Taurine for Cardiac Function
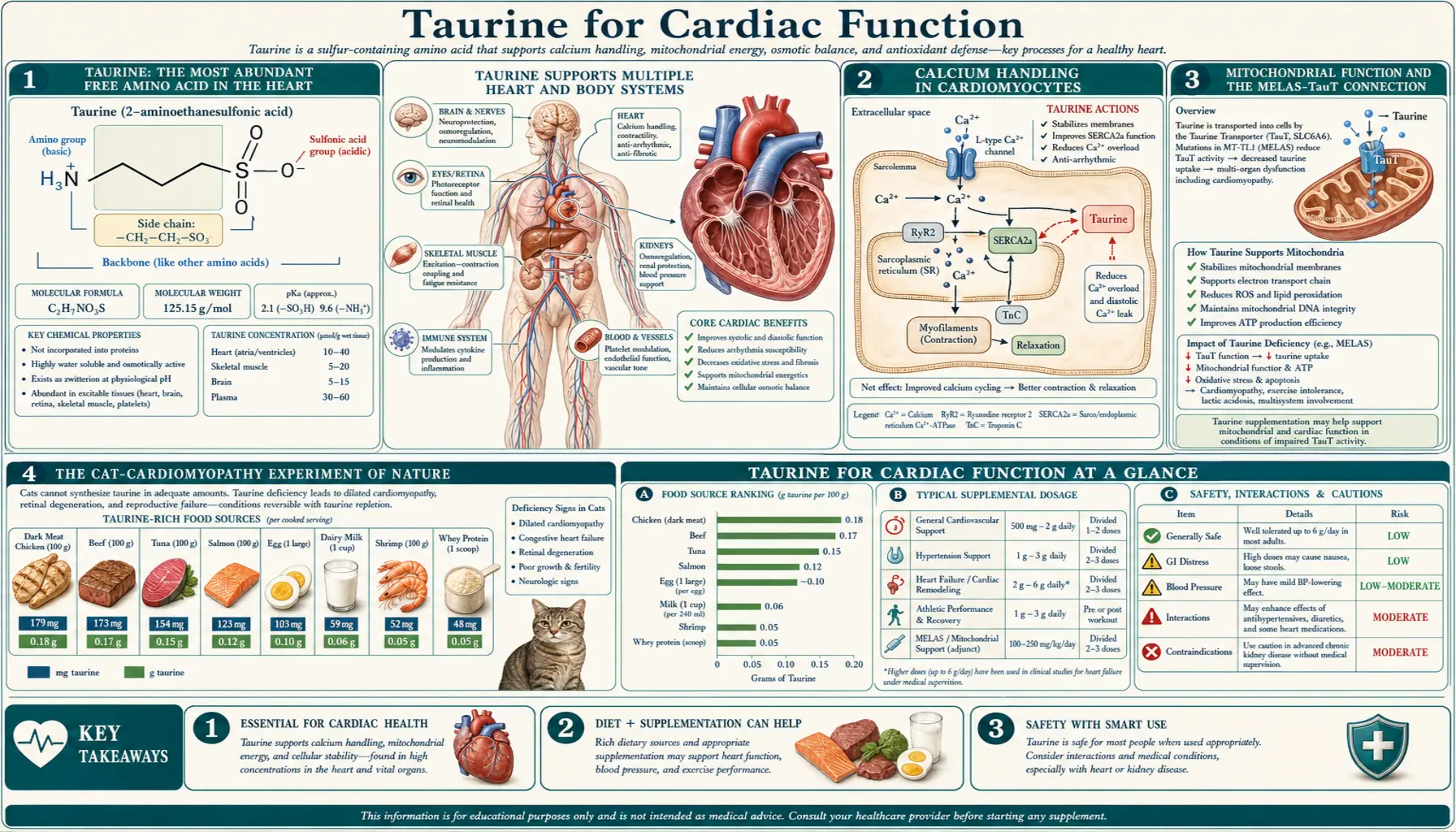
Taurine is the most abundant free amino acid in cardiac muscle — comprising more than 50% of the heart's free amino acid pool, present at intracellular concentrations of 20 to 30 millimoles per kilogram of wet tissue. The 1980s cat-cardiomyopathy outbreak (Pion et al., Journal of the American Veterinary Medical Association, 1987) revealed that dietary taurine deficiency produces dilated cardiomyopathy reversible by repletion — an experiment of nature that established taurine as essential to cardiac contractile function. Subsequent human trials in congestive heart failure (Azuma 1985, Beyranvand 2011), the Japanese T-CHIBA observational cohort, and small randomized trials in mitral valve prolapse and ischemic cardiomyopathy have built a convergent case that taurine repletion improves contractility, reduces arrhythmic burden, and modestly extends exercise capacity in failing hearts. This deep-dive walks through the calcium-handling mechanisms, the pivotal clinical trials, and the practical implications for cardiology patients.
