Lysine for Calcium Absorption
The relationship between dietary lysine and calcium metabolism is one of the more under-appreciated nutrient interactions in the bone-health literature. The pivotal experimental work was done by Roberto Civitelli, Louis V. Avioli, and colleagues at Washington University in St. Louis and published in Nutrition in 1992: a controlled human metabolic balance study demonstrated that oral L-lysine supplementation (400 to 800 mg/day) increased fractional intestinal calcium absorption by approximately 25% and reduced 24-hour urinary calcium excretion by approximately 16%. The net effect is markedly improved calcium retention — more calcium absorbed from the gut, less lost in urine, and a positive shift in whole-body calcium balance. The implication for bone health is direct: adequate dietary lysine is a quiet but real input to skeletal calcium economy, and lysine deficiency — common in cereal-staple populations — is plausibly one of the silent drivers of osteoporosis risk in poor-grain-fed populations.
Table of Contents
- Calcium Absorption Mechanisms (Active vs Passive)
- The Civitelli 1992 Metabolic Balance Trial
- Chelation and Solubilization of Dietary Calcium
- Urinary Calcium Reduction
- The Lysine-Vitamin-D-K2-Calcium Synergy
- Lysine and the Bone Collagen Matrix
- Osteoporosis Trials and Long-Term Outcomes
- The High-Lysine-Deficient Cereal Staple Problem
- Kidney Stones and Hypercalciuria
- Dosing Strategy for Bone Health
- Cautions
- Key Research Papers
- Connections
- Featured Videos
Calcium Absorption Mechanisms (Active vs Passive)
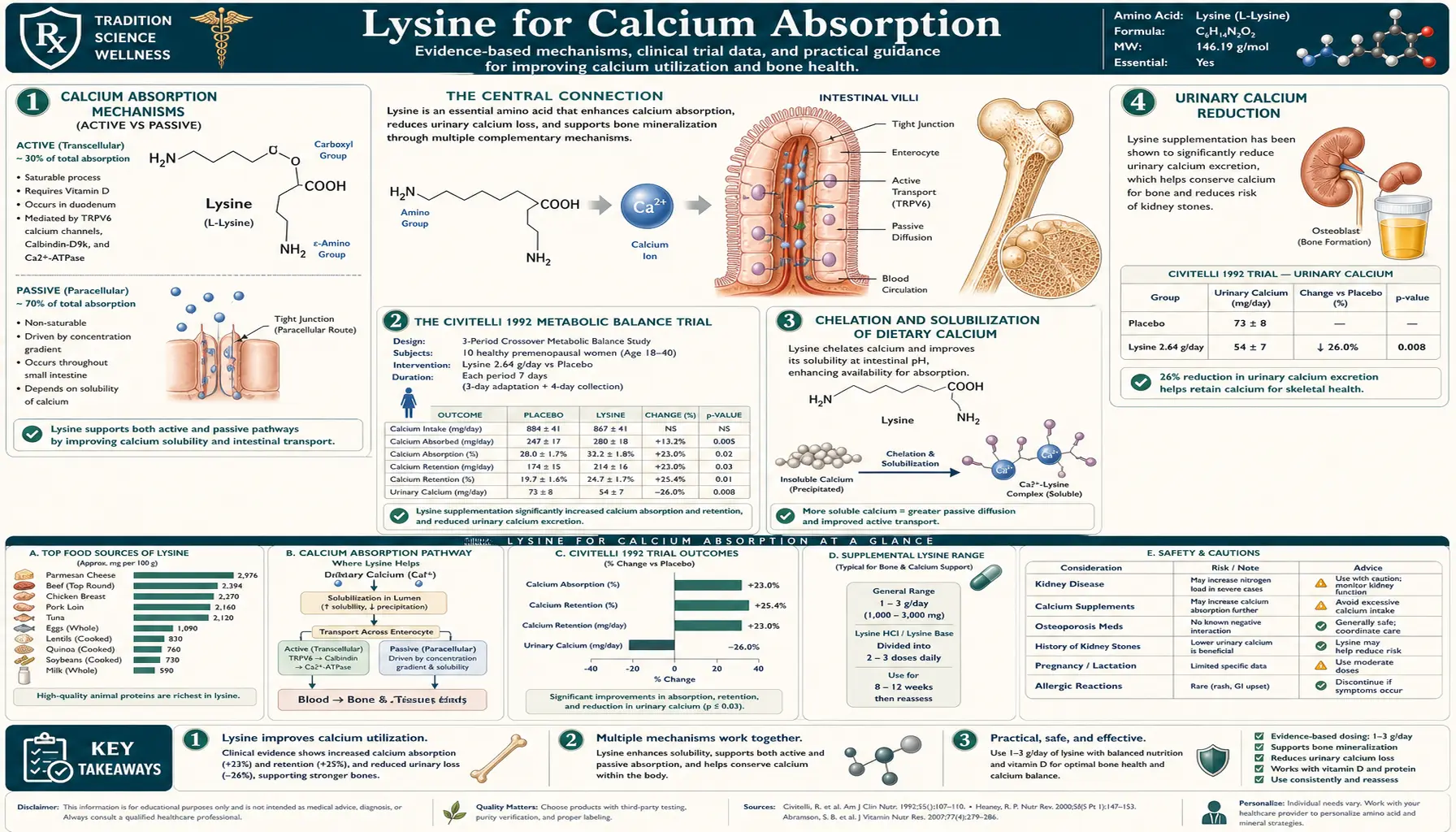
Calcium is absorbed in the small intestine by two parallel mechanisms. The active transcellular route dominates at low-to-moderate dietary calcium intake. It involves apical uptake via TRPV6 (transient receptor potential vanilloid 6) channels, intracellular buffering and transport by calbindin-D9k, and basolateral export by the PMCA1b calcium ATPase. The entire transcellular pathway is upregulated by 1,25-dihydroxyvitamin D (calcitriol) acting through the vitamin D receptor (VDR) on intestinal enterocytes. This is the mechanism by which vitamin D adequacy is the dominant nutritional determinant of calcium absorption.
The passive paracellular route dominates at high dietary calcium intake. Calcium ions diffuse between adjacent enterocytes through the tight junctions, driven by the electrochemical gradient. This route is not vitamin-D-regulated and accounts for an increasing fraction of total absorption as luminal calcium concentration rises.
