Taurine for Bile Acids and Fat Digestion
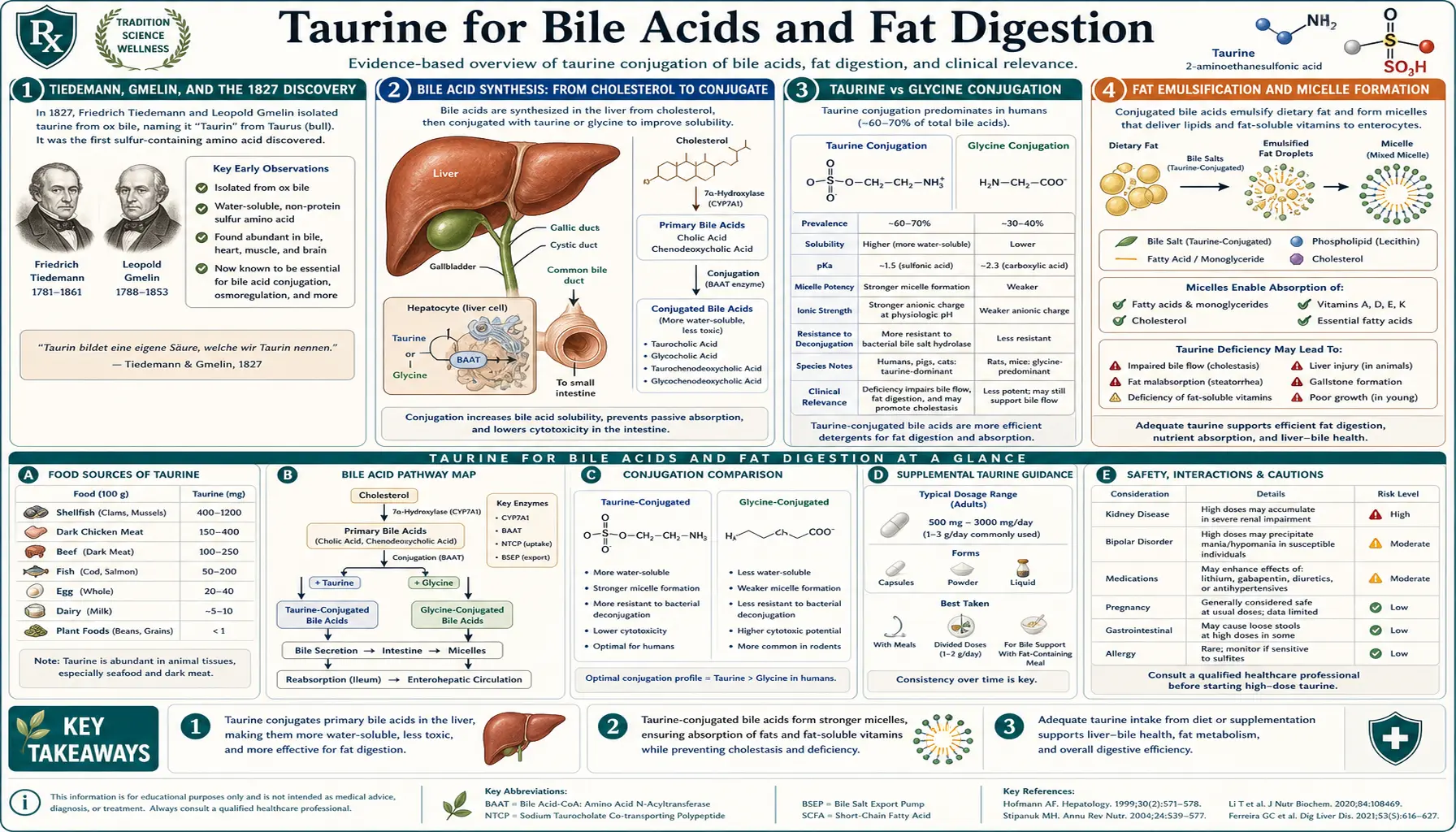
Taurine was first isolated from ox bile in 1827 by Friedrich Tiedemann and Leopold Gmelin — the molecule's very name derives from taurus, the Latin for “bull,” reflecting where chemistry first found it. Nearly two centuries later, the original function for which taurine was discovered remains one of its most important: it conjugates with primary bile acids in the liver to form taurocholic acid and taurochenodeoxycholic acid, the principal detergents the body uses to emulsify dietary fat and absorb the fat-soluble vitamins A, D, E, and K. Compared to glycine-conjugated bile salts, taurine-conjugated forms are more soluble in the acidic upper small intestine, more resistant to bacterial deconjugation in the colon, and more effective at stimulating bile flow (choleresis). This deep-dive walks through the bile acid synthesis pathway, the taurine-versus-glycine conjugation choice, the clinical implications of inadequate bile flow, and the role of taurine supplementation in cholestasis, gallbladder removal, ileal disease, and fat malabsorption syndromes.
