Tyrosine for Cold Tolerance
Cold exposure is a uniquely catecholamine-demanding stressor. The autonomic nervous system mounts a sympathetic surge to drive vasoconstriction (preserving core temperature) and shivering thermogenesis (generating heat from skeletal muscle ATP hydrolysis), while the brain simultaneously must maintain vigilance and decision-making for survival behavior. Both axes draw heavily on norepinephrine and epinephrine, and after several hours both deplete catecholamine pools faster than synthesis can replace them. Tyrosine supplementation prevents this depletion, sustaining both cardiovascular cold response and cognitive performance — the mechanism behind the Banderet 1989 USARIEM trial, the Shurtleff 1994 cold-only trial, the Mahoney 2007 working-memory study, and the OBrien 2007 cooling protocols. This page is the operational deep-dive on the cold use case, including the Special Forces and polar-research protocols, the cold-plus-hypoxia-plus-sleep-loss combined stressors, and the limitations.
Interactive Visualization Dopamine, Reward & How Habits Hijack You Dopamine is not the pleasure chemical. Watch the spike migrate from the reward to the cue — then withhold the reward and see it dip below zero. That dip is craving. Launch →
Table of Contents
- The Physiology of Cold Exposure
- Catecholamine Demand During Cold Exposure
- Shivering and Non-Shivering Thermogenesis
- Cognitive Failure Under Cold — The Performance Cliff
- Shurtleff 1994 — Cold-Only Working Memory Trial
- Mahoney 2007 — Repeat Cold + Working Memory
- O'Brien 2007 — Body Cooling Protocols
- The Combined Stressors — Cold + Altitude + Sleep Loss
- The Special Forces Cold Protocol
- Cold-Water Diving and Immersion Applications
- Polar Research and Extreme Cold Expeditions
- What Tyrosine Will Not Do for Cold (Limits)
- Practical Protocol Summary
- Key Research Papers
- Connections
- Featured Videos
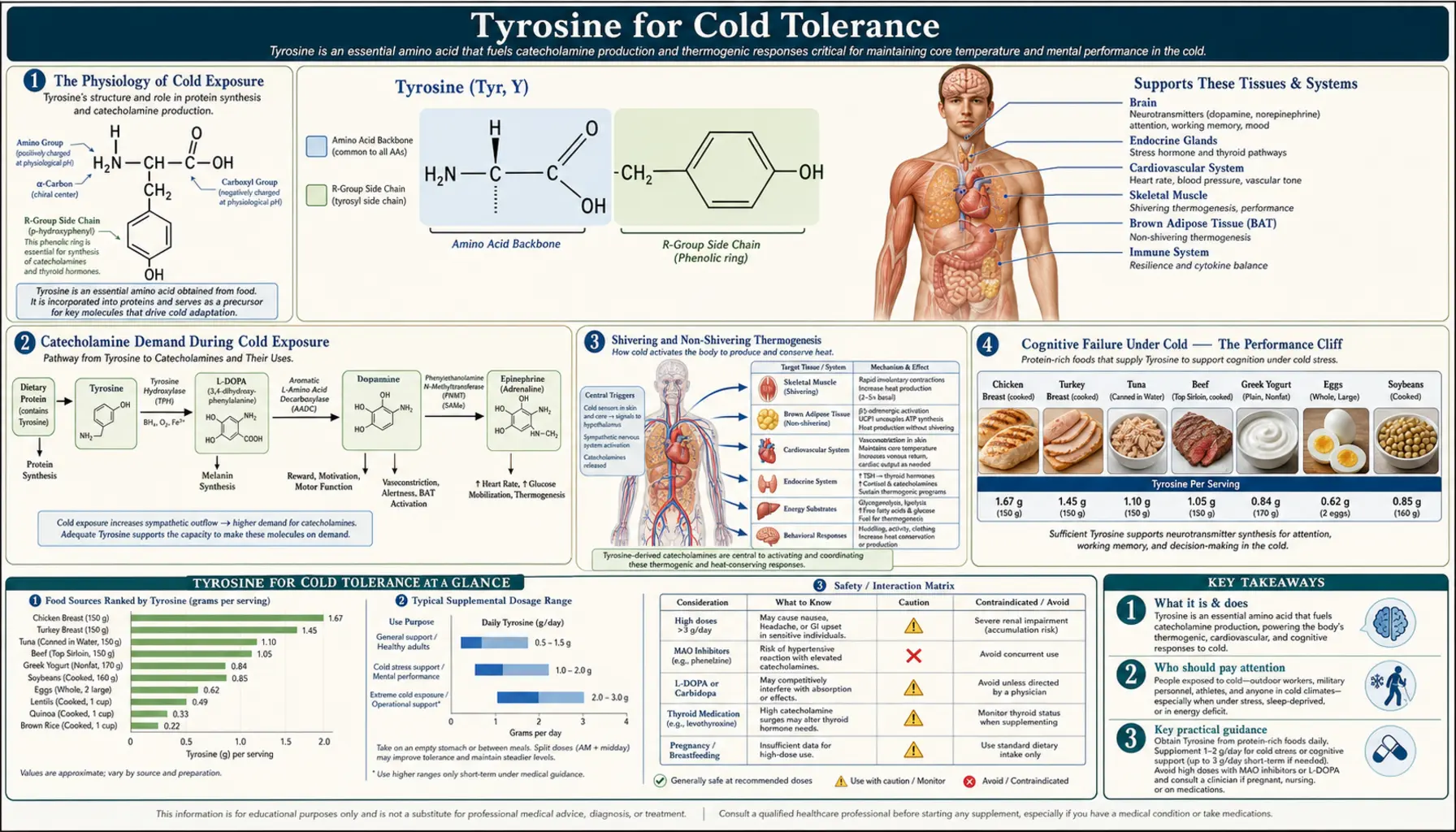
The Physiology of Cold Exposure
The human thermoregulatory response to cold is layered, with each layer engaging at a progressively lower body temperature or a longer exposure duration:
- Behavioral thermoregulation — first line. Add clothing layers, seek shelter, increase activity, drink hot fluids. Conscious and most effective. Failure here leads to engagement of the autonomic responses.
- Cutaneous vasoconstriction — sympathetic norepinephrine release at peripheral cutaneous arterioles produces alpha-1 adrenergic vasoconstriction, shunting blood from skin and extremities to the core. Preserves core temperature at the cost of cold hands and feet. Begins within seconds of cold exposure; sustained throughout exposure.
- Increased muscle tone (pre-shivering) — baseline muscle tension increases, generating modest heat without overt shivering. Mediated by sympathetic outflow and local muscle reflexes.
- Shivering thermogenesis — rhythmic synchronized contraction of antagonist muscle pairs, producing no net work but releasing the energy of ATP hydrolysis as heat. Engages at modest cold stress. Can increase metabolic rate 4–6 fold above basal but is metabolically expensive, fatiguing, and impairs fine motor function.
- Non-shivering thermogenesis — norepinephrine activates brown adipose tissue (more abundant in infants and cold-acclimated adults) and skeletal muscle uncoupling protein 3, producing heat without contraction. Mediates the metabolic adaptation to chronic cold exposure.
- Endocrine acclimation — chronic cold exposure increases thyroid hormone output (slightly), increases sympathetic tone, and increases brown adipose tissue depots. Develops over weeks of repeated exposure.
Every step from vasoconstriction onward depends on sympathetic catecholamine release. The colder the exposure and the longer it lasts, the larger the catecholamine demand. This is the substrate-availability problem that tyrosine addresses.
Catecholamine Demand During Cold Exposure
Acute cold exposure produces measurable spikes in plasma norepinephrine (3–5-fold above basal) and epinephrine (2–3-fold above basal) within the first 10–30 minutes. Both elevations sustain throughout the exposure. The synthesis of new catecholamines must keep pace with the accelerated release, or the catecholamine pools will deplete.
