D-Serine and NMDA Receptor Co-Agonism
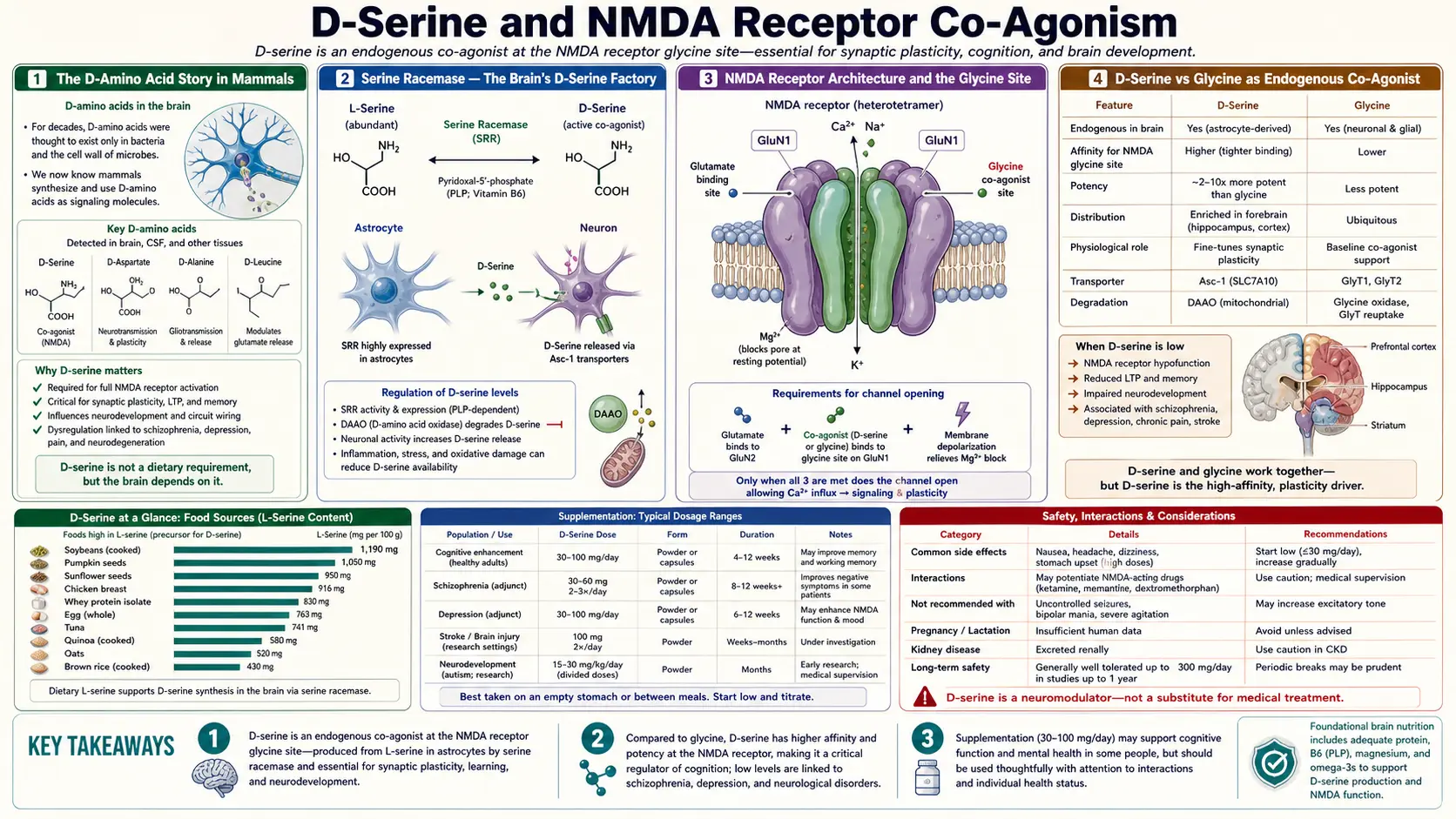
For most of the twentieth century, biochemists taught that mammalian proteins use only L-amino acids and that D-amino acids exist only in bacterial cell walls. That view was wrong. D-serine, the dextrorotary enantiomer of the otherwise familiar serine molecule, is synthesized in mammalian brain by an enzyme called serine racemase, is present in glutamatergic synapses at concentrations of tens of micromolar, and serves as the principal endogenous co-agonist at the glycine-binding site of the NMDA glutamate receptor. The NMDA receptor cannot open in response to glutamate alone — co-binding of either glycine or D-serine to the GluN1 subunit is required. This molecular discovery, made between 1992 and 2000, has transformed the understanding of synaptic plasticity, the genetics of schizophrenia, the pathobiology of ALS, and the search for antipsychotic drugs that work differently from the four-decade-old dopamine D2 antagonist class.
