Inositol for PCOS & Insulin Sensitivity
Polycystic ovary syndrome (PCOS) is the indication for which inositol has the strongest evidence base of any nutraceutical for any condition that primarily affects women. The combined therapy of myo-inositol and D-chiro-inositol at the 40:1 ratio — mirroring the natural plasma physiology — restores ovulation, lowers free testosterone, normalizes LH/FSH, regularizes cycles, and matches metformin's HbA1c reduction with dramatically better tolerability. The Genazzani PCOS trials, the Unfer 2017 meta-analysis, the Costantino 2009 double-blind trial, and the Pundir 2024 systematic review prepared for the 2023 International Evidence-Based PCOS Guidelines collectively establish 4 g/day myo-inositol + 100 mg D-chiro-inositol as the evidence-based standard. This deep-dive walks through the IPG second-messenger mechanism that PCOS patients are functionally deficient in, the comparison with metformin, the practical 6-month treatment timeline, and the 40:1 ratio controversy.
Table of Contents
- What PCOS Is
- The IPG Deficiency — PCOS as an Inositol-Signaling Disease
- The Epimerase Paradox — Why Myo-Alone Is Not Enough
- The 40:1 Ratio and Its Physiological Basis
- The Genazzani PCOS Trials
- Unfer Meta-Analysis & Costantino 2009
- Inositol vs Metformin Head-to-Head
- The 2023 International PCOS Guidelines
- Practical Patient Protocol & Timeline
- Beyond PCOS — Insulin Resistance & Metabolic Syndrome
- Patient FAQ
- Cautions Specific to PCOS Patients
- Key Research Papers
- Connections
- Featured Videos
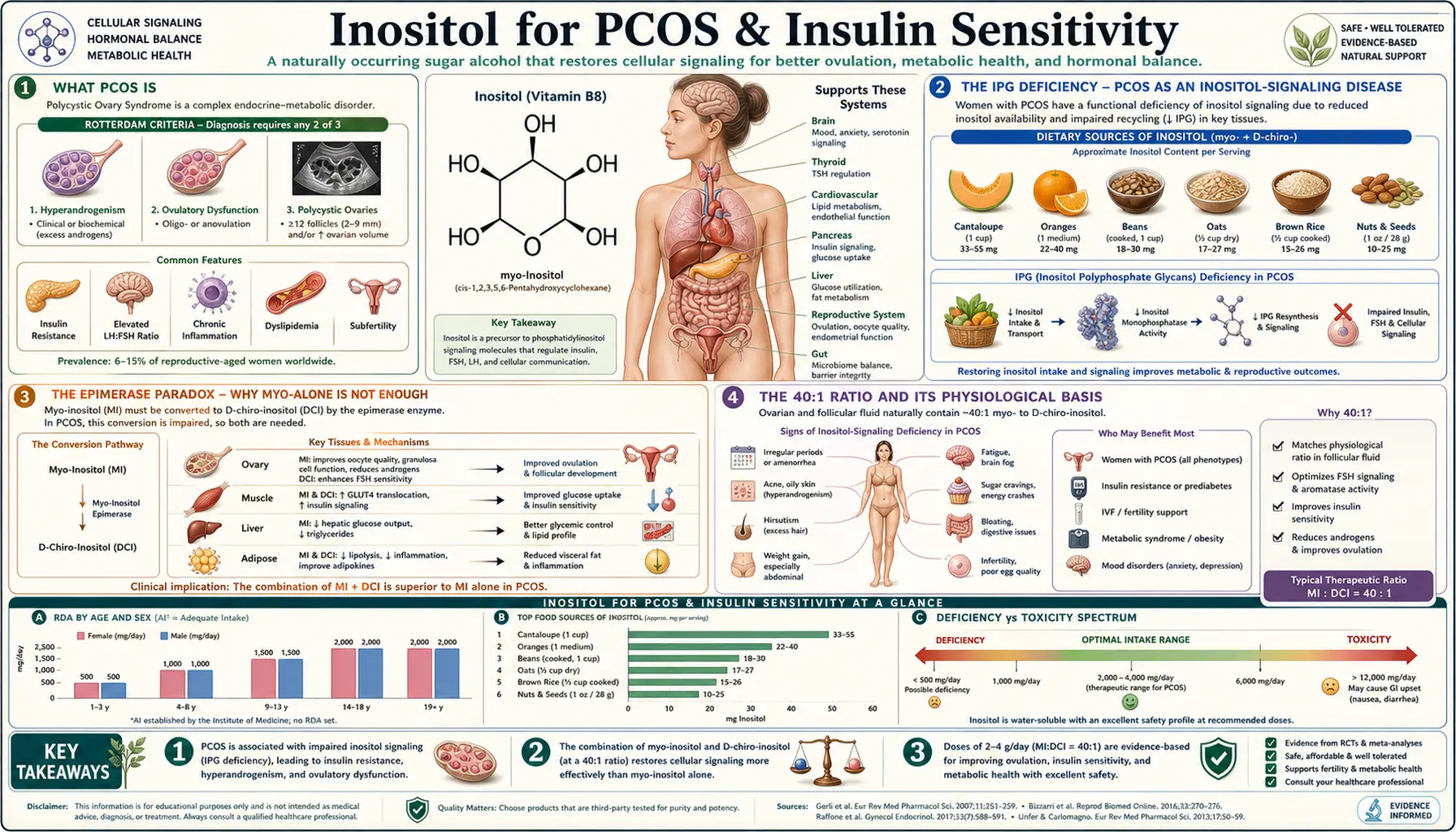
What PCOS Is
Polycystic ovary syndrome is the most common endocrine disorder in women of reproductive age, affecting an estimated 6 to 12 percent globally — close to 1 in 10 women. The Rotterdam criteria define PCOS by the presence of at least two of three features: oligo- or anovulation, clinical or biochemical hyperandrogenism, and polycystic ovarian morphology on ultrasound. The clinical presentation includes irregular or absent menstrual cycles, infertility, hirsutism (excess facial and body hair), acne, scalp hair thinning, weight gain (particularly central adiposity), and elevated risk of type 2 diabetes, dyslipidemia, hypertension, and cardiovascular disease.
