Inositol for Fertility & Egg Quality
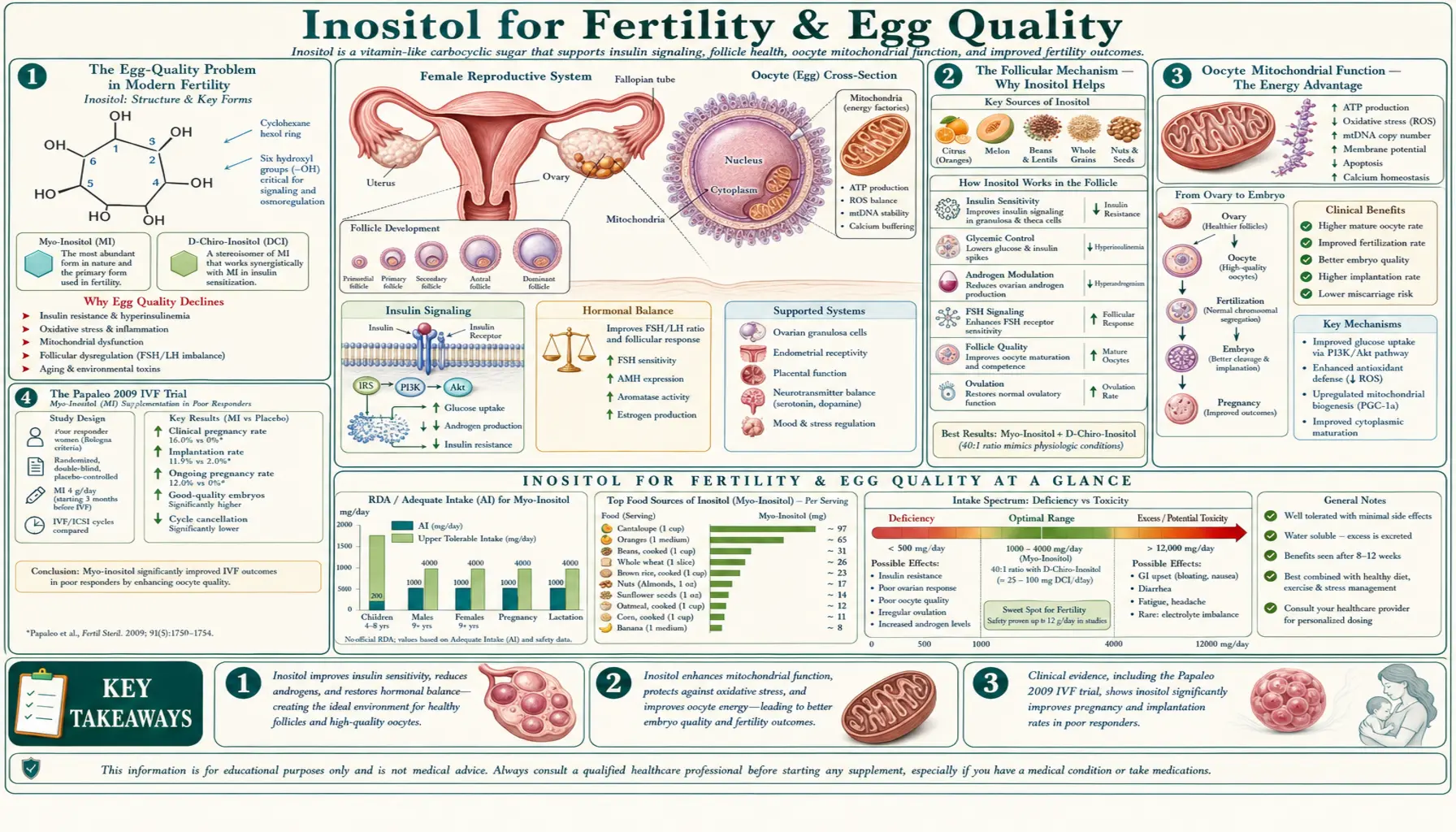
Myo-inositol is one of the most widely studied nutritional supplements in modern reproductive medicine. The Papaleo 2009 IVF trial established that 4 g/day myo-inositol starting one to three months before stimulation increases oocyte yield, raises the proportion of metaphase-II mature oocytes, and improves embryo quality scores. The Colazingari 2013 trial extended the evidence to combined myo + D-chiro-inositol at the 40:1 ratio. The Ghaemi 2024 systematic review of male fertility data confirmed improvements in sperm motility, DNA fragmentation, and testosterone. For advanced maternal age IVF, inositol pairs with melatonin, CoQ10, and DHEA in the canonical "fertility stack" that supports oocyte mitochondrial function and reduces the meiotic aneuploidy that defines age-related egg-quality decline. This deep-dive covers the IVF trials, the mitochondrial mechanism, male fertility, the pre-conception protocol, and the fertility-stack rationale.