Table of Contents
- The D-Amino Acid Story in Mammals
- Serine Racemase — The Brain's D-Serine Factory
- NMDA Receptor Architecture and the Glycine Site
- D-Serine vs Glycine as Endogenous Co-Agonist
- D-Serine in Schizophrenia — Tsai 1998 and Heresco-Levy 2005
- Sarcosine, D-Amino Acid Oxidase, and the Therapeutic Pipeline
- Parkinson's Disease and Alzheimer's Disease
- ALS — The Sasabe 2007 Finding
- Cognitive Aging and Memory
- Dosing, Sources, and Cautions
- Key Research Papers
- Connections
- Featured Videos
The D-Amino Acid Story in Mammals
For decades, biochemistry textbooks taught that proteins are built exclusively from the twenty L-amino acids, and that free D-amino acids in mammals are vanishingly rare — trace contaminants from gut bacteria at most. D-amino acids were assumed to belong to the bacterial world, where they are conspicuous components of peptidoglycan cell walls (D-alanine, D-glutamate) and of bacterial signaling peptides.
That worldview began to crack in the 1980s. Hashimoto and colleagues at Saitama Medical School in Japan, using newly developed chiral HPLC methods, reported in 1992 that D-serine is present in rat brain at concentrations comparable to L-serine in some regions and at micromolar levels overall. Subsequent work showed that D-serine concentration was highest in forebrain regions enriched in NMDA glutamate receptors — cortex, hippocampus, striatum — and lowest in cerebellum and brainstem. The distribution did not match dietary sources or bacterial contamination; D-serine was endogenously synthesized.
The enzyme responsible was identified in 1999 by the Snyder laboratory at Johns Hopkins. Serine racemase (SRR) converts L-serine to D-serine in a pyridoxal-5'-phosphate-dependent reaction. The enzyme is enriched in the same forebrain regions where D-serine accumulates, and is expressed predominantly in glutamatergic neurons (a 2005 finding that overturned an initial assumption that astrocytes were the source). Subsequent work has established that D-serine is the principal endogenous co-agonist at synaptic NMDA receptors in the forebrain, while glycine plays the equivalent role at extrasynaptic NMDA receptors and at NMDA receptors in the spinal cord and brainstem.
The discovery of mammalian D-serine biology was unexpected enough that it took roughly a decade for the field to incorporate it. The textbook claim that "mammals use only L-amino acids" survived in updated form — D-serine and a smaller amount of D-aspartate are now recognized as the exceptions, and the assertion is correct that no D-amino acids are incorporated into mammalian proteins. But the free D-amino acid pool in the brain is a real, regulated, functionally important system.
Serine Racemase — The Brain's D-Serine Factory
Serine racemase (SRR, encoded by the SRR gene on human chromosome 17p13) is a 36-kDa pyridoxal-5'-phosphate-dependent enzyme that catalyzes two reactions:
- Racemization — L-serine ⇌ D-serine. This is the canonical reaction and the source of brain D-serine.
- α,β-elimination — L-serine or D-serine → pyruvate + ammonia. This is a side reaction that degrades serine.
The two reactions are catalyzed at the same active site, and the partitioning between racemization and elimination is regulated by cofactors. ATP and Mg2+ favor racemization, while glycine and other modulators shift toward elimination. The result is a tightly regulated supply of D-serine to the extracellular synaptic space, where it can engage NMDA receptors.
The cellular expression of serine racemase has been a point of revision. Initially (Snyder 1999), SRR was reported as astrocyte-localized. By 2005-2010, a series of careful studies (Wolosker, Coyle, others) using cell-specific markers and conditional knockout mice showed that SRR is in fact expressed predominantly in glutamatergic neurons, not astrocytes. The corrected model is that neurons synthesize D-serine intracellularly and release it through volume-regulated anion channels or by serine-driven export mechanisms in response to neuronal activity, producing tonic and phasic D-serine signaling at synapses.