Table of Contents
- Tiedemann, Gmelin, and the 1827 Discovery
- Bile Acid Synthesis: From Cholesterol to Conjugate
- Taurine vs Glycine Conjugation
- Fat Emulsification and Micelle Formation
- Absorption of Vitamins A, D, E, and K
- The Enterohepatic Circulation and ASBT
- Choleresis and Biliary Flow Dynamics
- Cholestasis: Intrahepatic and Extrahepatic
- After Gallbladder Removal
- FXR and TGR5: Bile Acids as Hormones
- Cholesterol Gallstones and Tauroursodeoxycholic Acid
- Practical Dosing for Bile-Acid Indications
- Cautions and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
Tiedemann, Gmelin, and the 1827 Discovery
In 1827, two German scientists working at the University of Heidelberg — Friedrich Tiedemann (an anatomist) and Leopold Gmelin (a chemist) — isolated a previously unknown organic compound from ox bile. They named it “Gallen-Asparagin,” or bile asparagine, because they initially thought it resembled the amino acid asparagine. The name did not stick. By the 1840s, French and German chemists had renamed the compound taurine, from taurus, Latin for bull or ox — the source organism from which the molecule had been first isolated.
Tiedemann and Gmelin's discovery established the connection between bile and taurine that defines the molecule's name to this day. They could not have known the full biochemistry: taurine is not the bile acid itself but the molecule that the liver conjugates onto primary bile acids to make them functional. The free taurine they isolated from ox bile was actually a hydrolysis product of taurocholic acid and taurochenodeoxycholic acid, which break down into free taurine plus free bile acid when bile is processed.
For more than a century after the discovery, taurine's biological role was thought to be limited to bile acid conjugation. The molecule was dismissed as a dead-end product of sulfur metabolism, biologically inactive in its own right. Only in the second half of the twentieth century did the broader functions of taurine begin to be recognized — the cardiac role (see Cardiac Function), the retinal role (see Retinal Health), the osmolyte role (see Electrolyte Balance). But the bile acid conjugation function, the one Tiedemann and Gmelin glimpsed in 1827, remains one of taurine's most consequential biological activities.
Bile Acid Synthesis: From Cholesterol to Conjugate
Bile acids are synthesized in the liver from cholesterol via two main pathways:
- The classical (neutral) pathway begins with cholesterol 7-alpha-hydroxylase (CYP7A1), the rate-limiting enzyme of bile acid synthesis. Through a series of about 15 enzymatic steps, cholesterol is hydroxylated, side-chain shortened, and modified to produce the two primary human bile acids: cholic acid (a trihydroxy bile acid) and chenodeoxycholic acid (CDCA) (a dihydroxy bile acid). This pathway accounts for roughly 75% of bile acid synthesis under normal conditions.
- The alternative (acidic) pathway begins with sterol 27-hydroxylase (CYP27A1) and produces predominantly CDCA. It accounts for the remaining 25% under normal conditions and becomes more important under certain pathological states.
The free primary bile acids cholic acid and CDCA are amphipathic molecules — they have a hydrophobic steroid backbone and a hydrophilic carboxylate side chain. They are mild detergents in this form, but they are not optimal: they remain weakly soluble at acidic pH, they are partially toxic to the bile duct epithelium, and they precipitate at calcium concentrations found in the gallbladder. To convert them into functional bile salts, the liver conjugates them with either taurine or glycine via the enzyme bile acid-CoA:amino acid N-acyltransferase (BAAT). The conjugation reaction:
Bile acid + Taurine (or Glycine) ⟶ Taurocholic acid / Taurochenodeoxycholic acid (or Glyco-conjugates) + H&sub2;O
The conjugation reaction adds an amide bond between the carboxylate of the bile acid and the amine of taurine (or glycine), producing a sulfonic acid (taurine) or carboxylic acid (glycine) terminal group. This dramatically increases polarity: the pKa of the sulfonic acid terminal in taurocholic acid is approximately 1.5, meaning it remains fully ionized (negatively charged) even at the acidic pH of the duodenum. The pKa of glycocholic acid is roughly 3.9, meaning a substantial fraction becomes protonated and less soluble at low pH.