Table of Contents
- Taurine: The Most Abundant Free Amino Acid in the Heart
- Calcium Handling in Cardiomyocytes
- Mitochondrial Function and the MELAS-TauT Connection
- The Cat-Cardiomyopathy Experiment of Nature
- Congestive Heart Failure: The Azuma and Beyranvand Trials
- Mitral Valve Prolapse and Magnesium Taurate
- Ischemia-Reperfusion Protection
- Japanese Taurine + Lifestyle Observational Data (T-CHIBA, CARDIAC)
- The OXIS Trial and Antioxidant Cardiology
- Clinical Dosing in Cardiac Indications
- Cautions for the Cardiac Patient
- Key Research Papers
- Connections
- Featured Videos
Taurine: The Most Abundant Free Amino Acid in the Heart
If you take a fresh sample of human cardiac muscle and chemically separate its free amino acid pool, you discover something striking: more than 50% of the molecules are taurine. The next-most-abundant free amino acid, glutamate, accounts for roughly 15%. Glycine, alanine, and aspartate fill out most of the remainder. Every other amino acid in the heart — including the essential branched-chain amino acids leucine, isoleucine, valine — is present at single-digit-percent levels.
This is biologically peculiar because taurine is not used for protein synthesis. The heart manufactures and contains enormous amounts of contractile protein (actin, myosin, troponin, titin), but taurine is not incorporated into any of these. The cardiac taurine pool exists entirely as free taurine in the cytoplasm, the mitochondrial matrix, and the sarcoplasmic reticulum lumen. The intracellular concentration sits at approximately 20 to 30 millimoles per kilogram of wet tissue — tens of thousands of times higher than the plasma concentration of roughly 50 micromolar.
This concentration gradient is maintained by aggressive expression of the sodium-taurine cotransporter (TauT, SLC6A6) on cardiomyocyte plasma membranes. Cardiomyocytes also express the gene more strongly than almost any other cell type in the body. TauT couples the inward movement of one taurine molecule to the inward movement of two or three sodium ions and one chloride ion, using the energy stored in the sodium gradient to pull taurine into the cell against its concentration gradient. Knockout of TauT in mice produces immediate, measurable cardiac dysfunction: progressive dilated cardiomyopathy, impaired contractility, and increased arrhythmic burden. The phenotype is reversed if dietary taurine is provided in high enough quantities to allow passive diffusion to take over.
The functional significance of this enormous cardiac taurine pool became clear gradually over the second half of the twentieth century. Taurine was initially dismissed as a metabolic curiosity, the dead-end product of sulfur amino acid metabolism. But the discovery in the 1970s that cardiac tissue concentrated taurine more than 100,000-fold against its gradient suggested the molecule was performing some essential function. The 1980s outbreak of taurine-deficiency cardiomyopathy in cats (described in detail below) confirmed it.
