Rapamycin and the mTOR Inhibition Mechanism
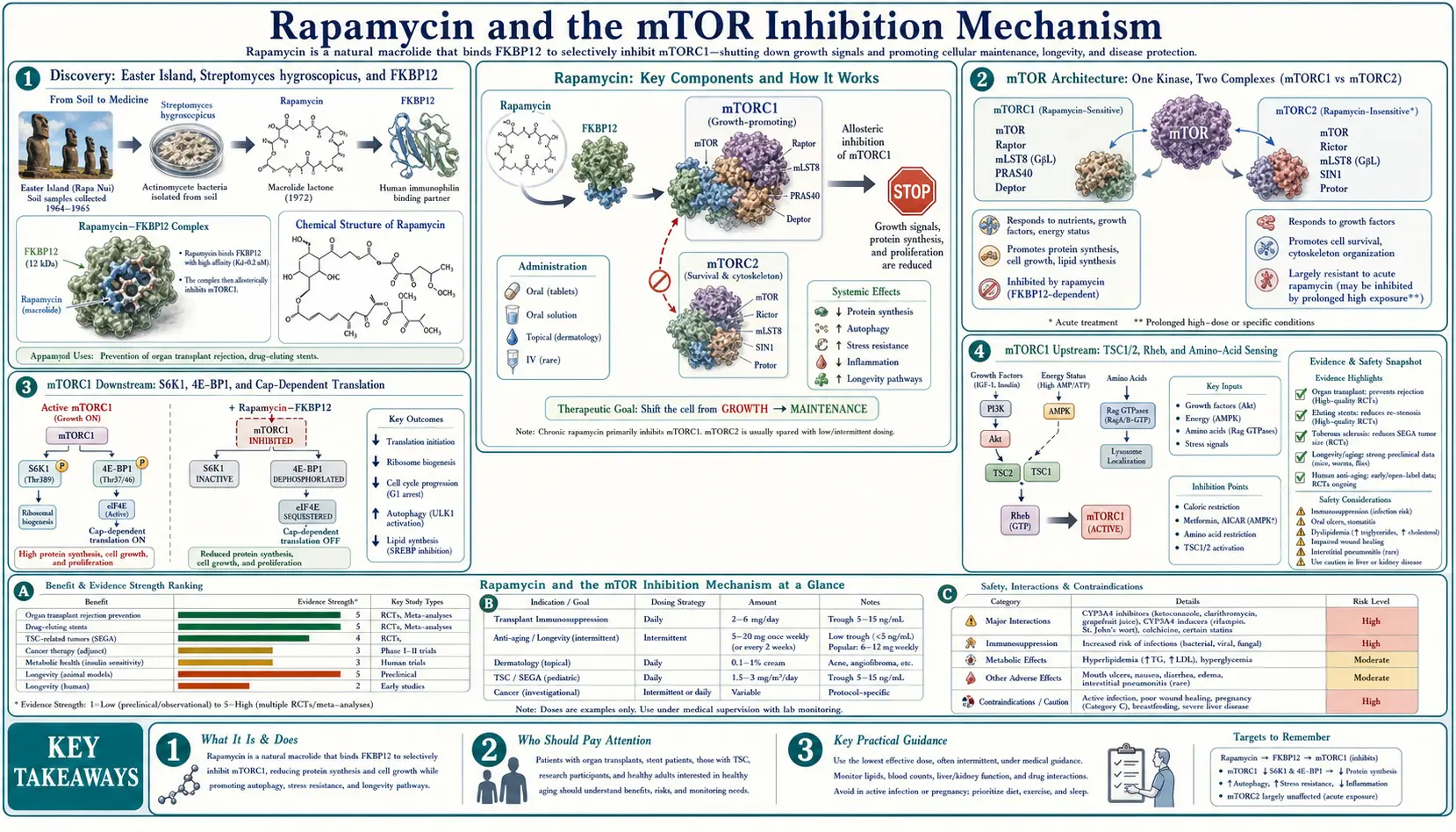
Rapamycin (sirolimus) is the prototypical and still the most important inhibitor of mechanistic Target of Rapamycin (mTOR), a serine/threonine protein kinase that integrates nutrient, growth-factor, energy, and oxygen signals and controls cellular decisions to either grow and divide (mTOR active) or to slow protein synthesis and recycle cellular components through autophagy (mTOR inhibited). Rapamycin does not bind mTOR directly. It first forms a complex with the cytosolic immunophilin FKBP12, and the FKBP12-rapamycin complex then docks onto the FRB (FKBP-rapamycin binding) domain of mTOR. The result is an allosteric inhibitor that selectively suppresses mTORC1 (the rapamycin-sensitive complex containing the scaffold protein Raptor) while sparing mTORC2 (the rapamycin-insensitive complex containing Rictor) — at least at short, intermittent exposures. The distinction between mTORC1 and mTORC2 is the single most important pharmacological fact for understanding why the same molecule can produce immunosuppression at one dose and putative geroprotection at another.