Three principal sites of catecholamine demand under cold:
- Adrenal medulla — secretes epinephrine and norepinephrine into the circulation in response to cold. Drives non-shivering thermogenesis via brown adipose tissue and supports cardiovascular response (increased cardiac output, vasoconstriction).
- Sympathetic postganglionic neurons — release norepinephrine onto cutaneous vasoconstrictors (alpha-1 mediated), onto cardiac muscle (beta-1 mediated, increasing heart rate and contractility), onto bronchial smooth muscle (beta-2, mild bronchodilation), and onto thermogenic tissues.
- Locus coeruleus (brainstem norepinephrine nucleus) — the principal source of brain norepinephrine. Activation during cold supports cortical arousal, attention, vigilance, and decision-making for cold-environment behavior. Without sustained LC activity, cognitive performance collapses.
The catecholamine pool of each of these sites is finite. The intracellular pool of dopamine, norepinephrine, and epinephrine is on the order of micrograms to milligrams per gram of tissue, with the largest depot in the adrenal medulla and the brain depots smaller. Sustained accelerated release without proportional synthesis depletes the pool over a timeframe of hours, depending on the intensity of the stressor.
This is what tyrosine pre-loading addresses. By providing the rate-limiting substrate for tyrosine hydroxylase across the elevated synthesis demand, tyrosine sustains the catecholamine pool, preserves both cardiovascular cold response and cognitive function, and delays the performance failure that occurs when stores are exhausted.
Shivering and Non-Shivering Thermogenesis
Shivering thermogenesis is the brute-force response. Antagonist muscle pairs contract rhythmically at 8–12 Hz, producing no net work but releasing the heat of ATP hydrolysis. Metabolic rate can increase 4–6 fold above basal (from approximately 70 W to 300–420 W) during peak shivering. The catecholamine demand here is sympathetic activation of muscle perfusion, glucose mobilization, and lipolysis to fuel the contraction. Shivering is fatiguing and impairs fine motor control (a shivering soldier cannot accurately fire a rifle, a shivering surgeon cannot operate, a shivering diver cannot manage complex gear).
Non-shivering thermogenesis (NST) is the elegant alternative. Norepinephrine at beta-3 adrenergic receptors on brown adipose tissue activates uncoupling protein 1 (UCP1), which short-circuits the mitochondrial proton gradient and dissipates the energy as heat without ATP production. Skeletal muscle also has a smaller contribution via UCP3. NST is metabolically more efficient than shivering, does not fatigue the same way, and does not impair motor function. Critical for infant thermoregulation; less abundant but still present in adults, with brown adipose tissue depots concentrated in supraclavicular, cervical, paraspinal, and perirenal locations.
Chronic cold exposure increases NST capacity. Cold-acclimated individuals (Inuit, Scandinavian fishermen, regular cold-plunge enthusiasts) have larger brown adipose depots, more responsive UCP1 expression, and rely more on NST and less on shivering for a given cold stress. This is the physiological basis for the modern interest in cold exposure (Wim Hof method, cold plunges, cryotherapy) as a metabolic-conditioning practice.
The tyrosine connection: both shivering and non-shivering thermogenesis depend on sympathetic catecholamine output. Tyrosine substrate support sustains both. For acute cold exposure of moderate to severe intensity (cold-water immersion, multi-hour cold-environment operations), tyrosine pre-loading delays the cumulative catecholamine depletion and helps maintain both heat-generation capacity and cognitive function for the duration of the exposure.
Cognitive Failure Under Cold — The Performance Cliff
One of the most consistently demonstrated findings in environmental physiology is that cognitive performance degrades nonlinearly with cold exposure. Mild cold (single-digit Celsius for under an hour with appropriate clothing) produces minimal cognitive impairment. Moderate cold (cold-clothed but with prolonged exposure of 2–4 hours) produces measurable degradation. Severe cold (insufficient clothing, multi-hour exposure, peripheral cold injury developing) produces dramatic performance failure that can be life-threatening — the hypothermic patient cannot make adaptive decisions, cannot navigate to safety, cannot self-extract.