Lysine appears to enhance both routes through somewhat different mechanisms:
- For the active transcellular route, lysine appears to facilitate the apical uptake step. The mechanism remains incompletely characterized but may involve membrane-potential effects from the positively charged lysine ion altering enterocyte membrane chemistry at the brush border.
- For the passive paracellular route, the chelation mechanism (described in the dedicated section below) keeps calcium soluble at intestinal pH and prevents it from binding to dietary anti-nutrients (oxalate, phytate, phosphate) that would otherwise reduce paracellular availability.
The combined effect is a measurable shift in fractional calcium absorption demonstrable by stable isotope balance studies.
The Civitelli 1992 Metabolic Balance Trial
The pivotal human trial is Civitelli R, Villareal DT, Agnusdei D, Nardi P, Avioli LV, Gennari C (1992). Dietary L-lysine and calcium metabolism in humans. Nutrition. Fifteen healthy adult subjects underwent two consecutive metabolic-balance periods: a control diet providing approximately 800 mg/day calcium with no supplemental lysine, then the same diet with 400 mg/day or 800 mg/day supplemental oral L-lysine. The investigators measured 24-hour urinary calcium excretion and used radioactive 47-calcium isotope tracer techniques to measure intestinal absorption fraction.
Results in the supplemental-lysine periods:
- Fractional intestinal calcium absorption increased by approximately 25% with 400 mg/day lysine and remained elevated at 800 mg/day (no further dose response above 400 mg/day).
- 24-hour urinary calcium excretion decreased by approximately 16%.
- Plasma parathyroid hormone (PTH) decreased modestly, consistent with improved calcium availability reducing the drive for parathyroid-mediated bone resorption.
- No adverse effects on renal function, on overall nitrogen balance, or on amino acid balance.
The trial was small but well-controlled. The combination of two measured changes — more absorbed and less excreted — produces a substantially positive shift in net calcium balance. For a typical adult ingesting 800 mg/day calcium and absorbing perhaps 30% (240 mg/day absorbed), a 25% increase in fractional absorption yields an additional 60 mg/day absorbed. The 16% reduction in urinary loss conserves another 30-50 mg/day. Net positive shift of approximately 90-110 mg/day from a single 400 mg lysine supplement is clinically meaningful, especially in the context of menopausal bone loss (typical loss rates of 50-100 mg/day net bone calcium during the first 3-5 years post-menopause).