Insulin resistance is the central pathological driver in the majority of PCOS patients — present in roughly 70% of lean women with PCOS and over 95% of overweight women with PCOS. The pathway is bidirectional and self-reinforcing: insulin resistance causes compensatory hyperinsulinemia, which stimulates ovarian theca cells to overproduce androgens (especially testosterone and androstenedione) and lowers sex-hormone-binding globulin (SHBG), increasing free testosterone bioavailability. The androgen excess then disrupts the normal LH-FSH ratio (LH rises, FSH falls), arrests follicular development at the antral stage, and prevents ovulation. The result is the characteristic polycystic ovary — not actually cysts but many small immature follicles arrested in development.
Conventional pharmaceutical treatment has historically targeted symptoms rather than the underlying signaling defect: oral contraceptives suppress androgen production but mask the disease, spironolactone blocks androgen receptors but is teratogenic, and metformin addresses insulin resistance but causes gastrointestinal side effects in 20-30% of patients. Inositol is the only nutraceutical that addresses the cellular root of the disease — the impaired insulin second-messenger signaling that drives both the metabolic and the reproductive features of PCOS.
For the broader clinical picture, see our PCOS disease page. For the metabolic context, see Insulin Resistance and Metabolic Syndrome.
The IPG Deficiency — PCOS as an Inositol-Signaling Disease
When insulin binds its receptor on a target cell (muscle, liver, adipose, ovary), it triggers a cascade in which receptor autophosphorylation activates downstream tyrosine kinases. One critical branch of that cascade releases inositol phosphoglycan (IPG) second messengers — small molecules derived from membrane glycosylphosphatidylinositol (GPI) anchors. IPGs come in two structural variants:
- IPG-A (myo-inositol-based) — mediates glucose uptake by stimulating GLUT4 translocation to the plasma membrane in skeletal muscle and adipocytes
- IPG-P (D-chiro-inositol-based) — mediates glycogen synthesis in muscle and liver by activating glycogen synthase and inhibiting glycogen phosphorylase
Multiple research groups (Larner, Romero, Asplin, and colleagues) demonstrated through the 1990s and 2000s that women with PCOS have impaired release of D-chiro-inositol-containing IPGs following insulin stimulation. Urinary D-chiro-inositol excretion is reduced, the IPG-P/IPG-A ratio is abnormal in serum, and the defect appears to be tissue-specific — some tissues (such as the ovary, paradoxically) accumulate D-chiro-inositol while others (skeletal muscle, liver) are functionally depleted. This means PCOS at the cellular level is not just "insulin resistance" in the generic sense; it is a specific deficiency in the second-messenger pathway that translates insulin binding into glucose uptake and storage.