D-serine breakdown is catalyzed by D-amino acid oxidase (DAO/DAAO), a flavin-adenine-dinucleotide-dependent enzyme that oxidizes D-serine to the corresponding α-keto acid and hydrogen peroxide. DAO is highly expressed in cerebellum and brainstem (regions with low D-serine), and at much lower levels in cortex and hippocampus. This complementary distribution — SRR high where DAO is low — explains the regional D-serine concentration map and is the source of considerable therapeutic interest, as DAO inhibitors would raise synaptic D-serine.
NMDA Receptor Architecture and the Glycine Site
The NMDA glutamate receptor is a heterotetrameric ion channel composed of two obligatory GluN1 subunits and two regulatory subunits drawn from the GluN2A, GluN2B, GluN2C, GluN2D, GluN3A, or GluN3B families. Each subunit has a large amino-terminal domain, a ligand-binding domain (LBD), three transmembrane domains, and a C-terminal cytoplasmic tail.
The critical architectural feature for understanding D-serine is that the NMDA receptor has two agonist binding sites:
- The glutamate-binding site on the GluN2 subunit — binds glutamate released into the synapse by the presynaptic terminal during normal excitatory neurotransmission.
- The glycine/D-serine binding site on the GluN1 subunit — binds either glycine or D-serine, both of which serve as co-agonists.
Both sites must be occupied simultaneously for the channel to open and allow the characteristic sodium, potassium, and calcium currents that distinguish NMDA receptors from other glutamate receptors. Glutamate alone produces no response. This dual-agonist requirement makes the NMDA receptor a coincidence detector — it opens only when presynaptic glutamate release coincides with adequate co-agonist availability, which provides a regulatory layer absent from other glutamate receptors.
The receptor also requires postsynaptic depolarization to release a magnesium ion that blocks the channel at resting membrane potential. The combination of these three requirements — glutamate, co-agonist, depolarization — means that NMDA receptors only conduct when a postsynaptic neuron is already partially excited and the synapse is actively firing. This is the molecular basis for Hebbian "neurons that fire together wire together" synaptic plasticity, and underlies long-term potentiation (LTP), the cellular correlate of learning.
The co-agonist binding site was discovered in 1987 by Johnson and Ascher, who reported that glycine at submicromolar concentrations was required for NMDA receptor activity. For roughly a decade, glycine was assumed to be the sole endogenous co-agonist. The 1990s-2000s revision of that view — D-serine is the dominant synaptic co-agonist in forebrain — rewrote a substantial fraction of NMDA receptor pharmacology.
D-Serine vs Glycine as Endogenous Co-Agonist
Both D-serine and glycine bind the same site on the GluN1 subunit with similar affinity (low micromolar for both). The current understanding of why both exist and how their roles differ:
- Synaptic vs extrasynaptic — in the forebrain (cortex, hippocampus, striatum), D-serine is the dominant co-agonist at synaptic NMDA receptors, while glycine dominates at extrasynaptic NMDA receptors. The molecular basis of this distinction relates to the distribution of glycine transporters (GlyT1, expressed on astrocytes around the synapse) that keep synaptic glycine low.
- Subunit composition — D-serine has slightly higher relative potency at GluN2A-containing receptors (mature, synaptic), while glycine is relatively more potent at GluN2B-containing receptors (developmental, extrasynaptic, perisynaptic).
- Regional — D-serine signaling dominates in forebrain; glycine signaling dominates in cerebellum, brainstem, and spinal cord. This matches the regional expression of serine racemase (forebrain-enriched) and DAO (hindbrain-enriched).
- Developmental — glycine is the dominant co-agonist during early development, while D-serine takes over progressively during postnatal maturation as serine racemase expression rises.
The clinical implication is that interventions targeting "the NMDA co-agonist site" need to be regionally and functionally precise. Raising whole-body glycine with an oral glycine supplement primarily increases extrasynaptic NMDA tone in spinal cord and brainstem (which is part of why glycine has the well-established sleep-promoting and muscle-relaxant effects). Raising D-serine, either directly via supplementation or indirectly via DAO inhibition, has more selective effects on forebrain synaptic NMDA receptors and the cognitive functions that depend on them.