Interactive Visualization Fertilization — follow the sperm and time the fertile window Watch 200 million sperm thin to a few hundred at the egg, harden the zona against the second one — then miss the window by two days and see nothing happen at all. Launch →
Table of Contents
- The Egg-Quality Problem in Modern Fertility
- The Follicular Mechanism — Why Inositol Helps
- Oocyte Mitochondrial Function
- The Papaleo 2009 IVF Trial
- Colazingari 2013 — Combined MI/DCI in IVF
- Male Fertility — Sperm Motility & DNA
- The Fertility Stack — Inositol + Melatonin + CoQ10 + DHEA
- Pre-Conception Protocol & Timeline
- IVF-Specific Timing & Coordination
- Patient FAQ
- Cautions for Fertility Patients
- Key Research Papers
- Connections
- Featured Videos
The Egg-Quality Problem in Modern Fertility
The defining challenge of modern reproductive medicine is the global trend toward delayed childbearing. The average age of first birth in developed countries has risen from 22-24 in the 1970s to 30-33 today. Beyond age 35, female fertility declines steeply — not because egg quantity has run out (typically a 35-year-old still has tens of thousands of oocytes in the ovarian reserve), but because egg quality deteriorates. The deteriorating egg quality manifests as:
- Meiotic spindle abnormalities — the chromosomes fail to segregate properly during meiosis, producing aneuploid embryos (extra or missing chromosomes). By age 40, more than 60% of embryos are aneuploid.
- Reduced mitochondrial function — the oocyte mitochondria accumulate damage over the decades the egg has been arrested in meiotic prophase I, reducing ATP production at the energy-intensive moments of fertilization and early embryo development.
- Increased reactive oxygen species — aged follicles show oxidative damage to mitochondrial DNA, lipids, and proteins critical for normal meiotic completion.
- Altered cytoplasmic environment — the follicular fluid environment changes with age, with shifts in inositol, glucose, amino acids, and growth factors that affect oocyte maturation.
Conventional IVF technology cannot "create" better eggs — it can only retrieve and select among the eggs that the woman's ovaries produce. This has driven enormous interest in nutritional interventions that might improve the quality of the available oocytes before retrieval. The two interventions with the strongest evidence base are inositol (for the follicular fluid environment and meiotic completion) and CoQ10 (for mitochondrial bioenergetics). Melatonin and DHEA are the third and fourth most commonly used.
The Follicular Mechanism — Why Inositol Helps
Inside the ovarian follicle, the oocyte is surrounded by cumulus cells and bathed in follicular fluid — a complex protein and metabolite mixture critical for normal oocyte maturation. In healthy reproductive-age women, follicular fluid contains a high concentration of myo-inositol, with the myo-to-D-chiro-inositol ratio approximately 100:1 (much higher than the plasma 40:1 ratio). This high-myo environment is essential for normal oocyte function:
- FSH receptor signaling — FSH stimulates the granulosa cells through a G-protein-coupled receptor that signals via the PIP2/IP3/calcium cascade, requiring adequate myo-inositol to support PIP2 regeneration
- Cumulus-oocyte communication — gap-junction signaling between cumulus cells and the oocyte depends on inositol-derived intracellular messengers
- Glucose metabolism in the cumulus complex — cumulus cells use glycolysis heavily during oocyte maturation, and myo-inositol participates in the glucose transporter signaling that supports this
- Calcium oscillations during fertilization — the sperm-induced calcium oscillations that activate the oocyte at fertilization are IP3-dependent and require adequate stored inositol
In PCOS and in older patients, the follicular fluid myo-inositol concentration is reduced and the myo/D-chiro ratio is disrupted. Supplemental myo-inositol restores the follicular fluid composition toward healthy levels, supporting the multiple inositol-dependent processes above. Studies have measured follicular fluid composition in women supplementing with myo-inositol vs not, and demonstrated meaningful shifts toward the healthy 100:1 ratio.
