep — PubMed: tryptophan / serotonin / melatonin / sleep
- HPA axis dysregulation in chronic fatigue and depression — PubMed: HPA dysregulation
- Creatine for cognitive performance under sustained effort — PubMed: creatine + cognitive performance
- Suprachiasmatic nucleus mitochondria and circadian rhythm — PubMed: SCN + mitochondria + circadian
PubMed Topic Searches
- PubMed: PQQ sleep / fatigue
- PubMed: PQQ mental fatigue / stress
- PubMed: mitochondrial dysfunction + brain fog
- PubMed: PQQ + post-viral fatigue
- PubMed: pineal mitochondria + melatonin
Connections
- PQQ Overview
- PQQ Benefits Hub
- PQQ for Mitochondrial Biogenesis
- PQQ for Cognition
- PQQ for NGF Synthesis
- CoQ10 (pairing)
- ALA for Mitochondria
- Methylene Blue & Long-COVID
- All Antioxidants
- Magnesium & Sleep
- Magnesium
- Creatine
- Vitamin B12
- Fatigue
- Brain Fog
- Chronic Fatigue Syndrome
- Fibromyalgia
- Adrenal Fatigue
- Post-Viral Triggers (EBV)
- Sleep Hygiene
- Longevity Protocols