D-Serine in Schizophrenia — Tsai 1998 and Heresco-Levy 2005
The clinical relevance of the NMDA co-agonist site was sharpened by a long-standing pharmacological observation: NMDA receptor antagonists such as phencyclidine (PCP) and ketamine produce a schizophrenia-like psychosis in healthy volunteers and exacerbate symptoms in patients with established schizophrenia. The NMDA hypofunction hypothesis of schizophrenia proposed that the disorder reflects reduced NMDA receptor signaling, and that boosting that signaling (via the glycine/D-serine site, which is safer than direct glutamate-site agonism that causes excitotoxicity) could produce antipsychotic effects.
Tsai et al. 1998, Biological Psychiatry. The first randomized, double-blind, placebo-controlled trial of D-serine in schizophrenia. Twenty-nine patients with chronic schizophrenia on stable antipsychotic medication received D-serine 30 mg/kg per day (roughly 2 grams for a 70-kg adult) for 6 weeks. Results:
- Significant improvement in negative symptoms (apathy, social withdrawal, anhedonia — the symptoms that conventional D2-antagonist antipsychotics treat least well)
- Significant improvement in cognitive function on the Wisconsin Card Sorting Test (a measure of executive function and cognitive flexibility)
- No worsening of positive symptoms; modest improvement on the positive symptom subscale
- Excellent safety profile — no acute toxicity, no neuroleptic-malignant-syndrome signal
Heresco-Levy et al. 2005, Biological Psychiatry. Confirmation trial using higher-dose D-serine (60 mg/kg per day, roughly 4 grams in a 70-kg adult) in 39 patients with chronic schizophrenia receiving conventional antipsychotic medication. Six weeks of treatment produced significant improvement on the positive, negative, and cognitive symptom subscales of the Positive and Negative Syndrome Scale (PANSS), with negative-symptom and cognitive improvement most pronounced. Replicated the Tsai 1998 finding at higher dose.
The two trials, together with several smaller replication studies, established D-serine as a proof-of-concept that the NMDA co-agonist site is a therapeutic target in schizophrenia. They did not, however, immediately produce a marketed antipsychotic drug. The reasons are practical: D-serine is a free amino acid with limited brain penetration (the BBB transports it but inefficiently), and the doses required (2-4 grams) approach the upper end of acceptable oral amino acid loads. Subsequent pharmaceutical development has focused on alternative approaches: DAO inhibitors that raise endogenous D-serine, glycine transporter 1 (GlyT1) inhibitors that raise synaptic glycine (bitopertin was the most advanced of these and reached Phase III before failing on the primary endpoint), and direct prodrugs of D-serine with better brain penetration.
For more on the broader schizophrenia treatment landscape, see our Schizophrenia page.
Sarcosine, D-Amino Acid Oxidase, and the Therapeutic Pipeline
The D-serine schizophrenia signal opened up an entire pharmacological research program. The principal targets and their lead compounds:
- Glycine itself — high-dose oral glycine (30-60 grams/day) was studied in the late 1990s in schizophrenia with modestly positive results. The doses required are at the limit of palatability and produce significant GI side effects.
- Sarcosine (N-methylglycine) — a glycine transporter (GlyT1) inhibitor that raises synaptic glycine. Sarcosine at 2 g/day has shown benefit in randomized trials in schizophrenia (Tsai 2004, Lane 2006, Lane 2013), particularly for negative symptoms and cognition. Sarcosine is available as a dietary supplement and is used by some integrative psychiatrists as an adjunct to conventional antipsychotic medication.
- Bitopertin (RG1678) — Roche's high-affinity GlyT1 inhibitor. Phase II results were promising, but the Phase III SearchLyte program failed in 2014-2015, dampening enthusiasm for this approach.
- D-amino acid oxidase (DAO) inhibitors — small molecules that block DAO and raise endogenous D-serine. Sodium benzoate (a generic and inexpensive food preservative that happens to be a weak DAO inhibitor) showed positive results in a 2013 trial in chronic schizophrenia (Lane et al., JAMA Psychiatry) at 1 g/day. SP-624 and other selective DAO inhibitors are in clinical development.
- Direct D-serine prodrugs — modified forms of D-serine with improved BBB penetration are in preclinical development.
