Lysine for Herpes Prevention
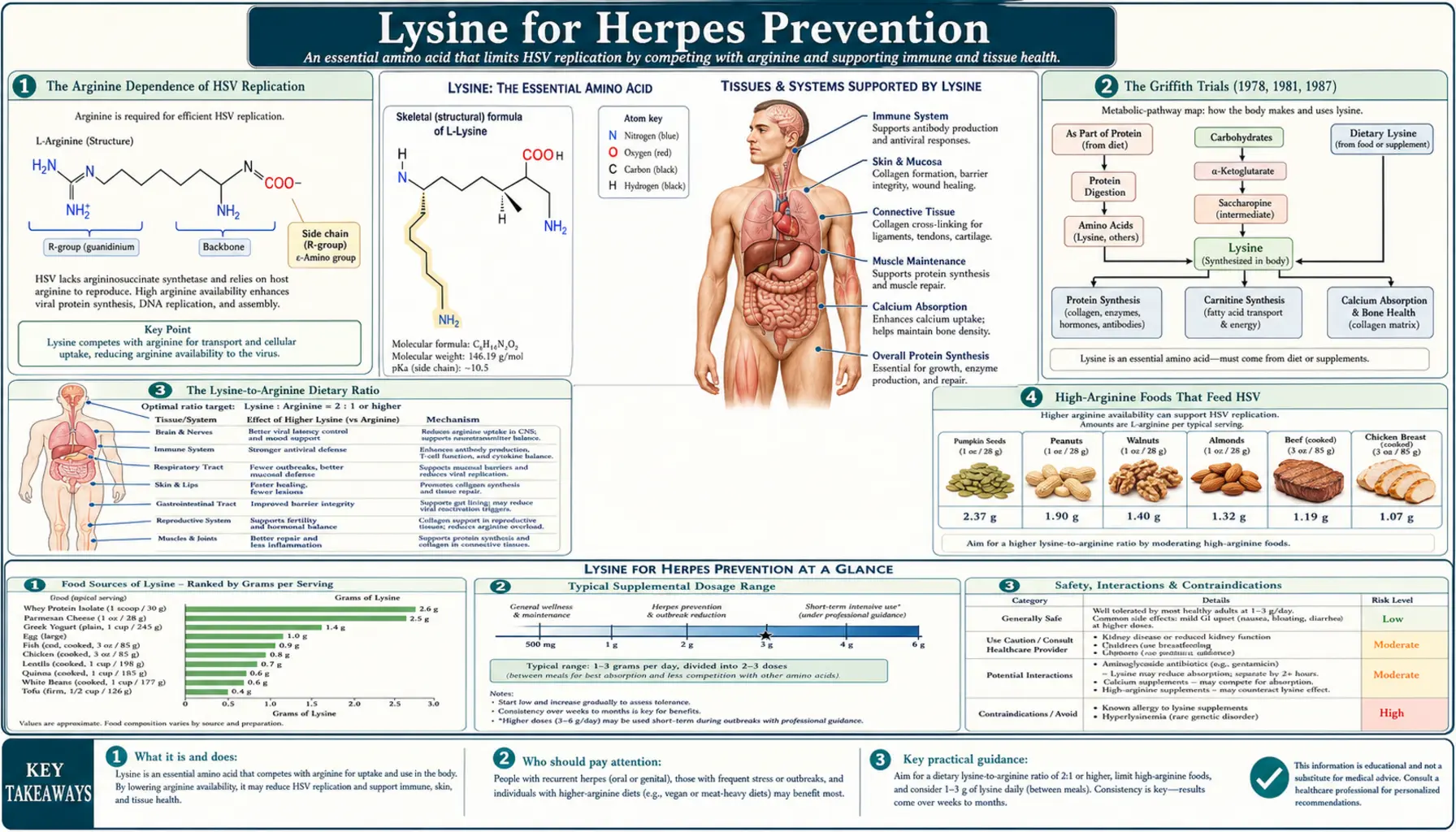
The single best-known clinical use of lysine is the prophylactic and suppressive treatment of herpes simplex virus (HSV-1 cold sores and HSV-2 genital herpes). The mechanism is mechanistic and elegant: HSV replication is arginine-dependent, lysine and arginine compete for the same intestinal and cellular transport systems, and tilting that ratio toward lysine starves the virus of its preferred substrate. Christopher Kagan, Richard Griffith, and colleagues established the foundation in a series of papers between 1978 and 1987. The clinical evidence is mixed in quality but converges on a meaningful effect at 1,000-3,000 mg/day for prophylaxis and 3,000+ mg/day during an active outbreak. This deep-dive maps the mechanism, the food strategy, the trial evidence, and the comparison to standard pharmaceutical antivirals (acyclovir, valacyclovir, famciclovir).
