Rapamycin Side Effects and Monitoring
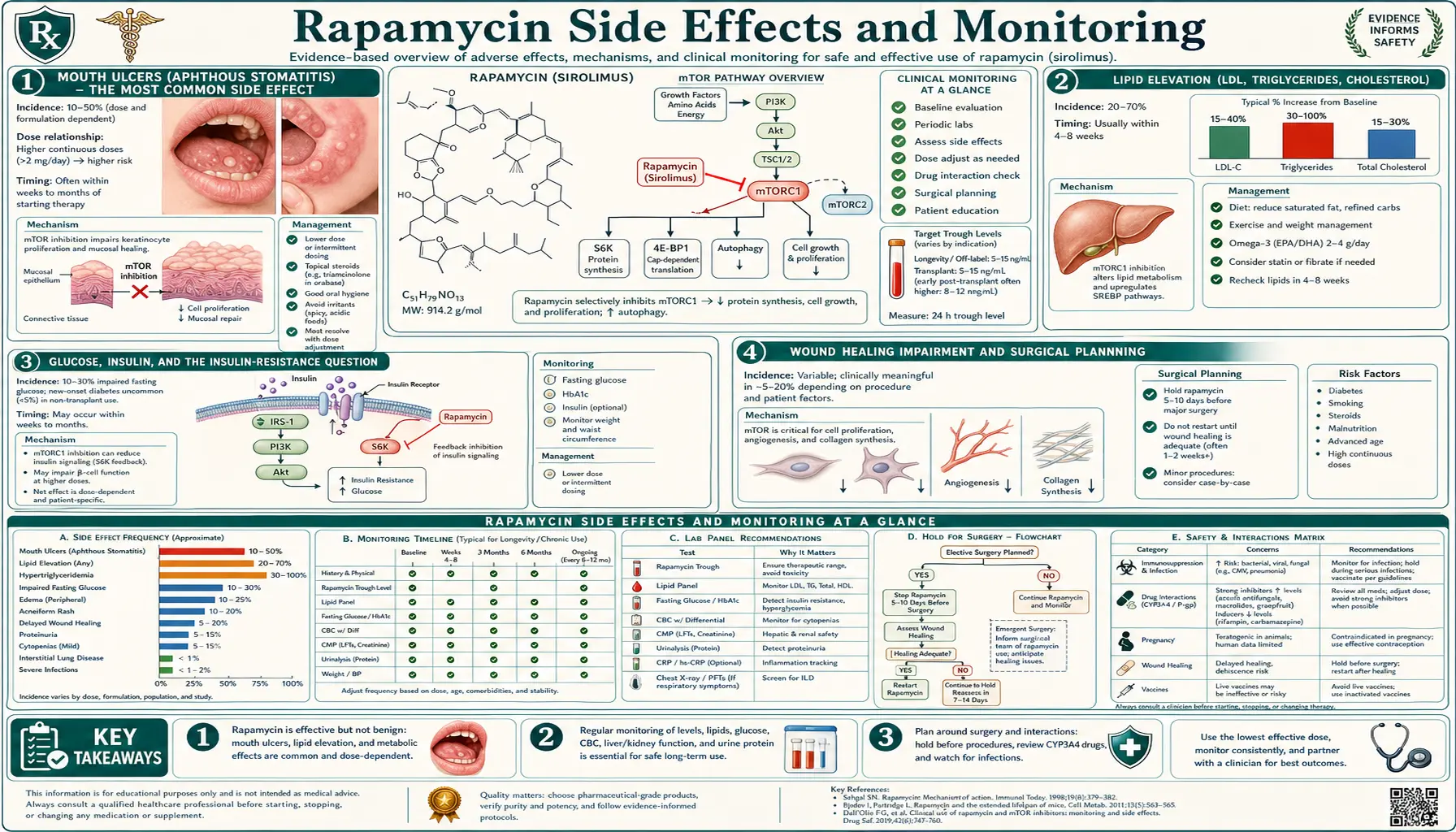
The side-effect profile of rapamycin is well characterized from two decades of transplant medicine and from the much shorter off-label longevity experience. The two profiles differ substantially because the doses differ by an order of magnitude. At transplant doses (2-5 mg daily, trough 5-15 ng/mL), serious side effects are common: significant immunosuppression with infection risk, new-onset diabetes, dyslipidemia requiring statin therapy, impaired wound healing, proteinuria, hematologic suppression, and interstitial pneumonitis. At off-label longevity doses (5-7 mg once weekly), the side-effect spectrum is much narrower and almost entirely manageable: mouth ulcers (the most common, dose-dependent), mild lipid elevation, the theoretical infection risk that has not been borne out at low intermittent dosing, and the pre-surgical wound-healing concern that requires temporary pause around any planned procedure. This page covers the full side-effect spectrum, the lab monitoring schedule appropriate for off-label longevity use, the red-flag symptoms that warrant pause or discontinuation, and the contraindications that should preclude rapamycin use entirely.