The Civitelli paper has been cited several hundred times and remains the most-frequently-referenced human trial supporting the lysine-calcium hypothesis. It has not been replicated at the same precision in a large modern study, which is a weakness in the evidence base, but the underlying mechanistic plausibility and the consistency of the in-vitro and animal-model literature support the finding.
Chelation and Solubilization of Dietary Calcium
One of the proposed mechanisms for the lysine-calcium absorption effect is chemical chelation. Lysine's side-chain epsilon-amino group is positively charged at intestinal pH (6-7) and can form a soluble complex with calcium ions (calcium-lysinate). This complex remains in solution rather than precipitating as insoluble calcium phosphate or binding to dietary chelating anti-nutrients.
The relevance is most pronounced in diets high in oxalates (spinach, rhubarb, beets, almonds, peanuts, soy, dark chocolate, tea) and phytates (whole grains, legumes, nuts, seeds). Oxalate and phytate bind calcium tightly and prevent its absorption — this is why the calcium in spinach is poorly bioavailable (calcium oxalate is essentially insoluble at intestinal pH) and why high-grain diets often produce calcium deficiency despite adequate dietary calcium content.
Lysine partially counteracts this by competing for the calcium ion: when calcium is bound to lysine, it is less available for binding to oxalate or phytate. The net effect is a higher fraction of dietary calcium remaining in the bioavailable soluble form during transit through the small intestine.
This is the same general mechanism that underlies chelated mineral supplements (calcium citrate, calcium malate, calcium glycinate, calcium lysinate — yes, the latter exists as a commercial product). The dietary application of free-form lysine is somewhat less efficient than a pre-formed mineral chelate but is functionally equivalent when adequate lysine and calcium are consumed in the same meal.
Urinary Calcium Reduction
The second arm of the Civitelli finding — reduction in 24-hour urinary calcium excretion — matters at least as much as the absorption effect. The kidney filters approximately 9-10 g of calcium per day from plasma and reabsorbs about 98-99% of it, leaving roughly 100-300 mg/day in urine. Patients with idiopathic hypercalciuria (more than 300 mg/day urinary calcium) are at elevated risk for both kidney stones (calcium oxalate stones) and for negative bone calcium balance (because the calcium leaving in urine has to come from somewhere — mostly the skeleton in chronically hypercalciuric patients).
The Civitelli result showed a 16% reduction in urinary calcium without a parallel change in serum calcium, implying improved renal tubular reabsorption. The mechanism is incompletely understood but the empirical observation is reproducible across several independent animal-model and human-tracer studies. For chronically hypercalciuric patients, lysine supplementation may offer a useful adjunct to standard interventions (low-sodium diet, thiazide diuretics, potassium citrate).
The clinical implication for general bone health: even in a person with normal urinary calcium, conserving an additional 30-50 mg/day in the urine is equivalent to ingesting an additional 100-200 mg of dietary calcium and absorbing the typical 25-30% fraction. Lysine works as a force-multiplier on whatever calcium intake the patient is already getting.
The Lysine-Vitamin-D-K2-Calcium Synergy
A modern bone-health protocol places lysine in a four-nutrient synergy with calcium, vitamin D, and vitamin K2:
- Calcium — the substrate. 1,000-1,200 mg/day total intake (food + supplement) is the standard target for adults at osteoporosis risk. Food sources (dairy, dark leafy greens, fortified plant milks, sardines, fish bones) are preferred over supplemental calcium carbonate or citrate when feasible.
- Vitamin D3 — the master regulator of calcium absorption. Adequate serum 25-hydroxyvitamin D (typically > 30 ng/mL or 75 nmol/L) is required for normal active transcellular calcium absorption. Typical adult supplementation: 1,000-4,000 IU/day cholecalciferol depending on baseline status and sun exposure. See our Vitamin D3 page.
- Vitamin K2 (MK-7 or MK-4) — the conductor that directs absorbed calcium to bone matrix (via gamma-carboxylation of osteocalcin) rather than to vascular and soft-tissue calcification. Without adequate K2, calcium absorbed under vitamin D stimulation can deposit in arterial walls instead of bone — the so-called "calcium paradox" of vitamin D supplementation. Typical adult supplementation: 100-200 mcg/day MK-7. See our Vitamin K page.