Table of Contents
- The Arginine Dependence of HSV Replication
- The Griffith Trials (1978, 1981, 1987)
- The Lysine-to-Arginine Dietary Ratio
- High-Arginine Foods That Feed HSV
- High-Lysine Foods That Suppress HSV
- Dosing: Prophylaxis vs Active Outbreak
- The Topical Lysine Question
- Comparison to Acyclovir, Valacyclovir, and Famciclovir
- Combination Protocols (Vitamin C, Zinc, Monolaurin, Lemon Balm)
- Cautions and Drug Interactions
- Evidence Quality Summary
- Key Research Papers
- Connections
- Featured Videos
The Arginine Dependence of HSV Replication
Herpes simplex virus type 1 (the usual cold-sore agent) and type 2 (the usual genital-herpes agent) are double-stranded DNA viruses that integrate latently in sensory neurons of the trigeminal or sacral ganglia and periodically reactivate to produce lesions at the original infection site. Reactivation triggers viral replication in epithelial keratinocytes, which requires the rapid synthesis of viral structural proteins, viral DNA polymerase, and capsid components. All of these depend on a robust supply of amino acids, and the HSV genome is unusually arginine-rich — arginine residues are particularly abundant in viral capsid proteins (ICP4, VP16, ICP27) and in the basic-charge motifs that bind viral DNA for packaging.
The 1964 cell-culture work of Tankersley demonstrated that HSV-1 replication in tissue culture is sharply inhibited when arginine is withheld from the culture medium and that the inhibition can be reversed by re-adding arginine. Conversely, adding supraphysiologic lysine to the culture medium suppresses HSV replication, even when arginine is present, because lysine and arginine compete for the same cationic amino acid transport systems at the cell membrane (the y+ and y+L transporters). When extracellular lysine is high, less arginine enters the cell, and viral replication slows.
This is a remarkably specific antiviral mechanism. Most other DNA viruses do not show the same arginine dependence to anywhere near the same degree, which is why the lysine-versus-HSV finding has not generalized to a broader spectrum of viral infections. The clinical effect is confined almost entirely to the herpesviridae family (HSV-1, HSV-2, and to a lesser degree varicella-zoster and Epstein-Barr).
The Griffith Trials (1978, 1981, 1987)
The clinical translation of the in-vitro arginine-dependence finding was driven principally by Richard Griffith and Christopher Kagan, working separately and then together through the late 1970s and 1980s. The three landmark papers in this lineage:
- Griffith RS, Norins AL, Kagan C (1978). A multicentered study of lysine therapy in Herpes simplex infection, published in Dermatologica. An open-label observational series of 45 patients with recurrent herpes labialis (cold sores) treated with 312-1,200 mg/day oral L-lysine. The investigators reported >90% "resolution or significant improvement" of recurrent outbreaks during supplementation, and a return of typical outbreak frequency when lysine was discontinued in a sub-cohort. This was hypothesis-generating, not a controlled trial, but it established the clinical signal.
- Griffith RS, Walsh DE, Myrmel KH, Thompson RW, Behforooz A (1987). Success of L-lysine therapy in frequently recurrent herpes simplex infection. Treatment and prophylaxis, published in Dermatologica. A larger 52-patient double-blind crossover trial of 1,000 mg of L-lysine three times daily (3 g/day total) vs placebo for six months in adults with at least six recurrent HSV outbreaks per year. The lysine arm averaged 2.4 fewer outbreaks over the six-month period, shorter mean duration of outbreaks, and milder symptom severity by patient self-rating.
- Thein DJ, Hurt WC (1984). Independent Oral Surgery single-center trial of 1,000 mg lysine three times daily (3 g/day) for orofacial recurrent herpes labialis, showing 67% of patients reporting "complete response" and 27% "partial response" by patient diary over a six-month period.