Table of Contents
- Discovery: Easter Island, Streptomyces hygroscopicus, and FKBP12
- mTOR Architecture: One Kinase, Two Complexes (mTORC1 vs mTORC2)
- mTORC1 Downstream: S6K1, 4E-BP1, and Cap-Dependent Translation
- mTORC1 Upstream: TSC1/2, Rheb, and Amino-Acid Sensing
- mTORC2 Effects: AKT, Insulin Signaling, and Why Chronic Dosing Differs
- Autophagy Induction via ULK1 Dephosphorylation
- Why Intermittent Dosing Matters: The mTORC2 Sparing Hypothesis
- Convergent Pathways: Why CR, Fasting, Metformin, and Rapamycin Look Alike
- Cellular Consequences: Senescence, Proteostasis, and Stem-Cell Function
- Key Research Papers
- Connections
- Featured Videos
Discovery: Easter Island, Streptomyces hygroscopicus, and FKBP12
Rapamycin's discovery is one of the more curious accidents of pharmaceutical history. In 1964, a Canadian expedition to Easter Island (Rapa Nui in the indigenous Rapanui language) collected soil samples as part of a survey of unusual microbial habitats. One sample, processed at Ayerst Research Laboratories in Montreal, yielded a previously unknown Streptomyces hygroscopicus strain producing an antifungal macrolide that was named rapamycin after the island. The compound's initial development as an antifungal was abandoned because of its potent immunosuppressive effect — an effect that turned out to be its eventual reason for approval.
The molecular target was unknown for nearly two decades. The breakthrough came in 1991 with the identification by Stuart Schreiber and Stanley Bishop's groups of FKBP12 (FK506-binding protein 12 kDa) as the cytosolic receptor that rapamycin binds first. Rapamycin alone does not inhibit mTOR; only the FKBP12-rapamycin complex does. This is why rapamycin pharmacology is so distinctive — the drug essentially requires a two-step recognition: first by FKBP12, then by the FRB domain on mTOR. The same FKBP12 binds tacrolimus (FK506), but the tacrolimus-FKBP12 complex inhibits calcineurin, not mTOR — explaining why two structurally similar macrolides have completely different mechanisms.
The mTOR kinase itself was identified independently by three groups in 1994 (Sabatini's RAFT1, Brown's mTOR, and Sabers' FRAP) using biochemical purification of the rapamycin-FKBP12 binding partner. The 2,549-amino-acid kinase turned out to be highly conserved, with clear orthologs in yeast (TOR1 and TOR2), worms, flies, plants, and all metazoans — one of the most ancient and conserved signaling molecules in eukaryotic biology.
mTOR Architecture: One Kinase, Two Complexes (mTORC1 vs mTORC2)
The mTOR kinase exists in cells as part of two functionally distinct multi-protein complexes:
- mTORC1 — contains mTOR, the scaffold protein Raptor (Regulatory-Associated Protein of mTOR), mLST8, PRAS40, and DEPTOR. Activated by amino acids (especially leucine and arginine), growth factors (via the PI3K-AKT axis), and cellular energy state (via AMPK and TSC1/TSC2). Phosphorylates two principal substrates: S6K1 (S6 kinase 1) and 4E-BP1 (eukaryotic translation initiation factor 4E binding protein 1). The functional output is increased protein synthesis, ribosome biogenesis, lipid synthesis, and cell growth; decreased autophagy. This is the complex rapamycin acutely inhibits.