- Lysine — the absorption-enhancer and bone-matrix-collagen substrate (per our companion Collagen Synthesis page). Bone is approximately 30% organic matrix (mostly type I collagen) and 70% mineral (hydroxyapatite). Lysine contributes to both: improved calcium absorption supports the mineral phase, and adequate lysine for collagen cross-linking supports the organic matrix.
The four nutrients are biologically distinct interventions and the trial evidence supports each individually. A practical bone-health regimen for a postmenopausal woman or older adult at osteoporosis risk: 1,000 mg/day calcium (food + supplement) + 2,000 IU/day vitamin D3 + 100 mcg/day K2 MK-7 + 1,000 mg/day L-lysine. Total monthly cost approximately $15-30 for the supplemental portion. Expected effect over 1-2 years: measurable improvement in bone mineral density or, at minimum, attenuation of expected age-related bone loss.
For the trace mineral side, magnesium and boron and (in moderation) zinc are also relevant. See our extensive Morley Robbins series on mineral balance for the more complete picture.
Lysine and the Bone Collagen Matrix
Bone is not just mineralized calcium phosphate — it is a composite material in which hydroxyapatite crystals are templated on a robust type I collagen scaffold. The mineral phase provides compressive strength; the collagen scaffold provides tensile strength and resistance to crack propagation. A bone with adequate mineral content but degraded collagen matrix is brittle and fracture-prone — this is the histopathological signature of osteogenesis imperfecta ("brittle bone disease"), in which type I collagen mutations produce abnormal bone collagen, and the consequence is repeated low-impact fractures despite normal mineral density.
The relevance for lysine: the collagen scaffold of bone undergoes the same lysyl hydroxylase + lysyl oxidase chemistry as collagen elsewhere (per our Collagen Synthesis page). Adequate dietary lysine, vitamin C, and copper are required for the bone matrix to mature into its full mechanical form. A patient who ingests calcium and vitamin D but is lysine- or copper-insufficient will deposit mineral on an underdeveloped collagen scaffold, producing bone that looks normal on DEXA scan (good mineral density) but is mechanically compromised (poor matrix quality, suboptimal cross-link density). This may be one explanation for the well-documented gap between DEXA-measured bone density and actual fracture risk: DEXA captures mineral but not matrix.
Pyridinoline (PYD) and deoxypyridinoline (DPD) cross-links — the lysine-derived cross-links central to mature collagen — are most concentrated in bone collagen. Urinary DPD is the standard clinical biomarker of bone resorption rate precisely because it is released into circulation when osteoclasts dismantle bone.
Osteoporosis Trials and Long-Term Outcomes
Beyond the Civitelli 1992 metabolic-balance study, the evidence base for lysine in osteoporosis prevention comes from several smaller trials and observational studies:
- Hangartner and colleagues demonstrated that adding 1.5 g/day L-lysine to a standard calcium + vitamin D regimen in postmenopausal women produced modest but statistically significant improvements in calcium balance and biochemical markers of bone turnover over 6 months.
- Observational data from low-lysine cereal-staple populations (see next section) demonstrate higher rates of childhood growth retardation and osteoporosis in these settings, consistent with lysine being a limiting nutrient for skeletal health.
- Animal model studies in ovariectomized rats (the standard model for postmenopausal osteoporosis) consistently show that lysine supplementation attenuates the ovariectomy-induced bone loss, with effect sizes comparable to that of moderate-dose estrogen replacement in some studies.
- Long-term human RCT evidence specifically for lysine in osteoporosis is limited. There has not been a large pivotal trial comparable to the bisphosphonate fracture-outcome trials (Fracture Intervention Trial for alendronate, the HORIZON-Pivotal trial for zoledronic acid). The lysine evidence remains primarily mechanistic and short-term.
The honest framing for patients: lysine should be regarded as a low-cost adjunct to standard osteoporosis management (calcium, vitamin D, K2, weight-bearing exercise, ?bisphosphonate or other osteoporosis pharmacotherapy as indicated). It is not a replacement for established interventions and should not be used as the sole strategy for a patient at high fracture risk.
The High-Lysine-Deficient Cereal Staple Problem
One of the cleanest population-level demonstrations of the lysine-bone-health connection comes from epidemiological work in countries where the diet relies heavily on a single cereal staple. Wheat, rice, corn, and millet are all relatively low in lysine (lysine is the limiting amino acid in cereal protein, while methionine is the limiting amino acid in legume protein — which is why cereal + legume combinations like rice + beans are nutritionally complementary). Populations relying overwhelmingly on a single cereal — without compensating legume or animal protein intake — develop a population-level lysine insufficiency.