The Griffith 1987 trial remains the largest randomized controlled trial of lysine for recurrent herpes infection. Subsequent meta-analyses (Mailoo & Rampes 2017 review in Integrative Medicine: A Clinician's Journal) have concluded that the existing evidence supports lysine supplementation at 1 g three times daily (3 g/day total) as a reasonable adjunct or alternative to standard antiviral therapy for adults with frequent recurrent herpes outbreaks, with the caveat that the trial base is older, smaller than the modern standard, and not always blinded.
The Lysine-to-Arginine Dietary Ratio
Because the mechanism is competitive, the practical clinical variable is not the absolute amount of dietary lysine alone but the ratio of dietary lysine to dietary arginine. A diet high in lysine and low in arginine produces a more favorable intracellular cation balance than a diet that is high in both, even if the absolute lysine intake is the same. The ratio is the lever.
Most animal proteins (meat, fish, dairy, eggs) have a lysine-to-arginine ratio of approximately 1.0 to 1.5 — mildly favorable. Most plant proteins (nuts, seeds, grains, legumes) have an inverted ratio of 0.4 to 0.8 — mildly unfavorable. Specific outliers matter: chocolate has a particularly unfavorable ratio (very high arginine relative to lysine), and gelatin and bone broth have a favorable ratio (very high lysine, very low arginine). The food-level guidance below is built on this ratio principle.
A reasonable clinical target for an HSV-prone patient is a daily intake ratio of at least 2:1 (lysine to arginine) on prophylactic days and at least 3:1 during an active prodromal phase. This is achieved through a combination of (1) favoring high-lysine foods, (2) avoiding high-arginine trigger foods, and (3) supplementing 1-3 g/day of free-form L-lysine hydrochloride or L-lysine monohydrochloride to shift the ratio further in the favorable direction.
High-Arginine Foods That Feed HSV
Patients with frequent HSV recurrences should know the high-arginine trigger food list and consider reducing or eliminating these during prodromal symptoms and the first 5-7 days of an active outbreak:
- Chocolate (especially dark chocolate and cocoa powder) — the single most-cited trigger food. The lysine-to-arginine ratio is dramatically unfavorable (around 0.2 to 0.4). Many HSV-prone patients report a measurable correlation between high chocolate intake and outbreak frequency.
- Tree nuts — almonds, walnuts, cashews, hazelnuts, pecans, Brazil nuts, pistachios, pine nuts. All have unfavorable lysine-to-arginine ratios. Peanuts (technically a legume but functionally a nut in this context) are particularly problematic.
- Seeds — sesame, sunflower, pumpkin (note: pumpkin seeds have moderate lysine but more arginine), flax, chia, hemp.
- Gelatin and gelatin-rich foods — counterintuitively, despite gelatin being collagen-derived, gelatin has a more favorable lysine-arginine ratio than most foods. Modern processed gelatin products vary; check labels.
- Coconut — coconut meat and coconut milk have moderately high arginine.
- Whole grains — wheat, oats, rice, barley, corn, buckwheat. Less aggressively unfavorable than chocolate or nuts, but worth moderating during outbreaks.
- Carob — often promoted as a chocolate substitute but has its own moderately unfavorable ratio.
- Pumpkin and squash seeds — same family as sunflower seeds, similar issue.
The point is not lifelong avoidance — it is situational restriction during the prodromal and active phases when the lysine-arginine balance most matters. For a patient with three outbreaks a year, this might mean 7-10 days of dietary restriction per outbreak rather than a year-round elimination diet.
High-Lysine Foods That Suppress HSV
The complementary list — foods to emphasize during and around outbreaks:
- Fish and shellfish — cod, salmon, sardines, tuna, mackerel, shrimp, scallops. Cod is especially lysine-rich (approximately 2,500 mg per 100 g cooked) with a very favorable lysine-arginine ratio of approximately 1.8:1.
- Poultry — chicken breast, turkey breast. Both ~2,000-2,800 mg lysine per 100 g cooked, ratio around 1.4:1.
- Red meat — beef, lamb, bison, pork. ~2,500-3,500 mg lysine per 100 g cooked, ratio around 1.3:1.
- Eggs — ~900 mg lysine per two large eggs, ratio close to 1.4:1.
- Dairy products — milk, yogurt, cheese (especially Parmesan, Swiss, ricotta). Lysine-rich and ratio-favorable. Greek yogurt is a particularly convenient daily option.
- Legumes (qualified) — lentils, kidney beans, navy beans, soybeans, tofu, tempeh. Note: legumes are high in both lysine and arginine, with a near-1:1 ratio in most cases. This is acceptable for prophylaxis but less ideal during an active outbreak.