- mTORC2 — contains mTOR, the scaffold protein Rictor (Rapamycin-Insensitive Companion of mTOR), mSIN1, mLST8, PROTOR, and DEPTOR. Activated by growth factors (primarily through ribosome association). Phosphorylates AKT at Ser473 (the activating hydrophobic motif phosphorylation), as well as SGK1 and PKC family kinases. The functional output is regulation of cytoskeleton, cell survival signaling, and insulin sensitivity. This complex is not acutely inhibited by rapamycin, but chronic exposure assembles a smaller fraction of newly synthesized mTOR into complete mTORC2 complexes, eventually reducing mTORC2 signaling as well.
The pharmacological selectivity for mTORC1 over mTORC2 occurs because the FKBP12-rapamycin complex binds to the FRB domain of mTOR, which lies between the kinase domain and the N-terminus. In assembled mTORC1, the FRB domain is accessible and the bound FKBP12-rapamycin physically obstructs substrate access to the kinase active site. In assembled mTORC2, the Rictor and mSIN1 subunits sterically occlude the FRB domain, so already-assembled mTORC2 is largely unaffected by rapamycin. However, mTOR-Rictor-mSIN1 assembly is dynamic, and during ongoing mTOR turnover the FRB domain is briefly exposed to cytosol — chronic rapamycin exposure captures the kinase in this transitional state and gradually depletes the pool of mature mTORC2 complexes. Sarbassov's 2006 Molecular Cell paper was the first to document this.
mTORC1 Downstream: S6K1, 4E-BP1, and Cap-Dependent Translation
The principal downstream effectors of mTORC1 are S6K1 and 4E-BP1. Both regulate protein translation, but through different mechanisms:
- S6K1 (p70 S6 Kinase 1) — phosphorylated by mTORC1 at Thr389 (the activating phosphorylation). Active S6K1 phosphorylates ribosomal protein S6 (giving it its name), eIF4B, eEF2K, and PDCD4. The functional output is increased translational efficiency particularly for mRNAs containing a 5' terminal oligopyrimidine (TOP) tract, which encode ribosomal proteins and other translation machinery components — an autocatalytic loop where increased S6K1 activity drives more ribosome production. S6K1 also negatively feeds back on IRS-1 (insulin receptor substrate 1), which is the principal molecular explanation for mTORC1-driven insulin resistance.
- 4E-BP1 (eIF4E Binding Protein 1) — hyperphosphorylated by mTORC1 at multiple sites (Thr37, Thr46, Ser65, Thr70). In its hypophosphorylated state, 4E-BP1 binds and sequesters eIF4E (the cap-binding initiation factor); hyperphosphorylation releases eIF4E to assemble with eIF4G and eIF4A into the eIF4F cap-binding complex that initiates cap-dependent translation. Cap-dependent translation is preferentially required for mRNAs with structured 5' UTRs encoding cell-cycle (cyclin D1, c-Myc) and pro-growth proteins.
The net effect of mTORC1 activation is a global shift in which mRNAs get translated — toward pro-growth, ribosomal, and biosynthetic transcripts, and away from autophagy and stress-response transcripts. Rapamycin reverses this shift. The mTORC1 inhibition is also more potent against 4E-BP1 phosphorylation at some sites than others, and is more potent against S6K1 than against 4E-BP1 — the so-called "incomplete" pharmacology of rapamycin compared to ATP-competitive mTOR inhibitors like Torin1 that block all mTORC1 substrate phosphorylation equally.
mTORC1 Upstream: TSC1/2, Rheb, and Amino-Acid Sensing
mTORC1 sits at the convergence of two major upstream input arms:
- Growth factor / energy state arm (via TSC1/TSC2 and Rheb). Growth factors (insulin, IGF-1, EGF) activate the PI3K-AKT pathway. Active AKT phosphorylates and inhibits the TSC1/TSC2 complex, which is a GTPase-activating protein for the small GTPase Rheb. Without TSC inhibition, Rheb stays in its GTP-bound active form and directly activates mTORC1 at the lysosomal membrane. AMPK, activated when cellular ATP is low, phosphorylates TSC2 in the opposite direction (activating it) and also directly phosphorylates Raptor — both effects inhibit mTORC1. This is the molecular reason why metformin (an AMPK activator) partly converges on the same mTORC1 inhibition that rapamycin produces.