Supplemental myo-inositol provides substrate for IPG-A regeneration in tissues that have become depleted, while supplemental D-chiro-inositol replaces the missing IPG-P signal in the muscle and liver. This is the mechanistic rationale for combined therapy at the physiological 40:1 ratio — restoring the natural balance rather than overloading one form at the expense of the other.
The Epimerase Paradox — Why Myo-Alone Is Not Enough
In healthy tissues, myo-inositol is converted to D-chiro-inositol by an insulin-dependent epimerase enzyme. This epimerase is tissue-specific in its expression and is upregulated by insulin signaling. In peripheral insulin-target tissues like skeletal muscle, the epimerase normally maintains adequate D-chiro-inositol levels to support glycogen synthesis. In the ovary, the epimerase is normally suppressed, maintaining a high myo-inositol environment (myo/DCI ratio approximately 100:1 in follicular fluid) that supports FSH signaling and oocyte maturation.
In PCOS, the hyperinsulinemia drives chronic activation of the ovarian epimerase, accumulating D-chiro-inositol in the ovary at the expense of myo-inositol — the opposite of what oocytes need. Meanwhile, peripheral tissues that need active D-chiro-inositol-based IPG signaling become functionally insulin-resistant, partly because the epimerase response to insulin becomes blunted in those tissues. This is the "ovarian paradox" in PCOS: D-chiro-inositol is in excess where it harms (ovary) and deficient where it helps (muscle, liver).
This is why D-chiro-inositol alone is not adequate therapy for PCOS, and in some studies has been shown to worsen oocyte quality and ovarian function when given at supraphysiological doses. Combined therapy at the 40:1 ratio restores the natural plasma physiology: 4 grams of myo-inositol delivers enough substrate for both peripheral IPG-A signaling and ovarian myo-inositol supplementation, while the 100 mg of D-chiro-inositol provides peripheral IPG-P support without overloading the ovary.
The 40:1 Ratio and Its Physiological Basis
The 40:1 ratio of myo-inositol to D-chiro-inositol is based on the natural ratio of these two forms in healthy human plasma. The ratio was first characterized in pharmacokinetic studies in the 2000s and adopted as the design principle for combined-therapy products. The biological logic:
- Healthy plasma: approximately 40:1 myo:DCI
- Healthy follicular fluid: approximately 100:1 myo:DCI (oocytes need a high-myo environment)
- PCOS follicular fluid: ratio drops as low as 0.2:1 (D-chiro accumulates, myo depletes)
- PCOS plasma: ratio is variably reduced compared to healthy controls
A typical 40:1 product delivers 4,000 mg myo-inositol + 100 mg D-chiro-inositol per daily dose (usually split into 2 grams + 50 mg twice daily). This restores the physiological plasma ratio while providing adequate myo-inositol substrate to repair the depleted follicular environment.
The 40:1 standard has attracted scrutiny: the original pharmacokinetic study had only 32 participants, and other research has suggested that the actual plasma ratio in healthy women may be closer to 111:1. Despite this debate, the 40:1 formulation remains the most extensively studied combination, is endorsed by professional guidelines, and forms the basis of the largest PCOS trial dataset.
The Genazzani PCOS Trials
Alessandro Genazzani at the University of Modena has been one of the most prolific clinical investigators of inositol in PCOS, conducting a series of trials through the 2000s and 2010s that established many of the practical clinical parameters used today. Key Genazzani findings:
- Myo-inositol 4 g/day reduces LH:FSH ratio — the elevated LH characteristic of PCOS normalizes within 12 weeks, restoring proper follicular development signaling
- Free testosterone falls within 8-12 weeks — the reduction in compensatory hyperinsulinemia decreases ovarian androgen output and improves SHBG, lowering bioavailable testosterone
- Spontaneous ovulation returns in approximately 65% of treated women — one landmark Genazzani study reported a 65% ovulation rate at 6 months on myo-inositol + folic acid versus much lower rates with placebo or metformin alone
- Insulin sensitivity improves as measured by HOMA-IR — consistent reductions in fasting insulin and HOMA-IR across multiple trials, with effect sizes comparable to metformin
- Lean and overweight PCOS phenotypes both respond — Genazzani specifically studied the lean PCOS subgroup (often underserved by metformin) and demonstrated similar improvements
The Genazzani body of work was instrumental in moving inositol from "interesting nutraceutical" to "evidence-based first-line therapy" in European reproductive endocrinology practice.