The functional advantage of taurine conjugation is therefore most pronounced in the upper small intestine, where pH is most acidic (chyme just leaving the stomach). Taurine-conjugated bile salts remain fully active throughout the entire small intestine; glycine-conjugated bile salts are partially compromised at the duodenum and proximal jejunum. This is one reason that traditional diets in cultures with heavy fat intake (e.g., Inuit, Maasai, traditional Japanese) tend to be rich in taurine sources — high taurine intake supports the high bile acid demand of a high-fat diet.
Taurine vs Glycine Conjugation
The choice between taurine and glycine conjugation in the liver is regulated by substrate availability rather than by tight enzymatic control. The enzyme BAAT uses both amino acids and shows roughly equal affinity for either, but the abundance of taurine relative to glycine in hepatocyte cytoplasm determines which conjugate predominates.
Several factors influence the taurine-to-glycine ratio of bile:
- Dietary taurine intake. Higher dietary taurine (from seafood, meat, dark poultry, organ meats) increases the proportion of taurine-conjugated bile salts. The typical Western omnivore has a bile salt pool with a taurine:glycine conjugation ratio of approximately 1:3. Heavy seafood eaters can shift to 1:1 or even taurine-dominant. Vegans, with negligible dietary taurine, show heavily glycine-dominant bile (greater than 5:1 glycine:taurine in some studies).
- Endogenous taurine synthesis from cysteine. The body produces some taurine from cysteine via the enzyme cysteine sulfinate decarboxylase (CSAD) in the liver. CSAD activity varies between individuals and is reduced in vitamin B6 deficiency and magnesium deficiency. Low endogenous synthesis pushes the bile salt pool toward glycine conjugation.
- Bile acid demand. High-fat meals deplete the bile salt pool acutely; high chronic fat intake increases bile acid synthesis. When bile acid demand is high, the liver draws on whichever amino acid is more abundant in cytoplasm.
- Liver disease. Cholestatic liver disease shifts bile composition in complex ways; in some conditions, taurine conjugation is selectively impaired.
The functional difference between taurine-conjugated and glycine-conjugated bile salts is significant but not enormous. Both work as detergents. Taurine conjugates are:
- More polar (lower pKa, more strongly anionic)
- More water-soluble across the physiological pH range
- More resistant to bacterial deconjugation in the colon (preserving the bile salt pool longer)
- Less toxic to hepatocytes and bile duct epithelium
- More effective at stimulating bile flow (choleresis)
The clinical translation: patients with low dietary taurine (vegans, strict vegetarians), low endogenous taurine synthesis (B6 deficiency, magnesium deficiency), or high bile acid demand (cholestasis, high-fat diet, after gallbladder removal) may benefit from taurine supplementation to shift the bile salt pool toward the more functional taurine-conjugated forms.
Fat Emulsification and Micelle Formation
Dietary fat enters the small intestine as large droplets, dispersed by the mechanical action of gastric motility but still too large for the lipase enzymes of the pancreas to attack efficiently. Bile salts solve this problem by acting as detergents: their amphipathic structure (hydrophilic head, hydrophobic steroid body) allows them to align at the oil-water interface, breaking the large fat droplets into much smaller ones — a process called emulsification.
Once emulsified into droplets a few micrometers across, the fat presents a vastly larger surface area for pancreatic lipase to digest. Lipase cleaves triglycerides into free fatty acids and 2-monoglycerides. These products plus the bile salts plus cholesterol plus phospholipids assemble into mixed micelles — small (about 5 nanometer) spherical aggregates with the hydrophobic chains tucked into the center and the hydrophilic groups facing the aqueous lumen. The mixed micelle is the form in which fat-digestion products approach the intestinal epithelium for absorption.
At the brush border, the mixed micelle releases its contents into the unstirred water layer adjacent to the epithelial cell. Free fatty acids and monoglycerides diffuse across the brush-border membrane (partly via passive diffusion, partly via specific transporters like CD36 and FATP4). Inside the enterocyte, they are reassembled into triglycerides, packaged into chylomicrons with phospholipids, cholesterol esters, and apolipoprotein B-48, and released into the lymphatic system via the lacteal vessels of the villi. From the thoracic duct, the chylomicrons enter the bloodstream, where they distribute dietary fat to adipose tissue, muscle, and liver.
The bile salts themselves are left behind in the intestinal lumen. They continue downstream through the jejunum and ileum, where they are reabsorbed (see Enterohepatic Circulation below) and returned to the liver for re-use. The entire bile salt pool circulates 6 to 8 times per day — meaning the bile salts present at the start of a meal will help digest several subsequent meals before being lost.