Table of Contents
- Mouth Ulcers (Aphthous Stomatitis) — The Most Common Side Effect
- Lipid Elevation (LDL, Triglycerides, Cholesterol)
- Glucose, Insulin, and the Insulin-Resistance Question
- Wound Healing Impairment and Surgical Planning
- Infection Risk and Immune Function at Low Doses
- Hematologic Effects (Anemia, Thrombocytopenia)
- Renal Function and Proteinuria
- Pulmonary Side Effects (Interstitial Pneumonitis — Rare at Low Dose)
- Cancer Risk — Net Effect Likely Protective
- Recommended Monitoring Schedule
- Red-Flag Symptoms Warranting Pause or Discontinuation
- Absolute and Relative Contraindications
- Key Research Papers
- Connections
- Featured Videos
Mouth Ulcers (Aphthous Stomatitis) — The Most Common Side Effect
Aphthous stomatitis — the painful round oral ulcers commonly called "canker sores" — is the single most common side effect of low-dose intermittent rapamycin, reported by 20-35% of off-label users at some point during treatment. The ulcers appear on the buccal mucosa, lateral tongue, soft palate, and gingival surfaces, typically 24-72 hours after a dose. They range from a single small lesion (under 5 mm, healing in a few days without treatment) to multiple painful ulcers that interfere with eating.
The mechanism appears to involve mTORC1 inhibition of the rapidly proliferating basal epithelial cells of the oral mucosa, which depend on high translational activity to maintain the turnover that keeps the mucosa intact. Reduced epithelial proliferation transiently exposes the underlying lamina propria, producing the characteristic ulceration. The same mechanism explains why oral mucositis is a well-known side effect of high-dose chemotherapy and of other mTOR inhibitor classes (everolimus, temsirolimus).
Practical management:
- Topical steroids — triamcinolone acetonide 0.1% dental paste applied directly to lesions, 3-4x daily, accelerates healing.
- Magic mouthwash compounds — various pharmacy-compounded rinses (diphenhydramine + lidocaine + Maalox; or dexamethasone-based) provide symptomatic relief.
- Salt-water rinses — warm saline rinses 3-4x daily help.
- Avoid acidic and spicy foods — tomatoes, citrus, vinegar, spicy peppers irritate active lesions.
- L-lysine supplementation — some anecdotal benefit; 1-2 g daily during active lesions.
- Dose reduction — if mouth ulcers recur consistently with each dose, the most reliable solution is to reduce the dose (e.g., from 6 mg/week to 4 mg/week). Most users find their personal ceiling for ulcer-free dosing.
Ulcers that develop on the first 1-2 doses sometimes do not recur with subsequent dosing — tolerance can develop. Persistent or worsening ulcers despite dose reduction warrant pause and reassessment.