Oocyte Mitochondrial Function
The mature oocyte is the largest single cell in the human body, containing approximately 100,000 mitochondria — far more than any somatic cell. This enormous mitochondrial complement is necessary because fertilization, the first cell divisions, and embryo development through the morula stage rely entirely on maternal mitochondria (paternal mitochondria are excluded after fertilization). The energy demand at fertilization is enormous: calcium signaling, sperm-egg fusion, polar body extrusion, pronuclear formation, and the first mitotic division all require ATP from the oocyte's pre-existing mitochondrial population.
With age, oocyte mitochondria accumulate damage: mtDNA deletions, membrane potential decline, reduced ATP output, and increased reactive oxygen species. This is the primary cellular basis for age-related egg-quality decline. Several supplements address this mitochondrial decline:
- CoQ10 (ubiquinol form) — cofactor in the mitochondrial electron transport chain; supports ATP production. Multiple IVF trials at 200-600 mg/day show improved oocyte yield and embryo quality in older patients.
- Myo-inositol — supports the IP3/calcium signaling that activates oocyte mitochondria at fertilization; improves the follicular environment.
- Melatonin — powerful antioxidant that crosses into mitochondria; specifically protects oocyte mtDNA from oxidative damage. IVF trials at 3 mg/day show improved fertilization rates.
- DHEA — serves as substrate for ovarian steroidogenesis; may modestly improve oocyte yield in diminished ovarian reserve patients at 25 mg three times daily for 8-12 weeks before IVF.
- NAC, vitamin E, vitamin C — general antioxidant support for the follicular environment.
The complementary mechanisms (inositol for signaling, CoQ10 for ATP, melatonin for antioxidant defense, DHEA for steroidogenesis) form the rationale for combining these supplements in pre-IVF protocols.
The Papaleo 2009 IVF Trial
The Papaleo et al. 2009 trial, published in Gynecological Endocrinology, was the breakthrough study establishing inositol's role in IVF outcomes. Design and findings:
- Design: Randomized controlled trial in PCOS women undergoing IVF with ICSI. The active group received 4 g myo-inositol + 400 mcg folic acid daily, started in the cycle before stimulation. The control group received folic acid alone.
- Outcomes: Total oocytes retrieved, mature (metaphase II) oocytes, fertilization rate, embryo quality, clinical pregnancy rate.
- Results: The inositol group had:
- Higher number of total oocytes retrieved
- Higher proportion of mature MII oocytes
- Significantly reduced units of FSH stimulation required (less medication needed for similar response — an important practical and economic outcome)
- Higher clinical pregnancy rate (32.6% vs 24.3%, though sample size limited statistical power for this endpoint)
- Improved embryo quality scores
- Safety: No adverse events attributable to inositol; no impact on hormonal monitoring during stimulation.
The Papaleo trial established 4 g/day myo-inositol starting 1-3 months before IVF stimulation as the evidence-based pre-IVF protocol. Subsequent trials have replicated and extended these findings in PCOS and non-PCOS populations.
Colazingari 2013 — Combined MI/DCI in IVF
Colazingari et al. 2013, published in Archives of Gynecology and Obstetrics, addressed the question of whether the combined myo + D-chiro-inositol at the 40:1 ratio was superior to D-chiro-inositol alone for IVF outcomes. Design and findings:
- Design: PCOS patients undergoing IVF randomized to either combined therapy (4 g myo + 100 mg D-chiro daily) or D-chiro-only (1.1 g daily). Both groups received folic acid.
- Outcomes: Oocyte yield, MII oocytes, embryo quality, clinical pregnancy rate.
- Results: Combined therapy was superior to D-chiro-only across essentially all measured parameters. The combined group had more oocytes, more mature oocytes, better embryo quality, and higher clinical pregnancy rate.
The Colazingari trial reinforced the "ovarian paradox" concept: excessive D-chiro-inositol in the ovarian environment actually impairs oocyte quality, so supplementation must maintain the physiological 40:1 plasma ratio with myo-inositol as the dominant component. This is why D-chiro-only formulations are not appropriate for fertility applications even if the patient has PCOS.