The cognitive domains affected:
- Working memory — capacity to hold and manipulate information over seconds to minutes. Degrades early and substantially under cold.
- Vigilance and sustained attention — capacity to maintain alertness across a monotonous task. Highly susceptible to the combined cold-plus-sleep-loss profile of military and search-and-rescue operations.
- Reaction time — slows progressively with peripheral cold (slower nerve conduction in cold extremities contributes mechanically), with central cold (reduced central processing speed), and with sustained exposure (catecholamine depletion).
- Spatial navigation and map reading — complex visuospatial tasks degrade substantially. Soldiers in cold environments perform map-and-compass tasks significantly worse than warm-equivalent controls.
- Decision-making and judgment — the most consequential. Hypothermic individuals make poor decisions about clothing, shelter, and route, sometimes including the paradoxical undressing observed in severe hypothermia (an irrational behavior that accelerates death from exposure).
- Mood and motivation — irritability, depressed mood, and reduced effort under sustained cold exposure. Affects team cohesion and morale during multi-day operations.
Tyrosine supplementation in the operational cold trials consistently mitigates these cognitive impairments. Effect sizes are larger when baseline degradation is larger — the soldiers who suffer most under placebo benefit most from tyrosine. Effect sizes are smaller in milder cold exposures where degradation is also smaller.
Shurtleff 1994 — Cold-Only Working Memory Trial
The Shurtleff 1994 study isolated the cold-exposure variable from the hypoxia and sleep-deprivation confounds present in earlier trials. Twelve subjects were exposed to 4°C cold air for 110 minutes, receiving either 150 mg/kg L-tyrosine or placebo in a double-blind crossover design.
The cognitive battery focused on working memory using a delayed matching-to-sample task. Subjects had to remember a target stimulus and then identify it after a delay among distractors. Under placebo + cold, working memory performance degraded significantly relative to a warm-baseline condition. Under tyrosine + cold, working memory performance was restored substantially toward the warm-baseline level. Statistical separation between tyrosine and placebo conditions was robust.
This study established that the cognitive benefit of tyrosine under cold was not driven by the altitude / hypoxia component of the earlier Banderet trial — cold alone was sufficient to produce the catecholamine depletion that tyrosine countered. The cleaner experimental design made it a useful citation for the cold-only operational use case.
Mahoney 2007 — Repeat Cold + Working Memory
Mahoney and colleagues at USARIEM in 2007 extended the cold + tyrosine paradigm with a more complex repeated-exposure design. Subjects were exposed to two cold-water immersion (foot in 4°C water) protocols on separate days, receiving 150 mg/kg L-tyrosine on one day and placebo on the other in randomized order. The working memory battery (Sternberg item recognition task, mental subtraction, four-choice reaction time) was administered both before and during cold exposure.
Results replicated the Shurtleff finding: cold exposure under placebo significantly degraded working memory, while cold under tyrosine produced significantly less degradation. The effect was particularly strong for the four-choice reaction time task, which specifically taxes attentional resources, consistent with the locus-coeruleus norepinephrine substrate model.
The Mahoney protocol — immersion of an extremity in cold water as the stressor — is operationally relevant for special operations, swift-water rescue, and emergency cold-water survival. The reproducibility of the tyrosine benefit in this paradigm strengthens the operational evidence base.
O'Brien 2007 — Body Cooling Protocols
O'Brien and colleagues 2007 examined tyrosine in whole-body cooling rather than extremity immersion. Subjects underwent body cooling in a cold-air chamber sufficient to drop core temperature by approximately 0.5°C while wearing standardized inadequate clothing. Cognitive and psychomotor performance was assessed during the cooling and during a follow-up rewarming phase.