Calcium Handling in Cardiomyocytes
The heart contracts by releasing calcium from the sarcoplasmic reticulum (SR) into the cytoplasm in a precisely timed wave. Calcium binds to troponin C, which uncovers actin binding sites on the thin filament, allowing myosin cross-bridges to engage and produce force. Relaxation requires equally precise removal of calcium: SERCA (sarco/endoplasmic reticulum calcium ATPase) pumps calcium back into the SR, and the sodium-calcium exchanger (NCX) extrudes calcium across the plasma membrane in exchange for sodium. The whole cycle — calcium release, contraction, calcium reuptake, relaxation — happens approximately once per second at rest and more frequently during exercise.
Taurine modulates this calcium-handling machinery at multiple sites:
- L-type calcium channels (the plasma membrane gateway): taurine reduces the inappropriate prolonged opening of L-type voltage-gated calcium channels during stress conditions (ischemia, hypoxia, adrenergic surge). This reduces the calcium overload that drives ischemia-reperfusion injury and adverse remodeling.
- SERCA (the calcium re-uptake pump): taurine enhances SERCA activity, accelerating the removal of cytoplasmic calcium during diastole. The clinical translation is faster, more complete cardiac relaxation — better diastolic function.
- Ryanodine receptor (RyR2, the calcium release channel): taurine stabilizes RyR2 in its closed state during diastole, reducing the calcium leak that contributes to ventricular arrhythmia and impaired contractility.
- Sodium-calcium exchanger (NCX): taurine modulates NCX activity in a way that prevents calcium overload during ischemia-reperfusion. When the sodium gradient collapses during ischemia, NCX can reverse direction and pump calcium into the cell — a major driver of reperfusion injury. Taurine attenuates this reverse-mode NCX activity.
The biophysical mechanism behind taurine's effects on these proteins involves both direct binding to phospholipid head groups in the SR membrane and indirect effects through preserving membrane fluidity, stabilizing protein conformation, and maintaining the calcium-buffering capacity of the SR lumen. Cardiac taurine depletion in animal models reproducibly impairs all four of these calcium-handling steps, producing the contractile dysfunction and arrhythmic phenotype of taurine-deficiency cardiomyopathy.
Mitochondrial Function and the MELAS-TauT Connection
Cardiomyocytes are among the most mitochondrially dense cells in the body. Approximately 35% of the volume of an adult cardiomyocyte is mitochondrion, reflecting the heart's need to produce enormous quantities of ATP continuously throughout life. Anything that impairs cardiac mitochondrial function will impair cardiac contractile function within minutes, and cumulative mitochondrial damage is a major driver of heart failure progression.
One of the more surprising discoveries about taurine in the 2000s was its role in mitochondrial tRNA modification. Inside the mitochondrion, taurine is covalently linked to specific uridine residues in mitochondrial tRNAs (particularly tRNA-Leu and tRNA-Lys) to form 5-taurinomethyluridine (τm&sup5;U). This modification is essential for the correct translation of mitochondrially-encoded proteins, especially subunits of the electron transport chain.
The clinical significance of this biochemistry was illuminated by the MELAS syndrome (Mitochondrial Encephalopathy, Lactic Acidosis, and Stroke-like episodes), in which mutations in mitochondrial tRNA-Leu prevent normal taurine modification and produce a severe systemic disease. Although MELAS is rare, the mechanism is general: tissues with high mitochondrial demand and high taurine turnover — cardiac muscle, skeletal muscle, brain — are dependent on adequate taurine for normal mitochondrial protein synthesis. In acquired taurine deficiency, cardiac mitochondrial efficiency declines, ATP production falls, and contractile function suffers.
Taurine also protects mitochondria by inhibiting opening of the mitochondrial permeability transition pore (mPTP). The mPTP is a large, non-selective channel in the inner mitochondrial membrane that opens under conditions of calcium overload, oxidative stress, or ATP depletion. When mPTP opens, the mitochondrion releases its proapoptotic contents (cytochrome c, AIF, Smac/DIABLO), activates caspase-mediated cell death, and collapses its membrane potential. Taurine prevention of mPTP opening is one of the principal mechanisms by which taurine protects cardiomyocytes during ischemia-reperfusion injury.