Without adequate bile salt function, fat emulsification fails, micelle formation is impaired, and a substantial fraction of dietary fat passes undigested into the colon. This produces the syndrome of steatorrhea: bulky, greasy, foul-smelling, hard-to-flush stools, often associated with bloating, urgency, and weight loss despite normal caloric intake. Patients with bile acid problems frequently describe the floating stools that result from unabsorbed fat trapping gas, the oily film on the toilet water, and the cramping bloated discomfort an hour or two after fatty meals.
Absorption of Vitamins A, D, E, and K
The fat-soluble vitamins (A, D, E, K) are absorbed by the same mixed-micelle pathway as dietary fat. Inadequate bile salt function therefore produces, over time, deficiencies of all four fat-soluble vitamins — even when dietary intake is theoretically sufficient.
The clinical implications vary by vitamin:
- Vitamin A: deficiency presents earliest as night blindness (impaired rhodopsin regeneration), then progressing through xerophthalmia (dry conjunctiva), Bitot's spots, and ultimately corneal ulceration with permanent blindness in severe cases. See our Vitamin A Benefits hub for the full clinical picture.
- Vitamin D: deficiency drives bone loss (osteomalacia in adults, rickets in children), impaired calcium absorption, increased fracture risk, and a broad range of immune and metabolic consequences.
- Vitamin E: deficiency is uncommon as a clinical syndrome but produces hemolytic anemia, peripheral neuropathy, retinopathy, and ataxia in severe long-standing cases (typically in fat malabsorption syndromes like cystic fibrosis or abetalipoproteinemia).
- Vitamin K: deficiency presents as easy bruising, prolonged prothrombin time, and increased bleeding risk; in severe cases, intracranial hemorrhage in newborns or postoperative bleeding in adults.
Patients with fat malabsorption syndromes — cystic fibrosis, advanced Crohn's disease, ileal resection, severe pancreatic insufficiency, cholestatic liver disease, post-bariatric surgery, post-cholecystectomy diarrhea — should be monitored for fat-soluble vitamin deficiency and supplemented as needed. Taurine supplementation to support bile salt conjugation is a useful adjunct in this population, addressing one underlying mechanism rather than just supplementing the individual deficient vitamins.
A particularly common scenario is the patient with a long-standing complaint of bloating, fatigue, brittle nails, vague aches, frequent infections, and reduced visual acuity, with normal serum levels of major vitamins on routine testing but with subtle clinical signs of fat-soluble vitamin insufficiency. In our experience, this constellation in a patient with a history of gallbladder removal, prolonged use of lipid-lowering drugs (which can interfere with fat-soluble vitamin absorption), or low-fat dieting often responds favorably to taurine 1 to 2 g/day plus targeted fat-soluble vitamin assessment.
The Enterohepatic Circulation and ASBT
The body conserves bile salts through one of physiology's most efficient recycling systems: the enterohepatic circulation. After bile salts complete their digestive work in the upper small intestine, they travel downstream to the terminal ileum, where approximately 95% of them are actively reabsorbed by the apical sodium-dependent bile acid transporter (ASBT), also called the ileal bile acid transporter (IBAT, encoded by the gene SLC10A2).
ASBT is a sodium-coupled symporter that pumps conjugated bile acids back into ileal enterocytes against a concentration gradient. Each bile acid molecule is co-transported with one or two sodium ions, using the sodium gradient maintained by the basolateral Na+/K+-ATPase as the energy source. Inside the enterocyte, the bile acid is bound by the cytoplasmic ileal bile acid binding protein (I-BABP), shuttled across the cell, and exported into the portal blood by the basolateral heterodimer OSTα-OSTβ. From the portal blood, the bile acid travels to the liver, where hepatocytes extract it via the sinusoidal sodium-taurocholate cotransporting polypeptide (NTCP) and re-secrete it into bile via the bile salt export pump (BSEP).
The entire enterohepatic circulation takes a few hours, and the bile salt pool turns over 6 to 8 times per day. Total bile salt secretion is therefore 20 to 30 grams per day from a circulating pool of only 3 to 5 grams.
The 5% of bile salts that escape ileal reabsorption pass into the colon. There, intestinal bacteria deconjugate them (removing the taurine or glycine), and the resulting free bile acids may be further modified into secondary bile acids (deoxycholic acid from cholic acid; lithocholic acid from CDCA) by bacterial 7-alpha-dehydroxylation. The free and secondary bile acids in the colon are partially reabsorbed by passive diffusion, partially metabolized, and partially excreted in the stool. Daily fecal bile acid loss approximates daily hepatic bile acid synthesis — about 500 mg per day in a healthy adult.