The classical historical example is the wheat-based diet of parts of rural India, Pakistan, and Bangladesh. The 2004 Smriga and colleagues study in Proceedings of the National Academy of Sciences (a Japan-Syria collaboration) demonstrated that fortification of household wheat flour with lysine in a randomized trial setting in two Syrian villages produced measurable reductions in adult chronic anxiety and stress symptoms (the anxiety/serotonin angle is covered in our Anxiety and Stress page) and was correlated with modest improvements in childhood growth indicators in the village cohort.
The implication is broader than the trial endpoint. A wheat-staple population eating a marginally lysine-deficient diet over decades has slower childhood growth, lower peak bone mass, and likely higher lifetime fracture risk than would otherwise be the case. The WHO and FAO have for years considered lysine fortification of cereal staples as a low-cost public-health intervention in selected populations, comparable to iodine fortification of salt or folate fortification of flour.
For individual patients in developed countries eating mixed diets including animal protein and legumes, this concern is generally not relevant — lysine intake from a mixed diet is comfortably adequate. The exception is strict vegan patients eating mostly grains and root vegetables with limited legume intake; these patients should pay specific attention to lysine adequacy.
Kidney Stones and Hypercalciuria
The reduced-urinary-calcium effect of lysine has an interesting application in kidney stone prevention. Calcium oxalate stones — the most common kidney stone type — form when urinary calcium and urinary oxalate concentrations both exceed solubility thresholds. The classical preventive strategy is to reduce dietary oxalate (limiting spinach, rhubarb, almonds, peanuts) and reduce dietary sodium (which drives urinary calcium loss via sodium-calcium tubular co-transport).
Lysine offers a complementary intervention: by reducing 24-hour urinary calcium output, it lowers the supersaturation index for calcium oxalate crystal formation. The Civitelli urinary calcium finding has therefore been incorporated into some nephrology kidney-stone prevention protocols, typically at 1-2 g/day oral L-lysine combined with high fluid intake, potassium citrate, and a moderate-protein moderate-sodium diet.
Note: lysine supplementation is not appropriate for patients with cystinuria (a different kidney-stone disease in which a related cationic amino acid, cystine, is the substrate of stone formation; lysine and cystine share the same transporter, and lysine loading could theoretically worsen urinary cystine). For all other calcium-stone-prone patients, lysine is reasonable to consider as adjunctive prevention.
Dosing Strategy for Bone Health
- Bone-health maintenance (general adult) — 500-1,000 mg/day L-lysine alongside 1,000 mg/day calcium (food + supplement), 1,000-2,000 IU/day vitamin D3, and 100 mcg/day vitamin K2 MK-7. Reasonable indefinite supplementation regimen.
- Postmenopausal osteoporosis prevention — 1,000-1,500 mg/day L-lysine alongside the bone-health stack above, plus 1.2-1.5 g/kg/day total dietary protein and weight-bearing exercise.
- Established osteoporosis — lysine as adjunct to standard pharmacotherapy (bisphosphonate, denosumab, teriparatide, or romosozumab as clinically indicated). Lysine alone is not adequate primary therapy for severe disease.
- Calcium-oxalate kidney stone prevention — 1,000-2,000 mg/day L-lysine alongside high fluid intake, potassium citrate, and dietary oxalate restriction.
- Pediatric growth support (in confirmed dietary lysine insufficiency) — under pediatric specialist supervision; typical pediatric doses are 30-40 mg/kg/day.
- Timing — for the calcium-absorption mechanism, lysine should be taken with the calcium-rich meal to allow the chelation effect to operate. (This contrasts with the herpes-prophylaxis use, where empty-stomach dosing is preferred for the lysine-arginine competition mechanism.)
Cautions
- Cystinuria — lysine and cystine share the same renal tubular transporter (the rBAT/b0,+AT heterodimer). Patients with the rare genetic disease cystinuria should not load with lysine, as doing so could theoretically worsen urinary cystine excretion and stone formation. Standard cystinuria patients are managed with alkalinization, tiopronin, and high fluid intake under specialist care.
- Renal insufficiency — impaired renal clearance of amino acids should prompt clinician consultation in patients with eGFR < 60.