Lipid Elevation (LDL, Triglycerides, Cholesterol)
Rapamycin elevates fasting lipids in a dose-dependent fashion. The mechanism is multifactorial: mTORC1 regulates SREBP1c (a master lipid biosynthesis transcription factor), and mTORC2 regulates lipoprotein receptor expression. At transplant doses, total cholesterol can rise 30-60 mg/dL, triglycerides can double, and LDL elevation often requires statin therapy. At off-label longevity doses, the elevations are smaller but still measurable in many users:
- Total cholesterol increase: typically 10-25 mg/dL
- LDL increase: typically 5-20 mg/dL
- Triglyceride increase: typically 20-50 mg/dL (more variable; some users see no change)
- HDL: little change in most users
Management strategies:
- Diet optimization — reduction in saturated fat, increase in soluble fiber, increase in omega-3 fatty acids. Some users see normalization of lipids with focused dietary changes alone.
- Statin therapy — rosuvastatin or pravastatin preferred (not metabolized through CYP3A4, no interaction concerns). Atorvastatin and simvastatin are CYP3A4 substrates and interact with rapamycin; if used, separate dosing day from rapamycin.
- Ezetimibe — non-statin LDL-lowering option, no significant interaction with rapamycin.
- EPA/DHA omega-3 supplementation — reduces triglycerides effectively at 2-4 g/day EPA+DHA combined.
- Bempedoic acid — non-statin LDL-lowering option for statin-intolerant patients, no interaction concerns.
- Dose reduction — if lipid elevation is the dominant side effect, reducing the rapamycin dose is often more effective than adding lipid-lowering therapy.
Important nuance: in transplant populations, the lipid elevation from sirolimus is associated with increased cardiovascular event risk and is treated aggressively. In off-label longevity populations, the elevations are much smaller, and there is no established outcome data on whether they translate to increased event risk. Most clinicians treat the elevation conservatively (target LDL appropriate to the patient's overall cardiovascular risk) but recognize that the situation is not directly analogous to the transplant data.
Glucose, Insulin, and the Insulin-Resistance Question
Daily continuous rapamycin produces measurable insulin resistance in transplant patients, with a meaningful incidence of new-onset diabetes (5-10% over the first year, depending on the population). The mechanism is the chronic mTORC2 depletion described in the mTOR Inhibition Mechanism deep-dive — loss of AKT Ser473 phosphorylation impairs insulin-stimulated GLUT4 trafficking and downstream insulin signaling.
The intermittent low-dose longevity regimen is hypothesized to spare mTORC2 substantially. Available human data suggests this hypothesis is largely correct:
- Kraig 2018 safety trial: no significant new-onset glucose dysregulation in healthy older adults on 1 mg daily for 8 weeks
- Mannick 2014: no significant glucose changes in low-dose RAD001 elderly cohort
- Off-label cohort data: most users do not develop significant new insulin resistance; some do
Monitoring should include fasting glucose (or HbA1c) and ideally fasting insulin at baseline and every 6 months. Calculate HOMA-IR ([fasting insulin in mU/L] x [fasting glucose in mg/dL] / 405; values <2.0 indicate good insulin sensitivity, 2.0-3.0 moderate, >3.0 increased resistance). Any progressive rise in HOMA-IR warrants discussion about dose reduction, dose interval extension, or addition of insulin-sensitizing interventions (metformin, exercise intensification, time-restricted eating).
Subset of users particularly at risk: those with pre-existing prediabetes, family history of type 2 diabetes, high baseline BMI, sedentary lifestyle, or polycystic ovary syndrome. For these populations, more conservative starting doses (3-5 mg/week) and more frequent monitoring (quarterly HbA1c and fasting insulin) are reasonable.
For related metabolic biomarker context, see our HbA1c page, Fasting Insulin page, and Insulin Resistance page.
Wound Healing Impairment and Surgical Planning
Rapamycin impairs wound healing by suppressing the mTORC1-driven cellular proliferation and protein synthesis required for tissue repair. In transplant medicine, this is a well-documented complication: wound dehiscence, lymphocele, anastomotic complications, and delayed surgical-site healing are all increased in patients on continuous sirolimus. Per Nashan and colleagues (2012), the wound healing complication rate in renal transplant patients on sirolimus is roughly 2-3x baseline.