Unfer Meta-Analysis & Costantino 2009
Costantino 2009
A landmark double-blind, placebo-controlled trial published in European Review for Medical and Pharmacological Sciences. PCOS patients received 4 g myo-inositol + 400 mcg folic acid daily versus placebo for 12-16 weeks. Outcomes measured included fasting insulin, HOMA-IR, LH, FSH, testosterone, androstenedione, glucose tolerance, and menstrual cycle regularity. Results showed statistically significant improvements across essentially all measured parameters in the inositol group, with no meaningful changes in placebo.
Unfer 2017 Meta-Analysis
The Unfer meta-analysis, published in Endocrine Connections, pooled randomized controlled trials of myo-inositol in PCOS through 2017. Findings:
- Statistically significant decrease in fasting serum insulin
- Statistically significant decrease in HOMA-IR
- Statistically significant decrease in LH levels
- Statistically significant decrease in FSH levels (with normalization of the LH:FSH ratio)
- Improvement in menstrual cycle regularity
- Improvement in spontaneous ovulation rate
- Favorable safety profile across all included trials
The Unfer meta-analysis provides Class I evidence for myo-inositol in PCOS — the same evidence level used to justify FDA drug approvals, though inositol is regulated as a dietary supplement.
Inositol vs Metformin Head-to-Head
Multiple head-to-head trials have compared myo-inositol (or combined MI/DCI at 40:1) against metformin in PCOS. The pooled finding across these trials:
- HbA1c reduction — comparable between the two interventions (both produce 0.3-0.5% reduction on average)
- HOMA-IR reduction — comparable, with some studies showing slightly greater reduction with combined MI/DCI
- Ovulation rate — often higher with myo-inositol than with metformin alone, particularly in lean PCOS patients
- Hyperandrogenism improvement — comparable for free testosterone reduction
- Tolerability — dramatically better with inositol. Metformin causes nausea, diarrhea, and abdominal cramping in 20-30% of patients (often dose-limiting); inositol GI side effects are mild and uncommon at the 4 g/day PCOS dose
- B12 depletion — metformin chronically depletes B12 through transporter interference; inositol does not
- Pregnancy compatibility — metformin is generally continued through the first trimester but practice varies; inositol has strong safety data for use throughout pregnancy and is actively beneficial for gestational diabetes prevention
The clinical bottom line: inositol matches metformin's metabolic benefits with substantially better tolerability and a clear advantage in fertility and pregnancy contexts. Many integrative endocrinologists now use inositol as the first-line insulin-sensitizing agent in PCOS, reserving metformin for cases where inositol alone is inadequate or unaffordable. Combination therapy with both is also well-tolerated and sometimes used in metabolically severe cases.
The 2023 International PCOS Guidelines
The 2023 International Evidence-Based PCOS Guidelines, produced by an international consortium including the Endocrine Society, the European Society of Endocrinology, ASRM, ESHRE, and patient advocacy groups, acknowledged the growing evidence base for inositol. The guidelines:
- Recognize inositol as a recommended option for women with PCOS
- Note its favorable safety profile across the lifespan
- Identify the 40:1 myo:DCI ratio as the most studied formulation
- Recommend continued research into live-birth outcomes and head-to-head comparisons
- Acknowledge that inositol may be preferred in patients who cannot tolerate metformin
The Pundir 2024 systematic review prepared in support of the guideline update concluded that inositol supplementation improves hormonal and metabolic parameters in PCOS and represents a reasonable evidence-based option for clinical use.