- Amino-acid sensing arm (via Rag GTPases and Ragulator). Specific amino acids — leucine, arginine, methionine — signal mTORC1 activation through a parallel pathway involving the Rag GTPases (RagA/B and RagC/D heterodimers) and the lysosomal Ragulator complex. When amino acids are abundant, the Rag GTPases recruit mTORC1 to the lysosomal membrane where Rheb-GTP is waiting. Without amino acids, mTORC1 stays cytoplasmic and inactive even if Rheb-GTP is abundant.
The leucine sensor is Sestrin2, identified by Wolfson et al. in 2016. Sestrin2 directly binds leucine; when leucine is present, Sestrin2 releases its inhibitory grip on GATOR2 (which inhibits GATOR1, which is a GAP for the Rag GTPases). The net effect is that leucine availability is sensed as a Rag GTPase activation signal, which in turn recruits mTORC1 to the lysosome. This explains why high-leucine intake (BCAA supplements, large amounts of whey protein) is mTORC1-activating in a way that has been hypothesized to oppose the geroprotective effect of rapamycin — though this is not yet rigorously established in human clinical evidence.
For the related amino-acid signaling biology, see our Leucine page and Methionine page.
mTORC2 Effects: AKT, Insulin Signaling, and Why Chronic Dosing Differs
mTORC2 phosphorylates AKT at Ser473, which is required for full AKT activation (the other activating phosphorylation, Thr308, is performed by PDK1 downstream of PI3K). Active AKT then drives multiple downstream pathways: TSC2 inhibition (activating mTORC1 in a feed-forward loop), GSK3 inhibition (releasing glycogen synthase and beta-catenin), FOXO transcription factor inhibition (suppressing stress-response and apoptotic gene expression), and GLUT4 trafficking to the plasma membrane in response to insulin.
When chronic rapamycin exposure begins to deplete mTORC2 (the Sarbassov 2006 finding), AKT Ser473 phosphorylation drops, AKT activity falls, GLUT4 trafficking is impaired, and insulin-stimulated glucose uptake decreases — producing measurable insulin resistance. Lamming and colleagues (2012 Science) showed that this insulin-resistance phenotype could be dissociated from the longevity-extending effect of rapamycin in mice by tissue-specific genetic strategies: deleting mTORC2 in liver alone produced the metabolic phenotype, but lifespan extension was attributable to mTORC1 inhibition in other tissues.
The clinical translation of this finding underpins the entire intermittent-dosing strategy that defines off-label longevity use. If daily transplant-dose rapamycin produces both mTORC1 and (with time) mTORC2 inhibition, but lifespan extension requires only mTORC1 inhibition, then an intermittent regimen that pulses high mTORC1 inhibition periodically while allowing mTORC2 to recover between doses should in principle deliver the longevity benefit while sparing the metabolic toxicity. This is the molecular justification for the 5-7 mg-once-weekly regimens that dominate the off-label longevity literature — covered in the Dosing, Cycling, and Off-Label Use deep-dive.
Autophagy Induction via ULK1 Dephosphorylation
One of the most therapeutically interesting downstream effects of mTORC1 inhibition is the release of brake on autophagy — the lysosome-mediated degradation pathway that recycles damaged proteins, lipids, and organelles. Active mTORC1 directly phosphorylates ULK1 (Unc-51 Like Kinase 1) at Ser757, inhibiting its activity. ULK1 is the rate-limiting kinase that initiates autophagosome formation by phosphorylating ATG13, FIP200, and ATG14L. When mTORC1 activity drops — whether from amino-acid withdrawal, energy depletion (AMPK activation), or rapamycin treatment — ULK1 Ser757 dephosphorylates, ULK1 activates, and autophagy proceeds.
The geroscience interest in autophagy is substantial. Across multiple model organisms, longevity interventions (caloric restriction, fasting, rapamycin, methionine restriction) require functional autophagy to extend lifespan — if essential autophagy genes (ATG5, ATG7) are deleted, the lifespan extension disappears. Autophagy clears damaged mitochondria (mitophagy), aggregated proteins (linked to Alzheimer's, Parkinson's, and Huntington's pathology), and senescent organelles. The hypothesis is that the slow accumulation of damaged cellular contents over decades is a substantial component of aging itself, and that periodic stimulation of autophagy by intermittent fasting or by intermittent rapamycin treatment may slow that accumulation.
For the related dietary autophagy biology, see our pages on Intermittent Fasting and Caloric Restriction.