At off-label intermittent low doses, the wound-healing impairment is smaller but real. Practical implications:
- Elective surgery planning. Pause rapamycin 1-2 weeks before any elective surgical procedure and resume 2 weeks after. For major surgery (orthopedic joint replacement, abdominal procedures, cardiac surgery), extend the pause to 4 weeks on either side.
- Dental procedures. Simple extractions or cleanings rarely require a pause. Implant placement, periodontal surgery, or root canal procedures should follow the 1-2 week pause protocol.
- Skin biopsies and dermatologic procedures. Minor punch biopsies are generally fine on rapamycin. Mohs surgery and larger excisions warrant 1-2 week pause.
- Emergency surgery. Notify the surgical team of recent rapamycin use. The wound-healing effect persists for several weeks after the last dose due to the long half-life and intracellular accumulation.
- Wound assessment. Any new wound (laceration, abrasion, surgical site) should be inspected regularly during rapamycin use for delayed closure or signs of infection.
Infection Risk and Immune Function at Low Doses
At transplant doses (continuous immunosuppression), rapamycin produces clinically significant immunosuppression with measurable increases in bacterial, viral, and fungal infection. Opportunistic infections (Pneumocystis pneumonia, CMV reactivation, BK virus nephropathy) are well-documented complications of transplant immunosuppression regimens including sirolimus.
At off-label intermittent low doses, the infection risk profile is qualitatively different. The Mannick 2018 trial showed reduced (not increased) laboratory-confirmed respiratory infections in elderly subjects on low-dose RTB101 over the year of follow-up. This counterintuitive finding likely reflects the mTORC1-driven rejuvenation of immune function (improved naive T-cell output, reduced exhausted T-cell burden, restored response to vaccination) outweighing any negligible immunosuppressive effect at the low dose.
Practical implications:
- Routine respiratory illnesses (common cold, mild influenza) do not require special management; symptomatic care as usual
- For any infection requiring antibiotic, antiviral, or antifungal therapy, pause rapamycin until resolution plus 1 week
- Standard vaccinations are generally compatible; the Mannick data even suggest enhanced response
- Live vaccines (yellow fever, oral typhoid, varicella in non-immune adults) warrant a pause around vaccination as a conservative default, though direct human data on this is limited at intermittent low doses
- Travel to areas with high infection risk (malaria-endemic areas, tropical destinations with food/water safety concerns) warrants discussion with the prescribing physician; the immune-status implications are likely minimal at intermittent low dose but practical caution applies
The unresolved question is whether long-term intermittent rapamycin use affects susceptibility to specific pathogens that aged immune systems handle poorly (varicella zoster reactivation, late-life pneumococcal disease, tuberculosis reactivation in those with prior exposure). Available data does not support a significant increase, but the data is from short-term trials only.
Hematologic Effects (Anemia, Thrombocytopenia)
Sirolimus suppresses hematopoiesis to varying degrees, with thrombocytopenia (low platelets) and anemia (low hemoglobin) being the most common manifestations. At transplant doses, these can be clinically significant. At off-label low intermittent doses, the effects are usually mild and may not require intervention:
- Mild anemia — hemoglobin drop of 0.5-1.5 g/dL is common, often without symptoms. If new anemia develops, check iron stores (ferritin, transferrin saturation), B12 and folate, and consider other causes.
- Mild thrombocytopenia — platelet count drop of 20-50% from baseline is occasionally seen, usually staying within or just below the normal range. Significant thrombocytopenia (<100k) warrants dose reduction or pause.
- Leukopenia — reductions in white blood cell count, particularly neutrophils, can occur at higher doses or with longer duration.
Routine CBC monitoring at baseline and every 6 months catches significant hematologic effects. New unexplained fatigue, easy bruising, prolonged bleeding from minor cuts, or persistent infection susceptibility should prompt an immediate CBC.
Renal Function and Proteinuria
Rapamycin can cause proteinuria, particularly in patients with pre-existing kidney disease or after kidney transplantation. The mechanism involves effects on podocyte function in the glomerulus. At transplant doses, clinically meaningful proteinuria affects 10-25% of patients depending on the underlying renal status.