The active research and the FDA approval of pimavanserin (a serotonin 5HT2A inverse agonist) for Parkinson's psychosis — an antipsychotic with no dopaminergic activity at all — reflect the broader shift away from the D2-antagonist paradigm that dominated antipsychotic pharmacology from the 1950s through the 2000s. NMDA co-agonist site interventions are one of the principal alternative strategies.
Parkinson's Disease and Alzheimer's Disease
D-serine and the NMDA co-agonist system have been investigated in other neurological conditions:
Parkinson's disease. NMDA receptor signaling in the basal ganglia contributes both to normal motor control and to the dyskinesias that develop in advanced PD on long-term levodopa therapy. D-serine cerebrospinal fluid levels have been reported as reduced in PD patients in some studies, raising the possibility that D-serine deficiency contributes to the cognitive impairment and dementia that develop in many PD patients. A small open-label trial of D-serine 30 mg/kg in PD with cognitive impairment reported improvements on cognitive endpoints, but no large randomized trials have been completed.
Alzheimer's disease. The relationship between NMDA signaling and Alzheimer's is complex. Excessive NMDA signaling contributes to amyloid-beta-mediated synapse loss and excitotoxicity (the rationale for memantine, an NMDA receptor antagonist approved for moderate-to-severe Alzheimer's). At the same time, reduced synaptic NMDA tone with preserved extrasynaptic NMDA activity may contribute to cognitive decline. D-serine CSF levels have been reported as altered in AD, but whether they are increased or decreased depends on the study and on disease stage. The therapeutic implications are not clear, and direct D-serine supplementation is not currently recommended for Alzheimer's disease.
ALS — The Sasabe 2007 Finding
Amyotrophic lateral sclerosis (ALS), the progressive motor neuron disease known as Lou Gehrig's disease, has a glutamate-excitotoxicity component — riluzole, the first ALS-modifying drug, works in part by reducing glutamate release. The D-serine connection emerged through a striking finding in 2007.
Sasabe et al. 2007, EMBO Journal. The Sasabe group reported that D-serine accumulates dramatically in the spinal cord of ALS patients and in mutant SOD1 mouse models of ALS, in parallel with motor neuron loss. The accumulation appears to be driven by reduced DAO activity (and in some cases by DAO mutations) plus inflammation-driven serine racemase induction in astrocytes around dying motor neurons. The excess D-serine then drives NMDA-mediated excitotoxicity on the remaining motor neurons, accelerating their death.
This was a paradigm shift in two ways. First, it identified D-serine as a pathological agent in a major neurodegenerative disease (in contrast to schizophrenia, where the issue is too little D-serine signaling). Second, it suggested that DAO activation, rather than DAO inhibition, might be the therapeutic strategy for ALS.
Subsequent work has confirmed the D-serine accumulation in ALS spinal cord and the contribution of excess D-serine signaling to motor neuron death. Some ALS patients carry rare DAO loss-of-function mutations that segregate with disease, supporting causality. Drug development for DAO activators (the opposite of the schizophrenia approach) is at an early stage, and no ALS-modifying drug currently targets this pathway clinically. But the finding established that the D-serine system has bidirectional therapeutic relevance — too little is bad for schizophrenia, too much is bad for motor neuron survival.
The clinical practical implication: D-serine supplementation should not be undertaken by ALS patients, and the broader use of high-dose L-serine in ALS (which has been popularized by certain alternative-medicine practitioners based on a hypothesis about cyanobacterial BMAA toxicity) should be approached cautiously given the spinal-cord D-serine accumulation findings. For more on ALS, see our ALS page.
Cognitive Aging and Memory
Beyond the specific psychiatric and neurodegenerative applications, the D-serine system has been implicated in normal cognitive aging. NMDA receptor function declines with age, and reduced synaptic D-serine availability may contribute to that decline. Small trials of D-serine supplementation in older adults (typically 2-4 g/day) have reported modest improvements on episodic memory tasks and on tests of cognitive flexibility, though the literature is sparse and the trials have been small.
The mechanism would parallel the schizophrenia rationale: restoring NMDA co-agonist tone supports the synaptic plasticity that underlies new memory formation. There is preliminary evidence from animal studies that chronic D-serine supplementation can reverse age-related decline in long-term potentiation in the hippocampus.