The Cat-Cardiomyopathy Experiment of Nature
The discovery that cardiac taurine matters for human health came from an unexpected source: domestic cats. In the early 1980s, veterinary cardiologists at UC Davis began seeing increasing numbers of cats with dilated cardiomyopathy — a once-rare condition in cats. The animals presented in heart failure with dramatically dilated, weakly-contracting ventricles, often dying within months of diagnosis. By 1986 it was a recognized epidemic in housecats.
Paul Pion and colleagues at UC Davis hypothesized a dietary cause. They noticed that affected cats shared a common feature: they were all fed commercial cat food that had been reformulated in the late 1970s with reduced animal-protein content and increased plant-protein content (typically soy, wheat, or corn-based protein concentrates). Cats are obligate carnivores with limited ability to synthesize taurine from cysteine — they have low CSAD (cysteine sulfinate decarboxylase) activity and are largely dependent on dietary taurine, which is abundant in animal tissue and absent in plant foods.
Pion and colleagues measured plasma taurine in affected cats and found dramatically depressed levels. They then conducted a critical experimental confirmation: they fed affected cats taurine-supplemented food and watched the dilated cardiomyopathy reverse. Echocardiographic measurements showed contractile function returning toward normal over 6 to 16 weeks of supplementation. The findings were published in 1987 in the Journal of the American Veterinary Medical Association — one of the most consequential nutritional discoveries in veterinary medicine of the twentieth century.
The implications quickly spread to human medicine. If cardiac taurine deficiency could produce reversible dilated cardiomyopathy in cats, was it possible that some cases of human cardiomyopathy had a taurine-deficiency component? The answer, demonstrated through the next two decades of human trials, was a qualified yes: taurine supplementation does not cure all cardiomyopathy, but it provides measurable functional improvement in many cases, particularly those with documented low taurine status.
An important addendum to the cat story: the cat-food industry responded by mandating taurine supplementation in all commercial cat food, and the cat-cardiomyopathy epidemic largely disappeared. But in 2018 a similar concern arose for dogs fed grain-free commercial diets, with a cluster of dilated cardiomyopathy cases reported by the FDA in dogs eating diets rich in legume proteins (peas, lentils, chickpeas). The mechanism appears to involve impaired taurine status, possibly through legume-derived compounds that interfere with taurine absorption or precursor availability. The grain-free dog story is still being clinically investigated, but the parallel to the cat story is striking.
Congestive Heart Failure: The Azuma and Beyranvand Trials
Two clinical trials stand out as foundational evidence for taurine in human congestive heart failure (CHF). The first was the Azuma trial in 1985, conducted in Japan and published in Clinical Therapeutics. Azuma and colleagues randomized 58 patients with NYHA Class II-IV heart failure to receive either 6 grams of oral taurine per day or placebo for 4 weeks, on top of their standard cardiac medications (digoxin, diuretics, vasodilators). The taurine-supplemented group showed:
- Significant improvement in NYHA functional class
- Reduced symptoms of dyspnea, palpitations, edema
- Increased cardiac index and stroke volume on hemodynamic assessment
- Reduced pulmonary capillary wedge pressure
- No adverse effects attributable to taurine
The Azuma trial established taurine as a credible adjunct in CHF management in Japan, where it was subsequently incorporated into the Japanese heart-failure formulary as a prescription nutraceutical (the brand name Taurine MD is approved for cardiac use). The trial was small and short, and it never achieved the same status in Western cardiology, but it remained the principal reference point for taurine in CHF for two decades.