Practical Patient Protocol & Timeline
Standard PCOS protocol
- Dose: 4 g myo-inositol + 100 mg D-chiro-inositol daily (the 40:1 ratio), typically split as 2 g myo + 50 mg DCI twice daily
- Folic acid: add 400 mcg/day (200 mcg with each inositol dose) — particularly important for women trying to conceive
- Timing: with breakfast and dinner; the powder can be dissolved in water or juice
- Form: powder is the most common and economical form at this dose; capsules are available but require multiple pills per dose
- Duration: minimum 6 months for meaningful evaluation; many patients continue indefinitely
Month-by-month timeline
- Month 1: usually no perceptible change; some patients notice modest reduction in carbohydrate cravings
- Month 2-3: first menstrual cycle changes — cycle length may begin to regularize; some patients with prolonged amenorrhea have their first spontaneous period
- Month 3-4: improvements in insulin sensitivity become measurable (fasting insulin, HOMA-IR); modest improvements in acne and hirsutism may begin
- Month 4-6: ovulation often returns; LH:FSH ratio normalizes; free testosterone drops; mood and energy often improve
- Month 6-12: sustained improvements in metabolic and reproductive parameters; many women conceive during this window if trying
- Year 1+: maintenance phase; benefits persist as long as daily dosing continues; the supplement is safe long-term
If pregnancy occurs
Continue myo-inositol throughout pregnancy at the same 4 g/day dose. It reduces gestational diabetes risk by approximately 50% in high-risk women (notably women with PCOS), reduces preeclampsia risk, and supports continued metabolic health. Discontinue D-chiro-inositol component during pregnancy if guided to do so by your clinician (data on D-chiro use in pregnancy is more limited).
Beyond PCOS — Insulin Resistance & Metabolic Syndrome
The IPG-based mechanism is not unique to PCOS — insulin signaling operates the same way in non-PCOS insulin-resistant patients. Inositol benefits extend across the spectrum:
- Prediabetes / impaired fasting glucose — myo-inositol 2-4 g/day improves fasting glucose and oral glucose tolerance test results over 3-6 months
- Type 2 diabetes — D-chiro-inositol 1 g/day or combined MI/DCI improves HbA1c and HOMA-IR; works synergistically with metformin
- Metabolic syndrome in postmenopausal women — the landmark trial of myo-inositol 2 g twice daily for 1 year showed 20% of participants no longer met diagnostic criteria for metabolic syndrome at 1 year. Improvements occurred in blood pressure, fasting glucose, triglycerides, total cholesterol, and HDL
- Gestational diabetes prevention — multiple meta-analyses confirm approximately 50% reduction in GDM incidence in high-risk women receiving myo-inositol 2 g twice daily throughout pregnancy
- NAFLD (non-alcoholic fatty liver disease) — emerging data show improvements in hepatic steatosis with inositol supplementation, mechanistically linked to improved insulin sensitivity and reduced de novo lipogenesis
Patient FAQ
Q: How long until I notice changes in my cycles?
Most patients see the first cycle change at 2-3 months; ovulation often returns by 4-6 months. Some patients respond faster (1-2 months) and some slower (6+ months). Continue for at least 6 months before judging response.
Q: Do I need both myo-inositol and D-chiro-inositol, or just myo?
For PCOS specifically, the 40:1 combined formulation has the strongest evidence base and addresses both the peripheral insulin resistance (D-chiro effect) and the ovarian myo-inositol depletion (myo effect). Myo-only is also acceptable and effective — just continue 4 g/day. Avoid D-chiro-only or formulas with the wrong ratio (excessive D-chiro can worsen ovarian function).
Q: Can I take inositol with metformin?
Yes — the combination is well-tolerated and may produce additive benefits. Some patients use inositol to allow a lower metformin dose, reducing metformin's GI side effects while maintaining metabolic benefit.
Q: Can I take inositol while on birth control pills?
Yes — the combination is safe and inositol can address the underlying metabolic dysregulation that the pill is masking. If you stop the pill to try to conceive, continue inositol; the cycle-restoring effects often become apparent within 2-3 months of stopping the pill.
Q: Does inositol cause weight loss?
Not directly — it is not a weight-loss drug. But by improving insulin sensitivity, reducing carbohydrate cravings, and lowering compensatory hyperinsulinemia, it makes weight loss easier when combined with appropriate dietary changes. Many PCOS patients report 3-5 kg weight loss over 6-12 months with inositol plus diet.
Q: Will I have to take this forever?
The underlying genetic predisposition to PCOS does not change, so most patients benefit from continued supplementation indefinitely. After menopause, supplementation may still be useful for cardiovascular and metabolic protection.
Cautions Specific to PCOS Patients
- Hypoglycemia risk — if you are on insulin, sulfonylureas, or high-dose metformin, monitor blood glucose closely for the first 2-4 weeks. Inositol enhances insulin sensitivity and may lower glucose enough that medication doses need reduction.