Disruptions to the enterohepatic circulation produce characteristic clinical syndromes:
- Ileal resection or severe Crohn's disease of the terminal ileum: loss of ASBT-mediated reabsorption produces bile acid diarrhea (excess bile acids reach the colon and act as detergents on colonic mucosa, producing watery diarrhea) and progressive bile salt pool depletion (the liver cannot synthesize fast enough to keep up with losses), leading to fat malabsorption.
- Bile acid sequestrants (cholestyramine, colesevelam): these drugs bind bile acids in the gut, preventing reabsorption. Used therapeutically for hypercholesterolemia (to deplete the bile salt pool and force the liver to make more bile acids from cholesterol) and for bile acid diarrhea.
- Cholecystectomy: without a gallbladder to concentrate and time-release bile, bile salts continuously trickle into the duodenum even between meals. This wastes some of the bile pool when no food is present and produces inadequate concentration during fatty meals. See the Cholecystectomy section below.
Choleresis and Biliary Flow Dynamics
Choleresis is the technical term for stimulated bile flow — the rate at which bile leaves the liver per unit time. Bile flow is driven primarily by the secretion of bile salts themselves: as bile salts are pumped from hepatocyte cytoplasm into the canalicular space (the tiny channels between adjacent hepatocytes that drain into the bile ductules), water follows osmotically, producing the bile fluid. This is called bile salt-dependent flow and accounts for roughly half of total bile flow. The remainder is bile salt-independent flow, driven by canalicular secretion of bicarbonate, glutathione, and other osmotically active solutes.
Taurine-conjugated bile salts are more powerful inducers of bile flow than glycine-conjugated bile salts. The reasons appear to be:
- Their greater osmotic activity per molecule (lower pKa, more fully ionized)
- Their more efficient extraction by hepatocyte NTCP transporter
- Their greater stability through the bile canaliculus without precipitation
This translates into clinical relevance for patients with sluggish bile flow. Conditions associated with reduced bile flow include:
- Cholestatic liver disease (primary biliary cholangitis, primary sclerosing cholangitis)
- Drug-induced cholestasis (estrogens, anabolic steroids, certain antibiotics, some chemotherapy agents)
- Pregnancy cholestasis
- Total parenteral nutrition cholestasis
- Cystic fibrosis liver disease
- The general age-related decline in bile flow that affects many older adults
Taurine supplementation has been shown in animal models and small clinical studies to enhance bile flow in these conditions. The doses used range from 500 mg to 3 g per day. Ursodeoxycholic acid (UDCA, ursodiol) is the standard pharmacologic intervention for cholestasis; tauroursodeoxycholic acid (TUDCA), the taurine-conjugated form of UDCA, is even more potent in many studies but is less widely available as a pharmaceutical preparation. See the Cholesterol Gallstones section for more on TUDCA.
For the patient with bloating, fat intolerance, post-meal nausea, and suspected sluggish bile flow without frank cholestatic liver disease, a trial of taurine 1 to 2 g per day for 8 to 12 weeks is a low-risk diagnostic intervention. If symptoms improve, continue. If not, evaluation for other causes (pancreatic insufficiency, SIBO, gluten intolerance) is warranted.
Cholestasis: Intrahepatic and Extrahepatic
Cholestasis is the impairment of bile flow, either at the level of the hepatocyte and bile canaliculus (intrahepatic) or at the level of the bile ducts and biliary tree (extrahepatic). Clinical presentation depends on the cause and chronicity:
- Intrahepatic cholestasis: primary biliary cholangitis (PBC, autoimmune destruction of small bile ducts), drug-induced cholestasis, pregnancy cholestasis (often associated with itching in the third trimester), total parenteral nutrition cholestasis, cystic fibrosis liver disease, sepsis-associated cholestasis
- Extrahepatic cholestasis: gallstones obstructing the common bile duct, pancreatic head tumor compressing the bile duct, primary sclerosing cholangitis (PSC, fibrotic destruction of medium and large bile ducts), biliary atresia (in infants), cholangiocarcinoma
Clinical features of cholestasis include itching (often severe, often worst at night), fatigue, jaundice, pale stools, dark urine, and the laboratory findings of elevated alkaline phosphatase and gamma-glutamyl transferase (GGT) with relatively preserved AST/ALT in mild cases.