Male Fertility — Sperm Motility & DNA
Male factor contributes to approximately 40-50% of infertility cases, yet receives much less attention in popular discussion. Male fertility is assessed through semen analysis measuring concentration (count), motility (movement), morphology (shape), and DNA fragmentation. Each parameter can be impaired by oxidative stress, environmental toxin exposure, varicocele, infection, and metabolic disease.
The Ghaemi et al. 2024 systematic review and meta-analysis (published in Food Science and Nutrition) pooled randomized controlled trials of myo-inositol supplementation in men with various forms of subfertility. Key findings:
- Total sperm motility — statistically significant improvement with myo-inositol supplementation
- Progressive sperm motility — statistically significant improvement (the most clinically meaningful motility parameter, as only progressively motile sperm can navigate the female reproductive tract)
- Sperm concentration — modest but significant improvement
- Sperm DNA fragmentation — significant reduction (an important marker, as high DNA fragmentation is associated with recurrent miscarriage and poor IVF outcomes)
- Serum testosterone — significant increase, particularly in men with subnormal baseline levels
- IVF/ICSI outcomes — some trials show improved fertilization rates and embryo quality when the male partner supplements with myo-inositol before sperm collection
Mechanistically, myo-inositol supports calcium signaling within sperm cells — essential for capacitation (the activation process sperm undergo in the female reproductive tract), the acrosome reaction (the membrane fusion that allows penetration of the egg), and ultimately fertilization. The supplementation protocol is typically 2 g twice daily for 3 months (corresponding to one full spermatogenesis cycle).
The Fertility Stack — Inositol + Melatonin + CoQ10 + DHEA
For advanced maternal age IVF (typically defined as ≥38 years) or for patients with diminished ovarian reserve, the canonical pre-IVF nutritional protocol — sometimes called the "fertility stack" — combines four supplements with complementary mechanisms:
| Supplement | Mechanism | Typical Dose |
|---|---|---|
| Myo-inositol | Follicular fluid composition; FSH signaling; oocyte maturation | 4 g/day (+ 100 mg D-chiro if PCOS) |
| CoQ10 (ubiquinol) | Mitochondrial ATP production in oocytes | 200-600 mg/day |
| Melatonin | Antioxidant protection of mtDNA in oocyte mitochondria | 3 mg at bedtime |
| DHEA | Substrate for ovarian steroidogenesis; potentially improves oocyte yield in DOR | 25 mg three times daily (start under clinician supervision) |
| Folic acid / methylfolate | DNA synthesis; methylation; neural tube defect prevention | 800 mcg/day (folate or 5-MTHF) |
| Vitamin D3 | Ovarian function; implantation; pregnancy outcomes | 2000-4000 IU/day (target 25(OH)D > 30 ng/mL) |
| Omega-3 EPA/DHA | Anti-inflammatory; cell membrane composition | 1000-2000 mg combined EPA+DHA/day |
This stack should be started at least 3 months before IVF stimulation — corresponding to the full duration of folliculogenesis (the process by which a primordial follicle becomes the dominant ovulatory follicle takes approximately 90 days). Supplementation started in the cycle of stimulation has less effect because the relevant follicles have already passed through most of their development.
For DHEA specifically, start under reproductive endocrinology supervision — some patients (particularly those with PCOS) should not take DHEA, and pre-treatment hormonal monitoring may be appropriate. For inositol and CoQ10, supplementation is essentially universal in advanced-age IVF protocols at reputable fertility centers.