- Combined oral contraceptives — safe to combine, but be aware that the pill masks PCOS rather than treating it. Long-term, addressing the metabolic root cause with inositol is preferable.
- Bipolar disorder caution (see related deep-dive) — inositol can theoretically trigger or worsen manic/hypomanic episodes in patients with bipolar disorder, even at the lower PCOS doses (4 g/day). If you have bipolar disorder and PCOS, use only with psychiatric supervision and watch for early mood elevation, decreased sleep need, or grandiose thinking.
- Trying to conceive — supplementation is beneficial, but combine with adequate folic acid (at least 400 mcg/day, ideally 800 mcg or methylfolate if MTHFR variant is present) and full pre-conception care.
- Use during pregnancy — myo-inositol continuation is safe and beneficial; D-chiro-inositol use during pregnancy has more limited data, so many clinicians switch to myo-only during pregnancy.
- Quality control — inositol supplements are not all equivalent. Look for products that specify USP-grade myo-inositol, the 40:1 ratio if combined, and third-party testing.
Key Research Papers
- Unfer V, Facchinetti F, Orrù B, Giordani B, Nestler J. (2017). Myo-inositol effects in women with PCOS: a meta-analysis of randomized controlled trials. Endocrine Connections, 6(8), 647-658. — PubMed
- Costantino D, Minozzi G, Minozzi F, Guaraldi C. (2009). Metabolic and hormonal effects of myo-inositol in women with polycystic ovary syndrome: a double-blind trial. European Review for Medical and Pharmacological Sciences, 13(2), 105-110. — PubMed
- Genazzani AD et al. Myo-inositol administration positively affects hyperinsulinemia and hormonal parameters in overweight PCOS patients. Gynecological Endocrinology. — PubMed
- Nordio M, Proietti E. (2012). The combined therapy with myo-inositol and D-chiro-inositol reduces the risk of metabolic disease in PCOS overweight patients compared to myo-inositol supplementation alone. European Review for Medical and Pharmacological Sciences, 16(5), 575-581. — PubMed
- Pundir J et al. (2024). Inositol for Polycystic Ovary Syndrome: A Systematic Review and Meta-analysis to Inform the 2023 Update of the International Evidence-based PCOS Guidelines. Journal of Clinical Endocrinology and Metabolism, 109(6), 1630-1645. — PubMed
- Bizzarri M, Carlomagno G. (2014). Inositol: history of an effective therapy for Polycystic Ovary Syndrome. European Review for Medical and Pharmacological Sciences, 18(13), 1896-1903. — PubMed
- Iuorno MJ et al. Effects of D-chiro-inositol in lean women with the polycystic ovary syndrome. Endocrine Practice. — PubMed
- Nestler JE et al. Ovulatory and metabolic effects of D-chiro-inositol in the polycystic ovary syndrome. New England Journal of Medicine. — PubMed
- Larner J. D-chiro-inositol — its functional role in insulin action and its deficit in insulin resistance. International Journal of Experimental Diabetes Research. — PubMed
- Showell MG et al. Inositol for subfertile women with polycystic ovary syndrome. Cochrane Database of Systematic Reviews. — PubMed
- Greff D et al. (2023). Inositol is an effective and safe treatment in polycystic ovary syndrome: a systematic review and meta-analysis of randomized controlled trials. Reproductive Biology and Endocrinology. — PubMed
PubMed Topic Searches
- PubMed: myo-inositol PCOS
- PubMed: 40:1 myo-inositol D-chiro-inositol ratio
- PubMed: inositol vs metformin PCOS
- PubMed: inositol phosphoglycan IPG
- PubMed: inositol metabolic syndrome
Connections
- Inositol Overview
- Inositol Benefits Hub
- Inositol for Anxiety & Panic
- Inositol for Fertility & Egg Quality
- Inositol for Bipolar & Depression
- PCOS
- Insulin Resistance
- Metabolic Syndrome
- Diabetes
- Gestational Diabetes
- Fasting Insulin
- Hemoglobin A1c
- Testosterone
- Folate (B9)
- Magnesium
- Acne
- All Vitamins
- Metformin — the standard insulin-sensitizing drug inositol is compared against in head-to-head PCOS trials.