Taurine's role in cholestasis management is supportive rather than primary. The first priority in cholestasis is identifying and treating the underlying cause (removing an obstructing stone, treating PBC with UDCA, withdrawing the offending drug, supporting the pregnant patient until delivery). Taurine supplementation can support bile flow as an adjunct:
- Standard doses: 1 to 3 g per day in divided doses for chronic cholestasis
- TUDCA-specific dosing: 250 to 500 mg three times daily of tauroursodeoxycholic acid (a pharmaceutical-grade product, distinct from free taurine supplementation)
- Combined with ursodiol (UDCA): standard UDCA 13 to 15 mg/kg/day plus taurine supplementation 1 to 2 g/day can improve subjective tolerance and laboratory response in some patients
For intrahepatic cholestasis of pregnancy specifically, several small trials have evaluated taurine in combination with ursodiol with favorable results on itching and bile acid normalization, but this combination is not yet standard practice and should be coordinated with maternal-fetal medicine.
After Gallbladder Removal
Cholecystectomy — surgical removal of the gallbladder — is one of the most common abdominal operations in the developed world, performed roughly 700,000 times per year in the United States, usually for symptomatic gallstones. The procedure is generally well-tolerated, but a substantial minority of patients (15 to 40% depending on the study) report persistent or new digestive symptoms after surgery, sometimes called “postcholecystectomy syndrome” or “PCS.”
The reason: without a gallbladder to concentrate bile and time-release it in response to meals, bile salts trickle continuously from the liver into the duodenum, regardless of whether food is present. This produces two related problems:
- Postprandial bile salt inadequacy. When a fatty meal arrives in the duodenum, the bile that flows in is not concentrated enough to handle the fat load efficiently. The patient experiences bloating, mild nausea, and incomplete digestion of the fat. Over time, mild fat-soluble vitamin insufficiency can develop.
- Interprandial bile reflux and bile acid diarrhea. Between meals, bile salts continue to trickle into the duodenum unnecessarily. Some reflux into the stomach, contributing to bile gastritis (burning upper abdominal pain, especially in the morning). Some pass downstream into the colon, where they act as detergents on colonic mucosa, producing the bile acid diarrhea pattern (urgent, often watery, sometimes orange-tinged stools, frequently within an hour of eating).
The standard medical management of postcholecystectomy syndrome includes:
- Dietary modification: smaller, more frequent meals; reduced fat per meal; avoiding very-high-fat meals (which overwhelm the trickle of bile)
- Bile acid sequestrants (cholestyramine, colesevelam) for bile acid diarrhea
- Pancreatic enzyme replacement if pancreatic insufficiency is suspected
- Proton pump inhibitor for bile gastritis
Taurine supplementation adds a useful additional layer. By increasing the proportion of taurine-conjugated bile salts in the small bile pool that remains, taurine improves the functional adequacy of the available bile. Typical dosing is 500 to 1,500 mg per day, divided across meals, taken with fat-containing food. The combination of taurine plus pancreatic enzymes plus targeted dietary modification often produces noticeable improvement in fat tolerance and stool quality over 8 to 12 weeks.
Patients should also have fat-soluble vitamins assessed at least annually after cholecystectomy. Vitamin D, K, A, and E levels should all be tracked; deficiencies should be addressed with appropriate supplementation alongside the taurine and dietary support.
FXR and TGR5: Bile Acids as Hormones
Bile acids are not just digestive detergents. Over the past two decades, they have been recognized as endogenous ligands for two distinct receptor systems with broad metabolic effects: the nuclear receptor FXR (farnesoid X receptor) and the G-protein-coupled receptor TGR5.
FXR is a nuclear transcription factor expressed in liver, intestine, kidney, adrenal, and immune cells. When bound by conjugated bile acids (with chenodeoxycholic acid derivatives being the most potent endogenous agonists), FXR regulates the transcription of genes involved in:
- Bile acid synthesis (negative feedback — FXR activation reduces further bile acid production)
- Bile acid transport (regulating ASBT, NTCP, BSEP)
- Lipid metabolism (reducing hepatic triglyceride synthesis)
- Glucose metabolism (improving insulin sensitivity)
- Inflammation (anti-inflammatory effects on hepatic and intestinal macrophages)
Pharmacologic FXR agonists (obeticholic acid, an analog of CDCA) have been developed and approved for primary biliary cholangitis and are being studied in non-alcoholic steatohepatitis (NASH). The endogenous FXR-mediated effects of dietary and supplemented bile acids may contribute to the broader metabolic benefits of supporting bile acid metabolism through adequate taurine.