Pre-Conception Protocol & Timeline
For women trying to conceive naturally
- Inositol: 4 g myo-inositol daily (+ 100 mg D-chiro if PCOS), with 400-800 mcg folic acid
- Start: at least 3 months before active trying
- Plus: prenatal multivitamin, omega-3, vitamin D as appropriate
- For PCOS-related anovulation: ovulation predictor kits to confirm cycles becoming regular; expect 3-6 months for full effect
- Continue: throughout the conception attempt and into pregnancy
For women planning IVF
- Inositol: 4 g myo (+ 100 mg D-chiro if PCOS); start 3 months before stimulation cycle
- CoQ10: 200-600 mg ubiquinol; start 3 months before stimulation
- Melatonin: 3 mg at bedtime; start 1-3 months before stimulation (some fertility specialists recommend stopping during the stimulation cycle, others continue throughout — follow your clinician's protocol)
- DHEA: only under clinician guidance; typically 25 mg three times daily for 8-12 weeks before stimulation in diminished ovarian reserve patients
- Folate, vitamin D, omega-3, prenatal multivitamin: standard
- Continue inositol through pregnancy: reduces gestational diabetes risk by ~50% in PCOS women
For male partners
- Myo-inositol: 2 g twice daily (4 g/day total); start 3 months before conception attempt (one full spermatogenesis cycle)
- Plus: CoQ10 200 mg/day, zinc 15-30 mg/day, selenium 100-200 mcg/day, L-carnitine 2 g/day, vitamin E 400 IU/day, vitamin C 500-1000 mg/day, omega-3 EPA/DHA 1000-2000 mg/day
- Lifestyle: avoid heat exposure to testes (saunas, hot tubs, laptops on lap); limit alcohol; stop smoking; avoid environmental toxins
IVF-Specific Timing & Coordination
Inositol can be continued throughout the IVF cycle — there is no interaction with the stimulation medications (gonadotropins, GnRH agonists/antagonists, hCG trigger). Some practical coordination notes:
- During stimulation: continue 4 g/day myo-inositol; some clinicians slightly increase the dose (to 6 g/day) during stimulation, others maintain the standard 4 g
- Day of retrieval: take morning dose before procedure; resume regular schedule the next day
- Embryo transfer: continue inositol; no interaction with progesterone support or other transfer-cycle medications
- Two-week wait through pregnancy test: continue inositol
- Positive pregnancy test: continue 4 g/day myo-inositol throughout pregnancy for gestational diabetes prevention and metabolic support
- Negative pregnancy test: continue inositol while planning next cycle; the supplement's benefit accumulates over multiple cycles
Patient FAQ
Q: I'm 38 and starting IVF in 4 months — what should I be doing now?
Start the fertility stack today: myo-inositol 4 g/day (with 100 mg D-chiro if you have PCOS), CoQ10 ubiquinol 400-600 mg/day, melatonin 3 mg at bedtime, folate 800 mcg/day, vitamin D 2000-4000 IU/day, omega-3 1000-2000 mg/day. Discuss DHEA with your reproductive endocrinologist (depends on AMH, antral follicle count, and other factors).
Q: Does my partner need to take anything?
Yes — sperm parameters significantly impact IVF success and a 3-month male preconception protocol can meaningfully improve outcomes. Myo-inositol 4 g/day, CoQ10 200 mg/day, zinc, selenium, L-carnitine, vitamin E, vitamin C, omega-3 as listed above.
Q: I have PCOS — should I take combined myo + D-chiro for IVF?
Yes — combined therapy at the 40:1 ratio (4 g myo + 100 mg D-chiro) is the preferred approach for PCOS patients undergoing IVF. Avoid D-chiro-only or formulas with excess D-chiro — supraphysiological D-chiro impairs oocyte quality.
Q: Will inositol increase my risk of multiples?
Not directly. The slight improvement in stimulation response may allow some patients to require slightly less FSH, but the number of mature follicles is closely monitored and managed by your clinician through dose adjustments and cycle cancellation if needed.
Q: Can I take it while breastfeeding after delivery?
Yes — inositol is a normal component of breast milk and supplementation while breastfeeding is considered safe.
Q: How much improvement should I expect?
Effects are real but modest at the population level. In meta-analyses, inositol improves oocyte yield by 20-30%, mature oocyte proportion by 5-15%, and clinical pregnancy rate by 5-10 percentage points. For an individual patient, the effect may be larger or smaller. The risk-benefit is highly favorable given the safety profile.
Cautions for Fertility Patients
- Bipolar disorder caution — even at the 4 g/day fertility dose, inositol can theoretically precipitate mania or hypomania in vulnerable individuals. If you have a personal or strong family history of bipolar disorder, discuss with your psychiatrist and reproductive endocrinologist before starting. Pregnancy itself is a high-risk time for mood episodes; mood stability planning is essential.