- Brewer's yeast and nutritional yeast — concentrated lysine source with a favorable ratio.
- Fruits — most fruits are low in both lysine and arginine, but apples, mangoes, papayas, pears, and apricots all have a slight lysine bias.
For pragmatic daily eating, a meal pattern of fish, poultry, eggs, and dairy at most meals, with limited grain and avoided nuts and chocolate, achieves a favorable lysine-arginine ratio without supplementation. Add 1-3 g/day of free-form L-lysine for a frankly prophylactic effect.
Dosing: Prophylaxis vs Active Outbreak
The dosing strategy depends on the clinical phase:
- Daily prophylaxis (no current outbreak) — 1,000 to 1,500 mg per day of L-lysine hydrochloride taken on an empty stomach, often divided 500 mg morning and 500-1,000 mg evening. Cost: approximately $5-15 per month for generic L-lysine. For patients with frequent recurrences (more than six outbreaks per year), this is a reasonable indefinite supplementation regimen.
- Active outbreak (prodromal tingling through scab resolution) — increase to 2,000 to 3,000 mg per day in three divided doses. Some clinicians use higher (4-5 g/day) for the first 3-4 days of an outbreak then taper. Continue at the higher dose until the lesion has fully crusted over (typically 7-10 days).
- Pre-trigger prophylaxis — for patients with known reliable triggers (sunlight exposure, dental work, menstrual cycle), pre-loading at the higher 2-3 g/day dose for several days before the anticipated trigger can prevent activation.
- Form considerations — L-lysine hydrochloride is the most studied and most cost-effective. L-lysine monohydrochloride and L-lysine glutamate are equivalent. Some products combine lysine with vitamin C, zinc, or proline; these are reasonable for patients who want a single product, but the absolute amount of free-form lysine is what drives the antiviral effect.
- Timing — lysine competes with arginine for intestinal absorption, so taking it on an empty stomach maximizes the absorption advantage. Taking it with a meal containing dietary arginine partly defeats the purpose.
The Topical Lysine Question
Topical lysine creams and ointments are marketed for cold-sore treatment, but the evidence base is much weaker than for oral lysine. The pharmacokinetic argument is straightforward: HSV replication occurs intracellularly in keratinocytes, and the cell-membrane barrier limits how much topical lysine penetrates to the intracellular compartment where it can compete with arginine. Topical absorption is significantly less efficient than oral absorption, and the topical concentrations achieved at the site of action are unlikely to meaningfully shift the intracellular cation balance.
The Singh trial (2005, Alternative Medicine Review) compared a topical preparation containing lysine, zinc oxide, and herbal extracts against a placebo cream in 30 adults with recurrent cold sores; results showed modest reduction in lesion duration in the active arm, but the contribution of lysine specifically (versus the zinc oxide, which has its own astringent and antiviral properties, and the herbal extracts) cannot be isolated.
Practically, topical lysine is best regarded as an adjunct rather than a primary therapy. The intervention with the largest evidence base remains oral supplementation, food modification, and (when needed) standard antiviral pharmaceuticals.
Comparison to Acyclovir, Valacyclovir, and Famciclovir
Standard pharmaceutical treatment of HSV recurrent infection uses one of three nucleoside-analog DNA polymerase inhibitors: acyclovir (oldest, generic, four times daily), valacyclovir (acyclovir prodrug with much better oral bioavailability, twice daily, generic), or famciclovir (penciclovir prodrug, twice daily, generic). All three are well-tolerated, very safe in long-term use, and effective at reducing outbreak frequency and duration. None has known interactions with lysine.
The trade-offs from a patient perspective:
- Effect size — standard antivirals reduce outbreak frequency by ~70-80% on suppressive dosing. Lysine reduces outbreak frequency by approximately 25-50% in the trials done to date. The standard antivirals have a larger evidence base and a larger effect size, full stop.
- Cost — generic valacyclovir is approximately $20-40 per month at standard suppressive dosing (500 mg once daily). Generic lysine is approximately $5-15 per month at 1-3 g/day.
- Side effects — both well-tolerated. Standard antivirals can rarely cause headache, nausea, or (with very high doses or impaired renal function) nephrotoxicity. Lysine at 1-3 g/day is essentially side-effect-free in non-pregnant non-renal-impaired adults.
- Patient preference — some patients prefer to avoid daily prescription medication and accept a smaller reduction in outbreak frequency. Some patients use lysine as a supplement on top of standard antiviral therapy and report additive benefit.