Tyrosine pre-loading (150 mg/kg) significantly improved cognitive performance during the body-cooling phase compared to placebo. Psychomotor task performance was also preserved. The whole-body cooling paradigm is closer to the operational scenario of soldiers, hikers, or workers exposed to cold-weather conditions without adequate shelter, making this evidence particularly applicable to field operational use.
The cumulative body of cold + tyrosine evidence (Banderet 1989, Shurtleff 1994, Mahoney 2007, O'Brien 2007) makes tyrosine one of the best-supported nutritional countermeasures for cold-environment cognitive performance. The mechanism is consistent across trials, the dose is consistent (100–150 mg/kg), and the effect is reproducible.
The Combined Stressors — Cold + Altitude + Sleep Loss
In real-world military and high-altitude operations, the three stressors of cold, hypoxia (altitude), and sleep deprivation often combine. Each individually produces catecholamine depletion; combined, they produce a substantially larger demand on the catecholamine system than any one alone. This is the operational profile of:
- Mountain warfare operations (Hindu Kush, Andes, Himalayan deployments)
- Special Forces winter operations (10th Mountain Division, Norwegian Marines, Swedish K3 jaegers)
- High-altitude alpine search-and-rescue
- Polar expedition science (Antarctica, Arctic research stations)
- Long-range arctic patrols (Canadian Rangers, NORAD detachments)
Banderet's 1989 trial deliberately combined cold (4°C) and hypoxia (4,700 meter equivalent altitude) to model this operational reality. The tyrosine benefit was robust in this combined stressor. The Neri 1995 sleep-deprivation trial added the third axis. Combined-stressor field studies in mountain warfare units have similarly shown tyrosine benefit, though with more variability due to operational confounds (food, hydration, individual fitness, mission complexity).
For multi-day combined operations, the protocol is typically pre-loading on the morning of high-demand operations, redosing every 3–4 hours during sustained periods, and combining with caffeine (the additive effect of stimulant + substrate is operationally useful) and adequate carbohydrate intake. Tyrosine is not a substitute for proper cold-weather preparation, acclimatization, hydration, fuel, or rest — it is an adjunct that softens the cognitive cliff when the protective measures are insufficient.
The Special Forces Cold Protocol
The operational protocol that has emerged from the USARIEM evidence base and from informal Special Forces operational practice (Army Special Forces, Navy SEALs, Norwegian Marinejegerkommandoen, British SAS) for cold-environment operations:
- Pre-load dose: 100–150 mg/kg of L-tyrosine (approximately 7–10 g for a 70 kg operator) taken 30–60 minutes before anticipated cold exposure onset. Empty stomach or with small carbohydrate load.
- Redose schedule: half the original dose (3–5 g) every 3–4 hours during sustained operations, until exposure ends or rest period begins.
- Caffeine stack: 200–400 mg caffeine concurrent with or slightly before the tyrosine dose, for additive cognitive support. Some protocols use the U.S. military stim-pack (caffeine + carbohydrate + tyrosine) for this purpose.
- Carbohydrate co-administration: 10–20 g simple carbohydrate with each tyrosine dose to accelerate absorption, support glucose for muscle shivering, and induce mild insulin response that lowers competing branched-chain amino acids at the blood-brain barrier.
- Hydration: adequate fluid intake throughout; dehydration substantially worsens cognitive performance independent of the cold and substantially limits any tyrosine benefit.
- Avoid co-administration of: high-protein meals (compete for blood-brain barrier transport), BCAA supplements (specifically compete with tyrosine at LAT1), L-DOPA (Parkinson's patients should not deploy with this protocol), and MAO inhibitors.
This protocol is not classified or restricted — it is consistent with the published evidence base and with standard nutritional supplement practice. It is appropriate for any operator, soldier, mountaineer, or field worker facing prolonged cold-environment cognitive performance demands.