Why Intermittent Dosing Matters: The mTORC2 Sparing Hypothesis
The geroscience field's working hypothesis on intermittent rapamycin dosing rests on three pharmacokinetic and pharmacodynamic observations:
- Rapamycin has a long blood half-life (~62 hours in humans) — meaning that a single 5-7 mg dose produces multi-day exposure with measurable trough at one week, but trough levels well below the 5-15 ng/mL transplant target.
- mTORC1 inhibition is acute and reversible — even partial trough exposure produces meaningful mTORC1 suppression because the FKBP12-rapamycin complex acts allosterically on accessible mTORC1 in real time.
- mTORC2 depletion requires sustained exposure — chronic daily transplant dosing builds up enough sustained FKBP12-rapamycin in cytosol to capture freshly translated mTOR before it assembles into mature mTORC2. Pulsed weekly dosing, with five days of declining exposure between doses, allows mTORC2 to assemble normally most of the time.
The Arriola Apelo 2016 paper in Aging Cell tested this hypothesis directly in mice: an intermittent regimen (rapamycin every five days) produced lifespan extension in female C57BL/6J mice without inducing the insulin resistance or metabolic toxicity seen with daily continuous dosing. The Bitto 2016 paper in eLife showed that even a transient 90-day course of rapamycin in middle-aged mice produced lasting lifespan extension — suggesting the geroprotective effect may not require continuous treatment, just periodic mTORC1 pulses against a background of normal mTORC2 function.
The unresolved questions: optimal dosing interval (weekly versus every 10 days versus every 14 days), optimal dose (5 mg, 6 mg, 7 mg, or higher), whether cycling on and off (e.g., 3 months on / 1 month off) provides additional benefit, and whether co-administration with metformin or other mTORC1-relevant compounds is additive, redundant, or counterproductive. These are open empirical questions that the PEARL trial and the next-generation longevity cohort studies are designed to address.
Convergent Pathways: Why CR, Fasting, Metformin, and Rapamycin Look Alike
One of the most striking observations in geroscience is the molecular convergence of the major reproducibly-lifespan-extending interventions, all of which act in part through mTORC1 inhibition:
- Caloric restriction (CR) — reduced food intake reduces amino-acid signaling (especially leucine and methionine), reduces insulin and IGF-1 signaling, and elevates AMPK activity. All three converge on mTORC1 inhibition.
- Time-restricted eating / intermittent fasting — produces alternating mTORC1 cycling: high after meals, low during the fasted window. The fasted-period autophagy induction is thought to be the principal mechanism.
- Methionine restriction — methionine is one of the amino acids that directly signals mTORC1 via the SAMTOR sensor. Selective methionine restriction (without total caloric restriction) extends lifespan in rodents, presumably through this pathway.
- Metformin — activates AMPK indirectly via mitochondrial complex I inhibition. AMPK then phosphorylates and inhibits mTORC1. Also produces some direct effects on lysosomal mTORC1 assembly. The TAME trial is designed to test whether this translates to clinical benefit in humans.
- Acarbose — reduces postprandial glucose and insulin spikes, indirectly reducing mTORC1 activation. Independently established lifespan extension in mice in the ITP.
- Protein restriction / vegan and vegetarian diets — reduce amino-acid signaling. Compatible with the FGF21 elevation and lower IGF-1 seen in long-lived populations.
- Rapamycin — the most pharmacologically direct mTORC1 inhibitor, requiring none of the dietary or metabolic intermediates above.
The convergent-pathway picture is important because it suggests rapamycin and dietary interventions are partially redundant rather than additive. A person already practicing meaningful caloric restriction or intermittent fasting may capture much of the geroprotective benefit through diet, and rapamycin may add less than it would for a person eating an ad libitum Western diet. This is one of the practical considerations in deciding whether to add off-label rapamycin to a comprehensive longevity strategy. For comparison with other interventions in this convergent space, see our pages on Metformin, Intermittent Fasting, and Caloric Restriction.
Cellular Consequences: Senescence, Proteostasis, and Stem-Cell Function
Beyond the immediate effects on translation and autophagy, mTORC1 inhibition produces several downstream phenotypes relevant to the hallmarks of aging:
- Cellular senescence and the SASP — senescent cells (post-mitotic, metabolically active, secretory) accumulate with age and contribute to inflammaging via the senescence-associated secretory phenotype (SASP). mTORC1 signaling is required for the full SASP secretory program; rapamycin attenuates SASP without necessarily killing senescent cells, distinguishing it from senolytics (which clear senescent cells via apoptosis). The clinical implication is that rapamycin may reduce the inflammatory contribution of accumulated senescent cells.