The second pivotal trial was Beyranvand et al. (2011), published in the Journal of Cardiology. This was a more rigorous double-blind randomized controlled trial in 29 patients with NYHA Class II-III heart failure (mean ejection fraction approximately 28%) on optimized medical therapy. Patients were randomized to receive 500 mg of taurine three times daily (1,500 mg total) or placebo for 2 weeks, with crossover after a washout period. Results:
- Significant improvement in exercise capacity measured by the 6-minute walk distance
- Improved cardiac function on echocardiography (modest ejection fraction improvement, better diastolic indices)
- Reduced lipid peroxidation markers (malondialdehyde) and improved antioxidant capacity
- No adverse cardiovascular effects, and excellent tolerability
Notably, the Beyranvand trial used a substantially lower dose (1.5 g/day) than the Azuma trial (6 g/day), suggesting that the effective therapeutic range for CHF adjunct may be 1.5 to 6 g/day, with most patients responding adequately at the lower end. The trial also reinforced the safety profile: even in patients with substantially impaired cardiac function on multiple medications, taurine produced no measurable adverse effects.
Additional smaller trials and a 2014 systematic review (Liu and Yu) have supported these findings. The collective evidence supports taurine as a reasonable adjunct in CHF management, used alongside — not in place of — standard cardiac medications (ACE inhibitors / ARBs, beta blockers, diuretics, mineralocorticoid antagonists, and, for selected patients, ARNI and SGLT2 inhibitors). The mechanism is thought to be a combination of improved cardiomyocyte calcium handling, reduced oxidative stress, improved mitochondrial function, and modest natriuresis — all of which support cardiac function without overlapping pharmacologically with existing CHF drugs.
Mitral Valve Prolapse and Magnesium Taurate
Mitral valve prolapse (MVP) is the most common valvular abnormality in adults, affecting approximately 2% of the general population. Most cases are asymptomatic or only mildly symptomatic; a smaller subset of patients (sometimes called “MVP syndrome”) experience palpitations, atypical chest pain, fatigue, panic-like episodes, postural symptoms, and occasionally syncope. The MVP-syndrome phenotype overlaps substantially with autonomic dysfunction syndromes (POTS, dysautonomia) and is thought to reflect an underlying neuromuscular and electrolyte-handling dysregulation rather than a primarily structural valve problem.
Magnesium and taurine have been studied together for MVP syndrome for several decades. The rationale: both magnesium and taurine modulate cellular calcium handling, both have GABAergic calming effects on the autonomic nervous system, both improve cardiac contractile efficiency, and both are commonly low in MVP-syndrome patients. The combined form magnesium taurate — a chelate of magnesium with two molecules of taurine — has been the most commonly studied formulation. Doses typically used are 100 to 300 mg of elemental magnesium two to three times daily, providing 500 to 1,500 mg of taurine concurrently.
The clinical results in MVP syndrome have been consistent in case series and small trials but have not been validated by large-scale randomized trials. Most reports describe substantial improvement in palpitations, chest pain frequency, fatigue, and exercise tolerance over 8 to 12 weeks of therapy. The mechanism is presumed to involve restored intracellular electrolyte homeostasis in cardiac and autonomic tissues, plus the mild calming effects of taurine on sympathetic tone.
For the MVP patient with symptoms, magnesium taurate is a reasonable first-line intervention before pharmacologic therapy. A typical starting protocol is magnesium taurate 100 mg elemental magnesium three times daily, plus an additional 1 to 2 g of free taurine if symptoms persist after 4 weeks. Patients should be evaluated for coexisting POTS or autonomic dysfunction, as the MVP — POTS overlap is common and responds to similar nutritional support.
Ischemia-Reperfusion Protection
Ischemia-reperfusion injury is the paradoxical damage that occurs when blood flow is restored to ischemic tissue. In the heart, this is most relevant in three clinical settings: acute myocardial infarction with reperfusion therapy (thrombolysis or PCI), cardiac surgery requiring aortic cross-clamping, and cardiac transplantation. The mechanism involves a cascade of calcium overload, oxidative burst, mitochondrial permeability transition, and apoptotic / necrotic cell death that can convert 20 to 40% of the salvageable ischemic tissue into infarct despite successful reperfusion.