- D-chiro-inositol caution in non-PCOS fertility patients — if you do not have PCOS, myo-inositol alone is preferred. The D-chiro component is specifically beneficial for the PCOS metabolic phenotype and may not add value (or could theoretically harm follicular environment) in non-PCOS patients.
- Pregnancy continuation — myo-inositol continuation throughout pregnancy is well-studied and safe. D-chiro continuation has less safety data; many clinicians transition to myo-only during pregnancy out of caution.
- Coordination with reproductive endocrinology — tell your reproductive endocrinologist what you are taking. While inositol does not interfere with stimulation protocols, your clinician should know the full picture for hormone monitoring and protocol adjustment.
- Quality assurance — for fertility applications, use USP-grade myo-inositol from a reputable manufacturer. Third-party testing is a plus.
- Hypoglycemia in PCOS patients with diabetes meds — if you are on metformin or insulin, monitor blood glucose for the first 2-4 weeks of inositol supplementation.
- Realistic expectations — inositol improves but does not transform fertility outcomes. It is a meaningful intervention, particularly in PCOS and advanced maternal age contexts, but is not a substitute for medical evaluation and treatment of underlying causes of infertility.
Key Research Papers
- Papaleo E, Unfer V, Baillargeon JP, De Santis L, Fusi F, Brigante C, Marelli G, Cino I, Redaelli A, Ferrari A. (2009). Myo-inositol in patients with polycystic ovary syndrome: a novel method for ovulation induction. Gynecological Endocrinology. — PubMed
- Colazingari S, Treglia M, Najjar R, Bevilacqua A. (2013). The combined therapy myo-inositol plus D-chiro-inositol, rather than D-chiro-inositol, is able to improve IVF outcomes. Archives of Gynecology and Obstetrics, 288(6), 1405-1411. — PubMed
- Ghaemi SR, et al. (2024). The effect of myo-inositol on improving sperm quality and IVF outcomes: A systematic review and meta-analysis. Food Science and Nutrition, 12(12), 9573-9587. — PubMed
- Unfer V, Carlomagno G, Rizzo P, Raffone E, Roseff S. (2011). Myo-inositol rather than D-chiro-inositol is able to improve oocyte quality in intracytoplasmic sperm injection cycles. European Review for Medical and Pharmacological Sciences. — PubMed
- Tamura H et al. Melatonin and the ovary: physiological and pathophysiological implications. Fertility and Sterility. — PubMed
- Bentov Y, Casper RF. The aging oocyte — can mitochondrial function be improved? Fertility and Sterility. — PubMed
- Gleicher N, Weghofer A, Barad DH. Dehydroepiandrosterone (DHEA) reduces embryo aneuploidy. Reproductive Biology and Endocrinology. — PubMed
- Lerchbaum E et al. Myo-inositol supplementation in andrology patients. European Journal of Endocrinology. — PubMed
- Condorelli RA et al. Myoinositol: does it improve sperm mitochondrial function and sperm motility? Urology. — PubMed
- D'Anna R, Di Benedetto V, Rizzo P, Raffone E, Interdonato ML, Corrado F, Di Benedetto A. (2012). Myo-inositol may prevent gestational diabetes in PCOS women. Gynecological Endocrinology. — PubMed
- Brown J, Crawford TJ, Alsweiler J, Crowther CA. (2016). Dietary supplementation with myo-inositol in women during pregnancy for treating gestational diabetes. Cochrane Database of Systematic Reviews. — PubMed
PubMed Topic Searches
- PubMed: myo-inositol IVF oocyte quality
- PubMed: myo-inositol sperm male fertility
- PubMed: CoQ10 ubiquinol IVF aged oocyte
- PubMed: melatonin IVF oocyte fertilization
- PubMed: DHEA diminished ovarian reserve IVF
Connections
- Fertilization: How Sperm Meets Egg — interactive animation
- Inositol Overview
- Inositol Benefits Hub
- Inositol for PCOS & Insulin Sensitivity
- Inositol for Anxiety & Panic
- Inositol for Bipolar & Depression
- PCOS
- Gestational Diabetes
- CoQ10
- Melatonin
- Folate (B9)
- Vitamin D
- Zinc
- Selenium
- L-Carnitine
- Testosterone
- Preeclampsia
- All Vitamins