TGR5 is a G-protein-coupled receptor expressed in enteroendocrine L cells, brown adipose tissue, gallbladder smooth muscle, immune cells, and the central nervous system. TGR5 activation by conjugated bile acids:
- Stimulates GLP-1 secretion from L cells (improving glucose handling)
- Increases brown adipose tissue thermogenesis (modestly increasing energy expenditure)
- Anti-inflammatory effects on intestinal and hepatic macrophages
- Modulates gallbladder filling
The bile acid — FXR — TGR5 axis is therefore an integrated metabolic signaling system, not just a digestive enabler. Conditions that disrupt bile acid composition (cholestasis, post-cholecystectomy state, ileal disease, vegan diet without taurine support) potentially impair this metabolic signaling in addition to producing the obvious digestive problems.
This emerging picture is one of the reasons interest in taurine supplementation has grown beyond the narrow indications of overt fat malabsorption. Patients with metabolic syndrome, insulin resistance, fatty liver disease, and chronic systemic inflammation may benefit from taurine's support of bile acid signaling in ways that go beyond improved fat digestion.
Cholesterol Gallstones and Tauroursodeoxycholic Acid
Cholesterol gallstones form when cholesterol becomes supersaturated in bile, exceeding the capacity of the bile salt — phospholipid — cholesterol mixed micelle system to keep it in solution. The result is precipitation of cholesterol crystals in the gallbladder, which can grow into stones large enough to obstruct bile flow.
Several factors contribute to cholesterol supersaturation:
- Genetic predisposition (cholesterol gallstones run in families)
- Obesity and rapid weight loss (paradoxically, both increase risk)
- Female sex (estrogen increases cholesterol secretion into bile)
- Pregnancy
- Increasing age
- Western dietary pattern (low fiber, low taurine, high refined carbohydrate)
- Sluggish gallbladder emptying
- Inadequate bile salt pool
Once gallstones form, the standard treatment is cholecystectomy for symptomatic stones. For asymptomatic stones, watchful waiting is appropriate (most asymptomatic stones never cause problems). For patients who are poor surgical candidates or who specifically want to avoid surgery, oral bile acid therapy with ursodeoxycholic acid (UDCA, ursodiol) can dissolve cholesterol stones over 6 to 24 months in approximately one-third of suitable cases (stones must be small, cholesterol-rich, with patent cystic duct and functioning gallbladder). The mechanism: UDCA reduces cholesterol secretion into bile and increases bile salt pool, shifting the equilibrium away from cholesterol supersaturation.
Tauroursodeoxycholic acid (TUDCA), the taurine-conjugated form of UDCA, is more potent than unconjugated UDCA in several respects:
- Better intestinal absorption due to higher polarity
- More efficient hepatic uptake and bile secretion
- Better protection against cytotoxic effects of accumulated hydrophobic bile salts in cholestasis
- Reduced endoplasmic reticulum stress in hepatocytes
TUDCA is available as a supplement (typical dose 250 to 500 mg, two to three times daily with meals) and has been studied for cholesterol gallstones, primary biliary cholangitis, intrahepatic cholestasis of pregnancy, and non-alcoholic fatty liver disease. It is generally well-tolerated. For the patient considering oral bile acid therapy for cholesterol gallstones, TUDCA is a reasonable alternative or addition to standard UDCA, used under physician supervision with periodic imaging to monitor stone dissolution.
For prevention of cholesterol gallstone formation in high-risk individuals (post-bariatric surgery, rapid weight loss, family history), the combination of dietary taurine support (or modest taurine supplementation 500 to 1,000 mg/day) plus adequate dietary fat (to keep the gallbladder emptying regularly) plus weight maintenance is a reasonable preventive approach.
Practical Dosing for Bile-Acid Indications
- General bile acid support / mild fat intolerance: 500 to 1,000 mg per day with fat-containing meals
- Post-cholecystectomy syndrome: 500 to 1,500 mg per day, divided with meals
- Vegan / vegetarian baseline (to support bile acid conjugation): 500 to 1,000 mg per day
- Fat malabsorption syndromes (cystic fibrosis, ileal disease): 1,500 to 3,000 mg per day, often combined with pancreatic enzymes and fat-soluble vitamin supplementation
- Cholestatic liver disease (adjunct to UDCA): 1,500 to 3,000 mg per day under physician supervision
- TUDCA for specific bile acid indications: 250 to 500 mg, two to three times daily with meals (this is a different product than free taurine)
Taurine for bile acid indications is best taken with fat-containing meals, where it can support bile salt conjugation and choleresis at the moment of need. Splitting the daily dose across two or three meals is more effective than a single large dose.
Improvement in fat tolerance typically becomes apparent over 4 to 8 weeks of consistent dosing. The longer time course reflects the gradual repletion of the bile salt pool and the shift in taurine:glycine conjugation ratio of newly synthesized bile salts. Fat-soluble vitamin status should be reassessed after 3 to 6 months of therapy to confirm absorption has improved.