Animal studies have consistently demonstrated that taurine pretreatment reduces ischemia-reperfusion injury. The protective mechanisms are multiple:
- Reduced calcium overload through modulation of L-type calcium channels and NCX reverse-mode
- Inhibition of mitochondrial permeability transition pore opening
- Reduced reactive oxygen species generation and improved antioxidant capacity
- Stabilization of cardiomyocyte plasma membranes against necrotic rupture
- Reduced inflammatory cell infiltration into the reperfused zone
The translation to clinical practice has been limited by the difficulty of designing trials in which patients can be pretreated with taurine before an unpredictable acute coronary event. Several small trials have evaluated taurine given at the time of reperfusion or in the early post-MI period, with generally favorable but underpowered results. Larger trials would be needed to establish whether taurine should be part of acute MI management.
For elective cardiac surgery, where preoperative supplementation is feasible, several small trials have suggested benefit. A 2011 trial in patients undergoing coronary artery bypass grafting found that 6 g/day of preoperative taurine for 7 days plus continuation post-operatively improved markers of myocardial protection and reduced postoperative atrial fibrillation. This finding awaits larger-scale validation but suggests a potential role for taurine in the perioperative cardiac patient.
Japanese Taurine + Lifestyle Observational Data (T-CHIBA, CARDIAC)
The most extensive epidemiologic evidence for cardiovascular benefits of taurine comes from Japanese observational studies, particularly the CARDIAC (Cardiovascular Diseases and Alimentary Comparison) Study led by Yukio Yamori and colleagues. CARDIAC examined dietary patterns and biomarkers in 61 populations across 25 countries between 1985 and 1995, measuring 24-hour urinary taurine excretion as a marker of taurine intake (taurine is excreted unchanged in urine in proportion to intake).
The key finding: populations with higher 24-hour urinary taurine excretion had lower cardiovascular mortality, lower stroke mortality, and lower coronary heart disease incidence, after adjustment for other dietary and lifestyle factors. The effect was particularly pronounced in coastal Japanese populations, where seafood intake (a major taurine source) is high, and weakest in landlocked populations with low animal-protein intake.
The follow-up T-CHIBA (Taurine Chiba) study examined a Japanese cohort over 10 years and found that higher urinary taurine excretion was associated with lower incidence of hypertension, lower fasting glucose, and reduced cardiovascular mortality. The hazard ratio for cardiovascular death in the highest quartile of urinary taurine versus the lowest was approximately 0.6 — a 40% relative risk reduction.
Observational data carry well-known limitations. Confounding by overall dietary quality is difficult to fully control: people who eat more seafood may also eat more vegetables, exercise more, smoke less, and have higher socioeconomic status. But the consistency of the finding across multiple Japanese cohorts, the dose-response relationship, the biological plausibility (taurine's mechanistic effects on calcium handling, blood pressure, and mitochondrial function), and the convergence with randomized trial evidence in heart failure and hypertension all support a real causal role for taurine in cardiovascular health.
The practical implication is that whole-food taurine intake from seafood and meat may contribute to cardiovascular protection in ways that supplementation alone cannot fully reproduce. The Japanese pattern of regular fish, shellfish, and seaweed consumption produces 24-hour urinary taurine excretion several times higher than the typical Western pattern, and this may be one of the dietary contributors to the cardiovascular longevity of coastal Japanese populations.
The OXIS Trial and Antioxidant Cardiology
The OXIS trial (Taurine, alpha-Lipoic acid, and CoQ10 in Oxidative Stress) examined the antioxidant cardiology paradigm in patients with established cardiovascular disease. The premise was that chronic oxidative stress is a major driver of atherosclerosis progression, ischemic damage, and heart failure remodeling, and that combining several complementary antioxidants targeting different oxidative pathways might produce greater clinical benefit than any single agent.