Cold-Water Diving and Immersion Applications
Cold-water diving (commercial, scientific, military, recreational) is one of the most cognitively demanding cold scenarios civilian populations engage in. The combination of:
- Cold water producing rapid heat loss (water conducts heat approximately 25-fold faster than air)
- Decision-making under task load (gas management, depth control, decompression, navigation, equipment management)
- Time pressure (gas supply finite; decompression obligation accumulating)
- Often combined sleep loss (pre-dawn dive schedules)
- Hypoxia at depth (if breathing mixed gas)
produces a textbook substrate-limited catecholamine state. Tyrosine pre-loading 60–90 minutes before a planned cold-water dive is reasonable. The standard 100–150 mg/kg protocol applies. For technical dives with long bottom times and decompression obligations, the longer cold exposure makes the case stronger.
Practical caveats. Free amino acid dosing can cause mild GI upset, which is unpleasant in a dive context. Take with adequate water and ideally a small carbohydrate, well before the dive. Avoid heavy protein meals in the pre-dive window to maximize brain delivery. Combine with appropriate cold-water exposure protection (drysuit, hood, gloves) — tyrosine supports cognitive performance under cold stress but does not protect against hypothermia or peripheral cold injury.
Polar Research and Extreme Cold Expeditions
Polar field researchers, Antarctic station personnel, Arctic expedition members, and unsupported polar trekkers face sustained cold exposure over weeks to months. The acute tyrosine protocol does not translate directly to these chronic exposures — tolerance to high-dose tyrosine appears to develop over sustained dosing, possibly through TH down-regulation, possibly through tyrosine catabolism upregulation, possibly through receptor adaptations downstream.
For sustained polar operations, the more defensible use is acute pre-loading for specific high-demand periods (a difficult day's travel, a complex scientific operation in the field, a research aircraft landing on a remote ice runway) rather than daily prophylactic supplementation. The chronic cold acclimatization process itself (increased brown adipose tissue, increased sympathetic tone, increased thyroid hormone output) reduces the acute catecholamine demand of any given cold exposure, partially obviating the need for substrate support.
Some polar expedition medical kits include tyrosine for use on high-demand days. Some do not. The evidence does not currently support routine daily dosing across multi-month expeditions.
What Tyrosine Will Not Do for Cold (Limits)
Honest limits on the cold + tyrosine evidence base:
- Will not prevent frostbite or peripheral cold injury — vasoconstriction of cutaneous vessels under cold is mechanical and chemical; sustained adequate catecholamine output may marginally support distal perfusion in early cold exposure, but tyrosine does not provide meaningful protection against tissue freezing. Wear proper insulation.
- Will not prevent hypothermia — core temperature drop is a function of net heat balance (heat loss versus heat production). Tyrosine modestly supports thermogenesis through sustained sympathetic activation but cannot compensate for inadequate clothing or insulation. Wear proper insulation.
- Will not enhance baseline cold tolerance in unstressed individuals — the substrate-limitation mechanism requires the acute physiological stress that depletes catecholamines. Routine tyrosine dosing in subjects not facing acute cold stress produces no measurable cold tolerance improvement.
- Will not replace cold acclimatization — the long-term adaptation to cold (brown adipose tissue expansion, increased sympathetic tone, increased non-shivering thermogenesis) requires repeated exposure over weeks. Acute tyrosine supports a single cold exposure event; it does not produce the chronic adaptation.
- Will not work without adequate cofactors — iron deficiency, BH4 cofactor problems, B6 deficiency, copper deficiency, ascorbate deficiency can all blunt the catecholamine-synthesis benefit. Address underlying deficiencies.
- Will not produce stimulant-like overstimulation — tyrosine is a substrate, not a stimulant. The effect feels subtle (slightly more alert and capable under stress) rather than dramatic. Subjects expecting a coffee-like buzz are sometimes underwhelmed.
Practical Protocol Summary
- Anticipated cold exposure 1–4 hours: 100 mg/kg (7 g for a 70 kg adult) of L-tyrosine, 30–60 minutes before exposure, on relatively empty stomach with water and small carbohydrate (10–20 g).