- Proteostasis — the balance between protein synthesis (mTORC1-driven) and protein degradation (autophagy and ubiquitin-proteasome). Aging cells progressively accumulate misfolded and aggregated proteins. Reducing protein synthesis modestly while enhancing autophagy improves proteostasis. This is the molecular rationale for why mTORC1 inhibition may reduce risk of neurodegenerative disease, where misfolded protein aggregation is central.
- Stem-cell function — tissue-resident stem cells (intestinal, hematopoietic, neural, muscle satellite) lose proliferative capacity with age, in part through hyperactive mTORC1 driving them out of quiescence and into terminal differentiation or senescence. Rapamycin extends the proliferative capacity of stem-cell pools in multiple tissues.
- Mitochondrial function and mitophagy — mTORC1 inhibition activates PGC-1alpha-mediated mitochondrial biogenesis and increases turnover of damaged mitochondria via PINK1/Parkin-mediated mitophagy. The net effect over time is a younger-quality mitochondrial population.
- Immune-cell rejuvenation — this is the basis for the Mannick et al. 2014/2018 trials showing improved vaccine response in older adults treated with rapalogs. The mechanism is thought to involve clearance of senescent and exhausted T-cell populations and rejuvenation of naive T-cell output from the thymus.
Together, these cellular consequences are the molecular bridge between the abstract phrase "mTOR inhibition" and the observable phenotypes of slowed aging seen in animal models: maintained organ function, reduced age-related disease, better immune response, slower cognitive decline, and extended lifespan. The Longevity Evidence deep-dive walks through the species-by-species experimental evidence for each.
Key Research Papers
- Brown EJ et al. (1994). A mammalian protein targeted by G1-arresting rapamycin-receptor complex. Nature. — PubMed
- Sabatini DM et al. (1994). RAFT1: a mammalian protein that binds to FKBP12 in a rapamycin-dependent fashion. Cell. — PubMed
- Kim DH et al. (2002). mTOR interacts with raptor to form a nutrient-sensitive complex. Cell. — PubMed
- Sarbassov DD et al. (2006). Prolonged rapamycin treatment inhibits mTORC2 assembly and Akt/PKB. Molecular Cell. — PubMed
- Lamming DW et al. (2012). Rapamycin-induced insulin resistance is mediated by mTORC2 loss and uncoupled from longevity. Science. — PubMed
- Saxton RA, Sabatini DM (2017). mTOR Signaling in Growth, Metabolism, and Disease. Cell. — PubMed
- Wolfson RL et al. (2016). Sestrin2 is a leucine sensor for the mTORC1 pathway. Science. — PubMed
- Jung CH et al. (2009). ULK-Atg13-FIP200 complexes mediate mTOR signaling to the autophagy machinery. Molecular Biology of the Cell. — PubMed
- Sancak Y et al. (2008). The Rag GTPases bind raptor and mediate amino acid signaling to mTORC1. Science. — PubMed
- Inoki K et al. (2003). TSC2 mediates cellular energy response to control cell growth and survival. Cell. — PubMed
- Powers RW et al. (2006). Extension of chronological life span in yeast by decreased TOR pathway signaling. Genes & Development. — PubMed
- Kaeberlein M et al. (2005). Regulation of yeast replicative life span by TOR and Sch9 in response to nutrients. Science. — PubMed
PubMed Topic Searches
- PubMed: mTOR signaling pathway
- PubMed: Rapamycin FKBP12 FRB mechanism
- PubMed: ULK1 autophagy mTORC1
- PubMed: S6K1 4E-BP1 translation
- PubMed: mTORC2 Rictor AKT signaling
Connections
- Rapamycin Overview
- Rapamycin Benefits Hub
- Longevity Evidence
- Dosing & Cycling
- Side Effects & Monitoring
- Metformin (AMPK Activator)
- Berberine (AMPK Activator)
- Intermittent Fasting
- Caloric Restriction
- Leucine (mTORC1 Activator)
- Methionine (mTORC1 Activator)
- Arginine (mTORC1 Activator)
- Autophagy
- IGF-1 Testing
- Senolytics