At off-label intermittent low doses in patients with normal baseline kidney function, clinically significant proteinuria is uncommon. However, routine monitoring should include:
- Baseline assessment — serum creatinine, eGFR, urine protein:creatinine ratio or urinalysis with microalbumin
- Annual follow-up — same panel; investigate any significant change
- Higher-risk patients (pre-existing kidney disease, diabetes, hypertension, age >70) — consider more frequent monitoring and lower starting doses
Patients with stage 3b or worse chronic kidney disease (eGFR <45) are generally not good candidates for off-label rapamycin longevity use; the risk-benefit shifts unfavorably and there is little outcome data to support the practice.
Pulmonary Side Effects (Interstitial Pneumonitis — Rare at Low Dose)
Drug-induced interstitial pneumonitis is a rare but serious complication of all mTOR inhibitors (sirolimus, everolimus, temsirolimus). The mechanism is incompletely understood but appears to involve direct lung tissue toxicity at high cumulative exposure. Clinically, patients present with progressive dry cough, dyspnea on exertion, and characteristic ground-glass opacities on chest imaging. The condition is typically reversible with prompt drug discontinuation but can be fatal if not recognized.
Incidence in transplant populations on continuous sirolimus: 2-11% depending on definition and surveillance intensity. Incidence in off-label intermittent low-dose populations: not well characterized, but anecdotally very low. Case reports exist but no epidemiologic estimate is available.
Red-flag symptoms warranting immediate pause and pulmonary evaluation:
- New persistent dry cough lasting more than 1-2 weeks
- New unexplained shortness of breath, particularly on exertion
- Chest tightness or chest discomfort not attributable to cardiac or musculoskeletal causes
- Low-grade fever with respiratory symptoms
- Hypoxia on pulse oximetry
Evaluation should include chest imaging (CT preferred for the characteristic findings), pulmonary function testing, and ideally consultation with a pulmonologist familiar with drug-induced lung disease. Rapamycin should be discontinued pending evaluation.
Cancer Risk — Net Effect Likely Protective
The cancer-risk implications of rapamycin are complex and important to understand correctly:
- Transplant immunosuppression and skin cancer. Transplant patients on any immunosuppressive regimen have markedly increased rates of cutaneous squamous cell carcinoma, basal cell carcinoma, and Merkel cell carcinoma. Notably, sirolimus is associated with lower skin cancer rates than the calcineurin inhibitor regimens (cyclosporine, tacrolimus), making sirolimus the preferred immunosuppressive in transplant patients with prior skin cancer.
- mTOR inhibition and cancer biology. Hyperactive mTOR signaling is a hallmark of many cancers. Rapamycin and rapalogs (everolimus, temsirolimus) are FDA-approved for several cancer indications (renal cell carcinoma, neuroendocrine tumors, breast cancer with PI3K mutations).
- Mouse data. Rapamycin extends lifespan in cancer-prone mouse strains in part by reducing cancer incidence and progression.
- Cellular senescence and SASP. Rapamycin attenuates the senescence-associated secretory phenotype, which is a contributor to cancer progression through inflammatory signaling.
The integrated picture: at low intermittent doses in non-immunosuppressed adults, rapamycin's net effect on cancer risk is likely protective, not promoting. The strongest theoretical concern is the immunosuppression-related skin cancer signal seen at much higher transplant doses, but this is not borne out at low intermittent dosing in the available cohort data. Routine cancer-screening practices appropriate to age and risk profile should continue (mammography, colonoscopy, PSA, skin examination); no specific additional screening is indicated for off-label rapamycin users.
Important caveat: rapamycin is not a cancer treatment for the general population. Patients with active cancer should not start off-label rapamycin without explicit oncology consultation, since the drug's effects in the context of active malignancy depend on tumor biology and current treatment regimen.