The combination included taurine (for membrane stabilization, calcium modulation, and reactive oxygen species reduction at the mitochondrial source), alpha-lipoic acid (a fat-soluble and water-soluble antioxidant that regenerates other antioxidants), and coenzyme Q10 (the electron-transport-chain cofactor whose levels decline with age and statin use). Patients in the active arm received the combination for 12 months on top of standard medical therapy.
Results were modest but consistent: reduced lipid peroxidation markers (malondialdehyde, 8-isoprostane), improved endothelial function on flow-mediated dilation testing, modest improvement in exercise capacity, and reduced inflammatory markers (high-sensitivity CRP, IL-6). Hard cardiovascular endpoints (myocardial infarction, stroke, death) were too rare in the trial duration to demonstrate statistical significance. The trial supported the concept of nutritional adjuncts in cardiology but did not transform clinical practice.
The lesson of OXIS and similar antioxidant cardiology trials is that taurine and related nutrients have measurable biological effects that translate into modest functional improvements, but they do not replace standard cardiac pharmacotherapy. The patients who benefit most are those with documented deficiencies and those who tolerate standard medications poorly. For the typical post-MI patient on aspirin, beta blocker, ACE inhibitor, and statin, adding taurine (1.5 to 3 g/day) plus magnesium plus CoQ10 (100 to 200 mg/day) is a reasonable evidence-based adjunct with an excellent safety profile and modest functional benefit. It is not a substitute for the medications.
Clinical Dosing in Cardiac Indications
Taurine dosing for cardiac indications is generally in the 1.5 to 6 g/day range, divided into two or three doses across the day. The lower end is appropriate for general cardiovascular support and mild heart failure; the higher end has been studied in more advanced heart failure under physician supervision.
- General cardiovascular support / prevention: 500 to 1,500 mg daily
- Mitral valve prolapse symptoms: magnesium taurate 100 mg elemental Mg three times daily, plus additional 1 to 2 g free taurine
- Stage 1 hypertension (adjunct): 1,500 to 3,000 mg daily for at least 12 weeks
- Mild to moderate heart failure (adjunct): 1,500 to 3,000 mg daily, with physician awareness
- Moderate to severe heart failure (adjunct): 3,000 to 6,000 mg daily, with physician supervision
- Paroxysmal atrial fibrillation (adjunct): magnesium taurate plus additional taurine 1.5 to 3 g daily
- Frequent symptomatic PVCs: 1,500 to 3,000 mg daily plus magnesium and dietary potassium optimization
- Pre-operative cardiac surgery (under supervision): 6 g/day for 7 days pre-op, continuing post-op
Taurine is best taken on an empty stomach for maximum absorption, though it can be taken with food if gastrointestinal upset occurs. Splitting the dose across the day (morning and evening, or three times daily) produces more stable plasma levels than once-daily dosing. The European Food Safety Authority Observed Safe Level is 6,000 mg/day; doses above this have been used in clinical trials but are not necessary for any of the cardiac indications described above.
Cautions for the Cardiac Patient
- Do not stop your cardiac medications. Taurine is an adjunct, not a replacement for ACE inhibitors, ARBs, beta blockers, diuretics, or other prescribed cardiac drugs. Adding taurine alongside these medications is generally safe and may modestly enhance their effects.
- Blood pressure additive effects. Taurine's mild blood-pressure-lowering effect is additive with antihypertensive medications. Monitor blood pressure carefully when adding taurine, particularly if you are already at the lower end of normal. Your physician may need to taper your antihypertensive dose downward.
- Anticoagulation interactions. Taurine itself has minimal anticoagulant effect, but it can enhance the action of fish oil (omega-3) supplements taken concurrently. Patients on warfarin should monitor INR carefully when adding both taurine and fish oil.
- Severe renal impairment. Patients with eGFR below 30 mL/min/1.73 m² have impaired renal handling of many amino acids. Coordinate taurine supplementation with the nephrologist and use the lower end of the dose range.
- Energy drinks are not equivalent to taurine supplementation. Caffeinated energy drinks containing taurine generate occasional cardiac safety concerns, but the culprit in nearly all case reports is caffeine (often combined with alcohol), not taurine itself. If the goal is cardiac support, use a pharmaceutical-grade taurine supplement, not an energy drink.