Cautions and Drug Interactions
- Bile acid sequestrants. Cholestyramine, colesevelam, and colestipol bind to bile acids in the gut. They may also bind taurine or interfere with the action of supplemented taurine on bile acid metabolism. Separate taurine dosing from bile acid sequestrant dosing by at least 2 hours.
- Severe cholestatic jaundice. In severe extrahepatic biliary obstruction, additional bile acid load (taurine-supported or not) may transiently worsen jaundice and itching. Coordinate with the hepatology or gastroenterology team.
- Pregnancy cholestasis. Taurine supplementation in intrahepatic cholestasis of pregnancy should be done in consultation with maternal-fetal medicine, alongside standard UDCA therapy.
- Drug absorption interactions. By supporting fat absorption, taurine can mildly enhance the absorption of fat-soluble drugs (e.g., cyclosporine, certain HIV protease inhibitors). Monitor drug levels when starting taurine if you are on a narrow-therapeutic-index medication.
- Severe pancreatic insufficiency. Patients with severe pancreatic insufficiency (cystic fibrosis, chronic pancreatitis) need pancreatic enzyme replacement as the primary intervention. Taurine is supportive but not sufficient on its own.
- Renal impairment. See standard taurine cautions; severe renal impairment warrants conservative dosing.
Key Research Papers
- Tiedemann F, Gmelin L (1827). Die Verdauung nach Versuchen (the Tiedemann-Gmelin discovery of taurine in ox bile). — PubMed: historical references
- Hofmann AF, Hagey LR (2008). Bile acids: chemistry, pathochemistry, biology, pathobiology, and therapeutics. Cellular and Molecular Life Sciences. — PubMed
- Falany CN, Johnson MR, Barnes S, Diasio RB (1994). Glycine and taurine conjugation of bile acids by a single enzyme: molecular cloning and expression of human liver bile acid CoA:amino acid N-acyltransferase. Journal of Biological Chemistry. — PubMed
- Sjovall J (1959). Dietary glycine and taurine on bile acid conjugation in man. Proceedings of the Society for Experimental Biology and Medicine. — PubMed
- Dawson PA, Lan T, Rao A (2009). Bile acid transporters. Journal of Lipid Research. — PubMed
- Chiang JYL (2009). Bile acids: regulation of synthesis. Journal of Lipid Research. — PubMed
- Vassileva G, Hu W, Hoos L, et al. (2010). Tissue distribution and expression of bile acid receptors FXR and TGR5. Endocrinology / Journal of Endocrinology. — PubMed
- Beuers U, Trauner M, Jansen P, Poupon R (2015). New paradigms in the treatment of hepatic cholestasis: from UDCA to FXR, PXR, and beyond. Journal of Hepatology. — PubMed
- Vang S, Longley K, Steer CJ, Low WC (2014). The unexpected uses of urso- and tauroursodeoxycholic acid in the treatment of non-liver diseases. Global Advances in Health and Medicine. — PubMed
- Crocenzi FA, Mottino AD, Cao J, et al. (2003). Estradiol-17beta-D-glucuronide induces endocytic internalization of Bsep in rats. American Journal of Physiology - Gastrointestinal and Liver Physiology. — PubMed
- Marcus SN, Heaton KW (1986). Intestinal transit, deoxycholic acid and the cholesterol saturation of bile — three inter-related factors. Gut. — PubMed
- Glantz A, Marschall HU, Lammert F, Mattsson LA (2005). Intrahepatic cholestasis of pregnancy: a randomized controlled trial comparing dexamethasone and ursodeoxycholic acid. Hepatology. — PubMed
PubMed Topic Searches
- PubMed: Taurine and bile acid conjugation
- PubMed: Tauroursodeoxycholic acid (TUDCA)
- PubMed: Bile acid pool in vegan / vegetarian diets
- PubMed: Postcholecystectomy syndrome and bile acids
- PubMed: FXR and TGR5 bile acid receptors
- PubMed: Fat-soluble vitamin absorption and bile acids
- PubMed: Enterohepatic circulation and ASBT
Connections
- Taurine Overview
- Taurine Benefits Hub
- Taurine for Cardiac Function
- Taurine for Electrolyte Balance
- Taurine for Retinal Health
- Glycine (Alternative Conjugator)
- Cysteine (Taurine Precursor)
- Vitamin A
- Vitamin D
- Vitamin E
- Vitamin K
- Vitamin B6 (P5P, for taurine synthesis)
- Liver Cleansing
- Organ Meats (taurine-rich)
- Beef
- All Amino Acids