The practical takeaway for most older adults is conservative: ensure adequate dietary L-serine (the substrate for endogenous D-serine synthesis), consider L-serine supplementation at 2-5 g/day in those with cognitive complaints (the L-form is much better characterized for safety than D-serine), and reserve D-serine itself for specific clinical indications under medical guidance.
Dosing, Sources, and Cautions
L-serine supplementation (the substrate for endogenous D-serine synthesis):
- 2 to 5 grams per day, divided, is the typical dose for cognitive support
- Well-tolerated and broadly available as a dietary supplement
- Crosses the blood-brain barrier and supports astrocyte D-serine synthesis
D-serine direct supplementation:
- Used in research trials at 30 to 60 mg/kg per day (2 to 4 g for a 70-kg adult)
- Available from a small number of specialty supplement vendors but should be used only under professional guidance
- Contraindicated in ALS based on the Sasabe et al. spinal cord findings; caution in any setting where NMDA-mediated excitotoxicity may be active
- Renal function should be monitored at high doses; high-dose D-serine has produced nephrotoxicity in rodent studies, mediated by DAO-generated hydrogen peroxide in the renal tubule. This has not been a clinically prominent issue at the doses used in schizophrenia trials, but underscores the need for medical oversight.
Indirect approaches — raising endogenous D-serine through DAO inhibition (sodium benzoate 1 g/day has the most clinical evidence) or through glycine transporter inhibition (sarcosine 2 g/day) may be preferable to direct D-serine for some indications. These should be undertaken with psychiatric or neurological supervision.
Key Research Papers
- Hashimoto A et al. (1992). The presence of free D-serine in rat brain. FEBS Letters. — PubMed
- Wolosker H, Blackshaw S, Snyder SH (1999). Serine racemase: a glial enzyme synthesizing D-serine to regulate glutamate-N-methyl-D-aspartate neurotransmission. PNAS. — PubMed
- Tsai G et al. (1998). D-serine added to antipsychotics for the treatment of schizophrenia. Biological Psychiatry. — PubMed
- Heresco-Levy U et al. (2005). D-serine efficacy as add-on pharmacotherapy to risperidone and olanzapine for treatment-refractory schizophrenia. Biological Psychiatry. — PubMed
- Sasabe J et al. (2007). D-serine is a key determinant of glutamate toxicity in amyotrophic lateral sclerosis. EMBO Journal. — PubMed
- Mothet JP et al. (2000). D-serine is an endogenous ligand for the glycine site of the N-methyl-D-aspartate receptor. PNAS. — PubMed
- Lane HY et al. (2013). Add-on treatment of benzoate for schizophrenia: a randomized, double-blind, placebo-controlled trial of D-amino acid oxidase inhibitor. JAMA Psychiatry. — PubMed
- Tsai G, Lane HY, Yang P, Chong MY, Lange N (2004). Glycine transporter I inhibitor, N-methylglycine (sarcosine), added to antipsychotics for the treatment of schizophrenia. Biological Psychiatry. — PubMed
- Johnson JW, Ascher P (1987). Glycine potentiates the NMDA response in cultured mouse brain neurons. Nature. — PubMed
- Wolosker H et al. (2008). D-amino acids in the brain: D-serine in neurotransmission and neurodegeneration. FEBS Journal. — PubMed
- Coyle JT, Balu DT (2018). The role of serine racemase in the pathophysiology of brain disorders. Advances in Pharmacology. — PubMed
- Mitchell J et al. (2010). Familial amyotrophic lateral sclerosis is associated with a mutation in D-amino acid oxidase. PNAS. — PubMed
PubMed Topic Searches
- PubMed: D-serine and NMDA co-agonism
- PubMed: D-serine in schizophrenia
- PubMed: Serine racemase enzyme
- PubMed: D-amino acid oxidase
- PubMed: Sarcosine / GlyT1 inhibition
Connections
- Serine Overview
- Serine Benefits Hub
- Phosphatidylserine and Brain
- Glycine Source (SHMT)
- Sphingolipid Synthesis (SPT)
- Glycine
- Glutamic Acid
- Schizophrenia
- ALS
- Parkinson's Disease
- Alzheimer's Disease
- Vitamin B6 (Pyridoxal Phosphate)
- Magnesium (NMDA Channel Block)
- NAC & Glutathione
- All Amino Acids