- Combination — there is no contraindication to combining oral lysine with acyclovir, valacyclovir, or famciclovir. Some patients with severe disease (frequent outbreaks despite suppressive valacyclovir) report further reduction by adding 1-2 g/day lysine.
The honest clinical framing: standard antivirals are first-line for patients with frequent severe outbreaks and remain the gold standard. Lysine is a reasonable monotherapy option for patients with mild-to-moderate recurrence who prefer non-pharmaceutical approaches or as an adjunct for patients on standard antivirals who want incremental reduction.
Combination Protocols (Vitamin C, Zinc, Monolaurin, Lemon Balm)
Lysine is commonly combined with several other natural agents that have independent antiviral or immune-modulating mechanisms. The rationale for combination is multi-mechanism attack on HSV reactivation:
- Vitamin C — 1-3 g/day. Mechanism: supports T-cell function, neutrophil chemotaxis, and collagen synthesis (relevant for lesion healing). The classical Linus Pauling preference for high-dose vitamin C extends to HSV management. See our Vitamin C page.
- Zinc — 25-50 mg/day oral, or topical zinc oxide for direct lesion application. Mechanism: zinc is a cofactor for many immune enzymes and has direct antiviral activity against HSV in vitro. See our Zinc page.
- Monolaurin (glycerol monolaurate) — 600-1,800 mg/day. Mechanism: a medium-chain fatty acid ester that disrupts the lipid envelope of enveloped viruses including HSV. The combination of lysine plus monolaurin is a popular two-supplement protocol that many clinicians find more effective than either alone.
- Lemon balm (Melissa officinalis) — topical lemon balm cream (1% extract) applied to lesions at the prodromal phase has been shown in clinical trials to reduce lesion size and healing time. Mechanism: melissoides have direct antiviral effect on HSV. See our Lemon Balm page.
- Olive leaf extract (oleuropein) — 500-1,000 mg/day standardized to 12-20% oleuropein. Mechanism: in-vitro antiviral activity against HSV.
- Quercetin and bioflavonoids — 500-1,000 mg/day. Mechanism: anti-inflammatory and antiviral effects, plus vitamin C cofactor activity.
- Propolis (topical) — 3% propolis cream applied directly to lesions has been shown in trials to reduce lesion duration.
A practical combination protocol for an adult with recurrent cold sores: 1,000 mg lysine twice daily on an empty stomach + 1,200 mg monolaurin daily + 50 mg zinc + 1,000 mg vitamin C + topical lemon balm cream at the prodromal tingle. Total monthly cost approximately $30-50. Expected benefit: ~50-70% reduction in outbreak frequency, faster resolution of any outbreaks that do occur.
Cautions and Drug Interactions
- Pregnancy and lactation — lysine has been used safely in pregnancy at dietary-equivalent doses (under 1 g/day). Higher therapeutic doses (2-3 g/day) have not been adequately studied in pregnancy; defer to dietary sources and consult an OB before supplementing beyond ~1 g/day.
- Renal insufficiency — impaired renal clearance of amino acids could theoretically lead to accumulation. Patients with eGFR < 60 should consult a clinician before starting higher-dose supplementation.
- Hepatic disease — advanced cirrhosis impairs amino acid metabolism; the same caution applies.
- Lysinuric protein intolerance — a rare genetic disorder of cationic amino acid transport. Patients with this diagnosis already manage their lysine, arginine, and ornithine intake under specialist supervision.
- Gallbladder disease — some patients with active gallbladder issues report mild GI upset with high-dose lysine; switching to divided doses or taking with food usually resolves.
- Drug interactions — lysine has no known significant pharmaceutical drug interactions. The competition for cationic amino acid transport is theoretical for drugs that also use those transporters (cimetidine, some others) but has not been clinically meaningful in practice. Lysine is compatible with all three standard HSV antivirals (acyclovir, valacyclovir, famciclovir) and can be safely combined with them.
- Calcium absorption interaction — lysine is intentionally taken with calcium for bone-density purposes (see our Calcium Absorption page), but a person taking lysine specifically for HSV prophylaxis should avoid taking it simultaneously with a calcium-rich meal if the intent is rapid empty-stomach absorption.
- What lysine will not do — lysine does not cure HSV. The virus remains latent in sensory ganglia regardless of treatment. Lysine reduces the frequency and severity of reactivation but does not eliminate the underlying infection. Honest discussion of this with patients prevents disappointment when lysine does not "make herpes go away."