- Anticipated cold exposure 4–12 hours: initial 100–150 mg/kg dose, plus redose of half that amount every 3–4 hours during the exposure period.
- Combined cold + sleep loss + altitude: same dosing, with caffeine 200–400 mg added at the start. This is the Banderet/Neri operational regimen.
- Cold-water diving: 100–150 mg/kg 60–90 minutes pre-dive, with adequate hydration and pre-dive carbohydrate.
- Special operations sustained operations: as above with redosing; coordinate with caffeine and meal timing for sustained 12–48 hour mission profiles.
- Avoid in: hyperthyroid patients, Parkinson's patients on L-DOPA, patients on MAO inhibitors, active melanoma, pregnancy (without medical guidance).
- Common side effects at high dose: mild GI upset (nausea, loose stool) from osmotic load, easily mitigated by split dosing. Mild headache occasionally reported. Insomnia if taken late in the day.
Key Research Papers
- Banderet LE, Lieberman HR (1989). Treatment with tyrosine, a neurotransmitter precursor, reduces environmental stress in humans. Brain Research Bulletin. — PubMed
- Shurtleff D et al. (1994). Tyrosine reverses a cold-induced working memory deficit in humans. Pharmacology Biochemistry and Behavior. — PubMed
- Mahoney CR et al. (2007). Tyrosine supplementation mitigates working memory decrements during cold exposure. Physiology & Behavior. — PubMed
- O'Brien C et al. (2007). Dietary tyrosine benefits cognitive and psychomotor performance during body cooling. Physiology & Behavior. — PubMed
- Lieberman HR (2003). Nutrition, brain function and cognitive performance. Appetite. — PubMed
- Cuddy JS et al. (2007). Skin temperature and heart rate can be used to estimate physiological strain during exercise in the heat in a cohort of fit and unfit males. Military Medicine. — PubMed
- Castellani JW, Young AJ (2016). Human physiological responses to cold exposure: acute responses and acclimatization to prolonged exposure. Autonomic Neuroscience. — PubMed
- Young AJ et al. (1986). Cooling different body surfaces during upper and lower body exercise. Journal of Applied Physiology. — PubMed
- Stocks JM et al. (2004). Human physiological responses to cold exposure. Aviation, Space, and Environmental Medicine. — PubMed
- Cannon B, Nedergaard J (2004). Brown adipose tissue: function and physiological significance. Physiological Reviews. — PubMed
- Lieberman HR et al. (2002). A double-blind, placebo-controlled test of 2 d of calorie deprivation: effects on cognition, activity, sleep, and interstitial glucose concentrations. American Journal of Clinical Nutrition. — PubMed
- Coull NA et al. (2015). Tyrosine ingestion and its effects on cognitive and physical performance in the heat. Medicine & Science in Sports & Exercise. — PubMed
- Tipton MJ et al. (2017). Cold water immersion: kill or cure? Experimental Physiology. — PubMed
- Muza SR et al. (2001). Wearing a hood reduces respiratory water loss and oxygen consumption in cold exposed humans. Aviation Space Environmental Medicine. — PubMed
PubMed Topic Searches
- PubMed: Tyrosine and cold exposure cognition
- PubMed: Catecholamine response to cold
- PubMed: Brown adipose thermogenesis
- PubMed: Military cold-weather operations
- PubMed: Cold-water immersion cognition
Connections
- Dopamine, Reward & How Habits Hijack You — interactive animation
- Tyrosine Overview
- Tyrosine Benefits Hub
- Tyrosine for Stress & Cognitive Performance
- Tyrosine for Dopamine & Mood
- Tyrosine for Thyroid Function
- Phenylalanine (Precursor)
- Tryptophan
- Fatigue
- Brain Fog
- ADHD
- Vitamin B6 (AADC Cofactor)
- Vitamin C (DBH Cofactor)
- Iron (TH Cofactor)
- Iodine
- Selenium
- All Amino Acids
- Cold Exposure — the practice page on cold plunges, showers, and acclimation.