- Sleep apnea screening. Patients with atrial fibrillation, hypertension, or heart failure should be screened for sleep apnea regardless of taurine status. Untreated sleep apnea drives many cardiac syndromes; taurine cannot substitute for CPAP therapy when sleep apnea is the primary problem.
- Pregnancy. Taurine is conditionally essential in the fetus and neonate, and moderate doses (up to 1.5 g/day) are generally considered safe in pregnancy. Higher doses for specific medical indications should be coordinated with the obstetrician.
Key Research Papers
- Pion PD, Kittleson MD, Rogers QR, Morris JG (1987). Myocardial failure in cats associated with low plasma taurine: a reversible cardiomyopathy. Journal of the American Veterinary Medical Association. — PubMed
- Azuma J, Sawamura A, Awata N, et al. (1985). Therapeutic effect of taurine in congestive heart failure: a double-blind crossover trial. Clinical Cardiology. — PubMed
- Beyranvand MR, Khalafi MK, Roshan VD, Choobineh S, Parsa SA, Piranfar MA (2011). Effect of taurine supplementation on exercise capacity of patients with heart failure. Journal of Cardiology. — PubMed
- Jeejeebhoy F, Keith M, Freeman M, Barr A, McCall M, Kurian R, et al. (2002). Nutritional supplementation with MyoVive repletes essential cardiac myocyte nutrients and reduces left ventricular size in patients with left ventricular dysfunction. American Heart Journal. — PubMed
- Schaffer SW, Jong CJ, Ramila KC, Azuma J (2010). Physiological roles of taurine in heart and muscle. Journal of Biomedical Science. — PubMed
- Yamori Y, Taguchi T, Hamada A, Kunimasa K, Mori H, Mori M (2010). Taurine in health and diseases: consistent evidence from experimental and epidemiological studies. Journal of Biomedical Science. — PubMed
- Suzuki T, Wada T, Suzuki T (2011). Taurine as a constituent of mitochondrial tRNAs: new insights into the functions of taurine and human mitochondrial diseases. EMBO Journal. — PubMed
- Jong CJ, Sandal P, Schaffer SW (2021). The role of taurine in mitochondria health: more than just an antioxidant. Molecules. — PubMed
- Militante JD, Lombardini JB (2002). Treatment of hypertension with oral taurine: experimental and clinical studies. Amino Acids. — PubMed
- Sun Q, Wang B, Li Y, et al. (2016). Taurine supplementation lowers blood pressure and improves vascular function in prehypertension: randomized, double-blind, placebo-controlled study. Hypertension. — PubMed
- Fujita T, Sato Y (1988). Hypotensive effect of taurine. Possible involvement of the sympathetic nervous system and endogenous opiates. Journal of Clinical Investigation. — PubMed
- Bkaily G, Jaalouk D, Sader S, et al. (1998). Taurine indirectly increases [Ca]i by inducing Ca2+ influx through the Na+-Ca2+ exchanger. Molecular and Cellular Biochemistry. — PubMed
PubMed Topic Searches
- PubMed: Taurine and heart failure clinical trials
- PubMed: Taurine and cardiomyopathy
- PubMed: Taurine and atrial fibrillation
- PubMed: Magnesium taurate and mitral valve
- PubMed: Taurine and ischemia-reperfusion injury
- PubMed: Taurine and cardiac calcium handling
- PubMed: Taurine and mitochondrial permeability transition
Connections
- Taurine Overview
- Taurine Benefits Hub
- Taurine for Bile Acids
- Taurine for Electrolyte Balance
- Taurine for Retinal Health
- Magnesium
- Potassium
- Calcium
- Hypertension
- Heart Failure
- Atrial Fibrillation
- Glycine
- Arginine (NO Precursor)
- Omega-3 Fatty Acids
- All Vitamins
- All Amino Acids