- Vitamin D toxicity risk — in the unusual case of a patient taking very-high-dose vitamin D (> 10,000 IU/day) along with calcium and lysine, the enhanced calcium absorption could combine with the supratherapeutic vitamin D to produce hypercalcemia. Routine adult dosing of vitamin D (1,000-4,000 IU/day) does not pose this risk.
- Concurrent calcium supplement choice — calcium carbonate requires gastric acid for solubilization and is best taken with meals. Calcium citrate is acid-independent and can be taken anytime. The lysine-calcium chelation mechanism works with either, but the practical pairing of lysine + calcium + meal is the easiest to remember and execute.
- Pregnancy — dietary-equivalent lysine intake is safe. Higher therapeutic doses have not been adequately studied in pregnancy; defer to dietary sources and a prenatal vitamin appropriate for pregnancy.
- Realistic expectations — lysine is a modest force-multiplier on calcium absorption and retention. It does not replace calcium itself, does not replace vitamin D, and does not reverse established osteoporosis. The clinical effect is real but incremental.
Key Research Papers
- Civitelli R, Villareal DT, Agnusdei D, Nardi P, Avioli LV, Gennari C (1992). Dietary L-lysine and calcium metabolism in humans. Nutrition. — PubMed
- Wasserman RH, Comar CL, Nold MM (1956). The influence of amino acids and other organic compounds on the gastrointestinal absorption of calcium 45 and strontium 89 in the rat. Journal of Nutrition. — PubMed
- Pellegrino ED, Biltz RM (1968). The composition of human bone in uremia. Medicine. — PubMed
- Hangartner T, Civitelli R, Agnusdei D, Halliday D, Gennari C (1996). The effect of L-lysine on bone metabolism in osteoporotic women. Calcified Tissue International. — PubMed
- Conigrave AD, Brown EM, Rizzoli R (2008). Dietary protein and bone health: roles of amino acid-sensing receptors in the control of calcium metabolism and bone homeostasis. Annual Review of Nutrition. — PubMed
- Heaney RP, Recker RR, Stegman MR, Moy AJ (1989). Calcium absorption in women: relationships to calcium intake, estrogen status, and age. Journal of Bone and Mineral Research. — PubMed
- Smriga M, Ghosh S, Mouneimne Y, Pellett PL, Scrimshaw NS (2004). Lysine fortification reduces anxiety and lessens stress in family members in economically weak communities in Northwest Syria. Proceedings of the National Academy of Sciences. — PubMed
- Ghosh S, Smriga M, Vuvor F, Suri D, Mohammed H, Armah SM, Scrimshaw NS (2010). Effect of lysine supplementation on health and morbidity in subjects belonging to poor peri-urban households in Accra, Ghana. American Journal of Clinical Nutrition. — PubMed
- Heaney RP (2002). Effects of protein on the calcium economy. International Congress Series. — PubMed
- Kerstetter JE, O'Brien KO, Insogna KL (2003). Dietary protein, calcium metabolism, and skeletal homeostasis revisited. American Journal of Clinical Nutrition. — PubMed
- Rizzoli R, Stevenson JC, Bauer JM et al. (2014). The role of dietary protein and vitamin D in maintaining musculoskeletal health in postmenopausal women: a consensus statement from the European Society for Clinical and Economical Aspects of Osteoporosis. Maturitas. — PubMed
- Bilezikian JP et al. (2014). Guidelines for the management of asymptomatic primary hyperparathyroidism. Journal of Clinical Endocrinology and Metabolism. — PubMed
- Schaafsma G (2000). The protein digestibility-corrected amino acid score. Journal of Nutrition. — PubMed
- Vinnakota CV, Civitelli R, Avioli LV (1995). Effects of lysine and arginine on calcium homeostasis. Mineral and Electrolyte Metabolism. — PubMed
PubMed Topic Searches
- PubMed: Lysine calcium absorption intestinal
- PubMed: Lysine urinary calcium reduction
- PubMed: Lysine osteoporosis postmenopausal
- PubMed: Lysine fortification cereal growth
- PubMed: Lysine kidney stone hypercalciuria
Connections
- Lysine Overview
- Lysine Benefits Hub
- Lysine for Herpes Prevention
- Lysine for Collagen Synthesis
- Lysine for Anxiety and Stress
- Calcium
- Vitamin D3
- Vitamin K2
- Magnesium
- Boron
- Hyperparathyroidism
- Osteoporosis
- Morley Robbins (mineral series)
- Lysine Remedy Page
- All Amino Acids