Recommended Monitoring Schedule
A reasonable monitoring schedule for off-label longevity rapamycin use:
Baseline (before starting):
- Complete blood count (CBC) with differential
- Comprehensive metabolic panel (CMP) including creatinine, eGFR, liver enzymes
- Lipid panel (total, LDL, HDL, triglycerides; optionally ApoB and Lp(a))
- Hemoglobin A1c
- Fasting insulin (for HOMA-IR calculation)
- Urine protein:creatinine ratio or urinalysis with microalbumin
- TSH (thyroid function)
- Optionally: hs-CRP, ferritin, vitamin D, B12
- Comprehensive medication review for CYP3A4 / P-glycoprotein interactions
3 months after starting (or after each dose change):
- CBC, CMP, lipid panel
- Hemoglobin A1c if baseline was abnormal or trending
- Symptom review (mouth ulcers, wound healing, infection frequency, energy, fatigue)
Every 6 months on stable dose:
- CBC, CMP, lipid panel
- HbA1c and fasting insulin
- Urinalysis or urine protein:creatinine ratio (annually if normal at baseline)
- Symptom review including any concerning new respiratory symptoms
Annually:
- All of the above
- Age-appropriate cancer screening
- Dermatologic skin examination (particularly for patients with significant sun exposure history)
- Reassessment of dose, dose interval, and ongoing rationale for continued use
Optional advanced monitoring used by some longevity-focused practices:
- DNAm-based biological age clocks (Horvath, Hannum, GrimAge, PhenoAge) at baseline and annually
- Inflammatory markers panel (hs-CRP, IL-6, TNF-alpha)
- Comprehensive lipid analysis (ApoB, Lp(a), particle sizes via NMR)
- Body composition analysis (DEXA scan)
- Functional capacity assessment (VO2 max, grip strength, gait speed)
The advanced markers are research-grade and not validated as decision-making tools for individual patients. They may be useful for tracking longitudinal trends but should not drive dose adjustments in isolation from the standard clinical labs and symptom assessment.
Red-Flag Symptoms Warranting Pause or Discontinuation
The following symptoms warrant immediate pause of rapamycin and consultation with the prescribing physician:
- New persistent dry cough or unexplained dyspnea — rule out interstitial pneumonitis
- Severe or persistent mouth ulcers not responding to topical management within 2 weeks
- New unexplained bruising, bleeding, or fatigue — obtain CBC
- Significant unintentional weight loss — investigate
- Active infection requiring antibiotic, antiviral, or antifungal treatment — pause until resolution plus 1 week
- Any planned surgery — pause 1-2 weeks before; resume 2 weeks after (4 weeks for major surgery)
- New unexplained edema, particularly bilateral leg swelling — evaluate for renal, cardiac, or lymphatic causes
- Pregnancy or pregnancy intent — discontinue immediately and use reliable contraception
- Severe or progressive lipid elevation — manage with diet, statin, or dose reduction
- New or worsening glucose intolerance — consider dose reduction or alternative interventions
- Significant new proteinuria — evaluate cause
- Skin lesion that does not heal in expected time — consider drug-related wound impairment or new skin cancer
The principle: rapamycin is an elective intervention with a strong but incomplete evidence base. Any side effect that significantly impairs quality of life or signals serious physiologic disturbance is sufficient reason to pause and reassess. There is no clinical scenario in off-label longevity use where continuing rapamycin through a serious side effect is justifiable.