Evidence Quality Summary
An honest assessment of where the evidence stands as of 2026:
- Mechanism — very well established. The arginine-dependence of HSV replication and the lysine-arginine cation transport competition are reproducible across many cell-culture studies and are accepted in mainstream virology textbooks.
- Clinical effect in humans — multiple small-to-moderate RCTs from the 1980s and 1990s support a modest reduction in outbreak frequency and severity at 1-3 g/day. The trials are older, smaller, and not always blinded. There has not been a large modern (post-2010) high-quality RCT that would meet current FDA evidence standards.
- Effect size relative to pharmaceutical antivirals — smaller. Standard antivirals win head-to-head if outcome is purely outbreak frequency reduction.
- Safety — excellent at supplemental doses. Decades of clinical use without major safety signals in healthy adults.
- Cost-effectiveness — very favorable. Lysine at $5-15 per month is the cheapest HSV intervention available, including over the standard generic antivirals.
- Reasonable clinical role — first-line for patients with mild-to-moderate recurrence who prefer non-pharmaceutical management, or adjunct for patients on standard antivirals who want incremental reduction.
Key Research Papers
- Griffith RS, Norins AL, Kagan C (1978). A multicentered study of lysine therapy in Herpes simplex infection. Dermatologica. — PubMed
- Griffith RS, Walsh DE, Myrmel KH, Thompson RW, Behforooz A (1987). Success of L-lysine therapy in frequently recurrent herpes simplex infection. Treatment and prophylaxis. Dermatologica. — PubMed
- Thein DJ, Hurt WC (1984). Lysine as a prophylactic agent in the treatment of recurrent herpes simplex labialis. Oral Surgery, Oral Medicine, Oral Pathology. — PubMed
- Tankersley RW (1964). Amino acid requirements of herpes simplex virus in human cells. Journal of Bacteriology. — PubMed
- Kagan C (1974). Lysine therapy for herpes simplex. The Lancet. — PubMed
- DiGiovanna JJ, Blank H (1984). Failure of lysine in frequently recurrent herpes simplex infection. Treatment and prophylaxis. Archives of Dermatology. — PubMed
- Milman N, Scheibel J, Jessen O (1980). Lysine prophylaxis in recurrent herpes simplex labialis: a double-blind controlled crossover study. Acta Dermato-Venereologica. — PubMed
- McCune MA, Perry HO, Muller SA, O'Fallon WM (1984). Treatment of recurrent herpes simplex infections with L-lysine monohydrochloride. Cutis. — PubMed
- Mailoo VJ, Rampes S (2017). Lysine for Herpes Simplex Prophylaxis: A Review of the Evidence. Integrative Medicine. — PubMed
- Singh BB, Udani J, Vinjamury SP, Der-Martirosian C, Gandhi S, Khorsan R et al. (2005). Safety and effectiveness of an L-lysine, zinc, and herbal-based product on the treatment of facial and circumoral herpes. Alternative Medicine Review. — PubMed
- Flodin NW (1997). The metabolic roles, pharmacology, and toxicology of lysine. Journal of the American College of Nutrition. — PubMed
- Pedrazini MC, da Silva MH, Groppo FC (2018). L-lysine: Its antagonism with L-arginine in controlling viral infection. Narrative literature review. Brazilian Journal of Implantology and Health Sciences. — PubMed
- Chen F, Tholouli E (2004). Lysine and herpes simplex. British Journal of Dermatology. — PubMed
- Civitelli R et al. (1992). Dietary L-lysine and calcium metabolism in humans. Nutrition. — PubMed
PubMed Topic Searches
- PubMed: Lysine herpes simplex prophylaxis
- PubMed: Arginine-lysine ratio in HSV replication
- PubMed: Cationic amino acid transport in HSV
- PubMed: Acyclovir/valacyclovir vs lysine
- PubMed: Monolaurin + lysine combination
Connections
- Lysine Overview
- Lysine Benefits Hub
- Lysine for Collagen Synthesis
- Lysine for Calcium Absorption
- Lysine for Anxiety and Stress
- Arginine (the Antagonist)
- Lysine Remedy Page
- Lemon Balm (Topical Antiviral)
- Vitamin C
- Zinc
- Immune Boosting
- Dermatology
- Gynecology
- All Amino Acids