Absolute and Relative Contraindications
Absolute contraindications (rapamycin should not be used):
- Pregnancy or active attempt to conceive (rapamycin is teratogenic; pause 12+ weeks before conception attempt)
- Breastfeeding (drug excreted in milk)
- Active malignancy without explicit oncology consultation
- Active bacterial, viral, or fungal infection
- History of drug-induced interstitial pneumonitis from any mTOR inhibitor
- Hypersensitivity to sirolimus or any rapalog
- Advanced chronic kidney disease (eGFR <30) without specialist supervision
- Advanced liver disease (Child-Pugh C cirrhosis)
- Severe baseline thrombocytopenia or anemia
- Planned major surgery within 4 weeks
Relative contraindications (proceed with caution and individualized risk-benefit assessment):
- Diabetes mellitus or significant insulin resistance
- History of recurrent oral ulcers or aphthous stomatitis
- Concurrent use of CYP3A4-modulating medications (see drug interactions in the Dosing & Cycling deep-dive)
- Significant baseline dyslipidemia not at goal
- Chronic kidney disease stage 3 (eGFR 30-60)
- History of multiple skin cancers (basal cell, squamous cell)
- Age over 80 (risk-benefit less favorable; fewer years of potential benefit; greater vulnerability to side effects)
- Frailty syndrome
- Anticipated frequent surgical procedures (joint replacements, dental work, dermatologic procedures)
- Active inflammatory bowel disease in flare
- Severe baseline lymphopenia
For any patient with a relative contraindication, the decision to use off-label rapamycin should weigh the strength of the longevity evidence base against the specific increased risk in that individual. Many such patients can use rapamycin safely with appropriate dose reduction, more frequent monitoring, or specific risk-mitigation strategies. Some cannot, and alternative approaches to longevity optimization (caloric restriction, exercise, dietary protein optimization, sleep, stress management, metformin if diabetic, statin if dyslipidemic) may be more appropriate.
Key Research Papers
- Johnston O et al. (2008). Sirolimus is associated with new-onset diabetes in kidney transplant recipients. Journal of the American Society of Nephrology. — PubMed
- Pallet N, Legendre C (2013). Adverse events associated with mTOR inhibitors. Expert Opinion on Drug Safety. — PubMed
- Soefje SA et al. (2011). Common toxicities of mammalian target of rapamycin inhibitors. Targeted Oncology. — PubMed
- Mahe E et al. (2005). Cutaneous adverse events in renal transplant recipients receiving sirolimus-based therapy. Transplantation. — PubMed
- Nashan B, Citterio F (2012). Wound healing complications and the use of mammalian target of rapamycin inhibitors in kidney transplantation. Transplantation. — PubMed
- Morrisett JD et al. (2002). Sirolimus changes lipid concentrations and lipoprotein metabolism in kidney transplant recipients. Transplantation Proceedings. — PubMed
- Sofroniadou S, Goldsmith D (2011). Mammalian target of rapamycin inhibitors: hematological adverse effects. Drug Safety. — PubMed
- Lamming DW et al. (2012). Rapamycin-induced insulin resistance is mediated by mTORC2 loss and uncoupled from longevity. Science. — PubMed
- Kraig E et al. (2018). A randomized control trial to establish the feasibility and safety of rapamycin treatment in an older human cohort. Experimental Gerontology. — PubMed
- Mannick JB et al. (2018). TORC1 inhibition enhances immune function and reduces infections in the elderly. Science Translational Medicine. — PubMed
- Mancini M et al. (2018). Cutaneous adverse events of mTOR inhibitors: incidence, pathogenesis, and management. Critical Reviews in Oncology/Hematology. — PubMed
- Morath C et al. (2007). Sirolimus in renal transplantation. Nephrology Dialysis Transplantation. — PubMed
- Augustine JJ et al. (2007). Use of sirolimus in solid organ transplantation. Drugs. — PubMed
- Mahmood I (2010). Clinical pharmacology of sirolimus: a review. Clinical Pharmacokinetics. — PubMed
PubMed Topic Searches
- PubMed: Sirolimus adverse events
- PubMed: mTOR inhibitor mouth ulcers
- PubMed: mTOR pneumonitis
- PubMed: Sirolimus dyslipidemia
- PubMed: Rapamycin wound healing
Connections
- Rapamycin Overview
- Rapamycin Benefits Hub
- mTOR Inhibition Mechanism
- Longevity Evidence
- Dosing & Cycling
- Lipid Panel
- HbA1c
- Fasting Insulin
- Complete Blood Count
- Comprehensive Metabolic Panel
- Insulin Resistance
- Aphthous Ulcers / Canker Sores
- Interstitial Lung Disease
- Metformin
- Statins