Low-Dose Naltrexone (LDN): History and Origins
Low-dose naltrexone (LDN) has an unusually clear origin story for an off-label remedy: the parent drug, naltrexone, was a fully approved pharmaceutical, and the idea of using a tiny fraction of its normal dose to calm the immune system traces to one identifiable physician — Dr. Bernard Bihari (1931–2010), a Harvard-trained New York addiction specialist who first observed the effect in HIV/AIDS patients in 1985–1986. This page tells that story honestly: where naltrexone itself came from, who Bihari was, how he stumbled onto the low-dose effect, the laboratory science (the "opioid growth factor" work at Penn State) that later offered a possible mechanism, how patient communities and a UK charity spread the idea, and — just as important — what the controlled evidence actually shows. LDN is not FDA-approved for any of the autoimmune, pain, or chronic-illness conditions it is used for; it remains investigational. Where the record is firm we say so; where a claim is anecdote, theory, or still unproven, we name it as such.
Table of Contents
- Where Naltrexone Came From (1963–1984)
- Bernard Bihari: The Man Behind LDN
- The Discovery: AIDS and the 3 mg Observation
- From HIV to Autoimmunity and Cancer
- The Penn State Science: Opioid Growth Factor
- How LDN Spread: Patients, Pharmacies, and a Charity
- Evidence and Mainstream Reception
- Research Papers and References
- Connections
- Featured Videos
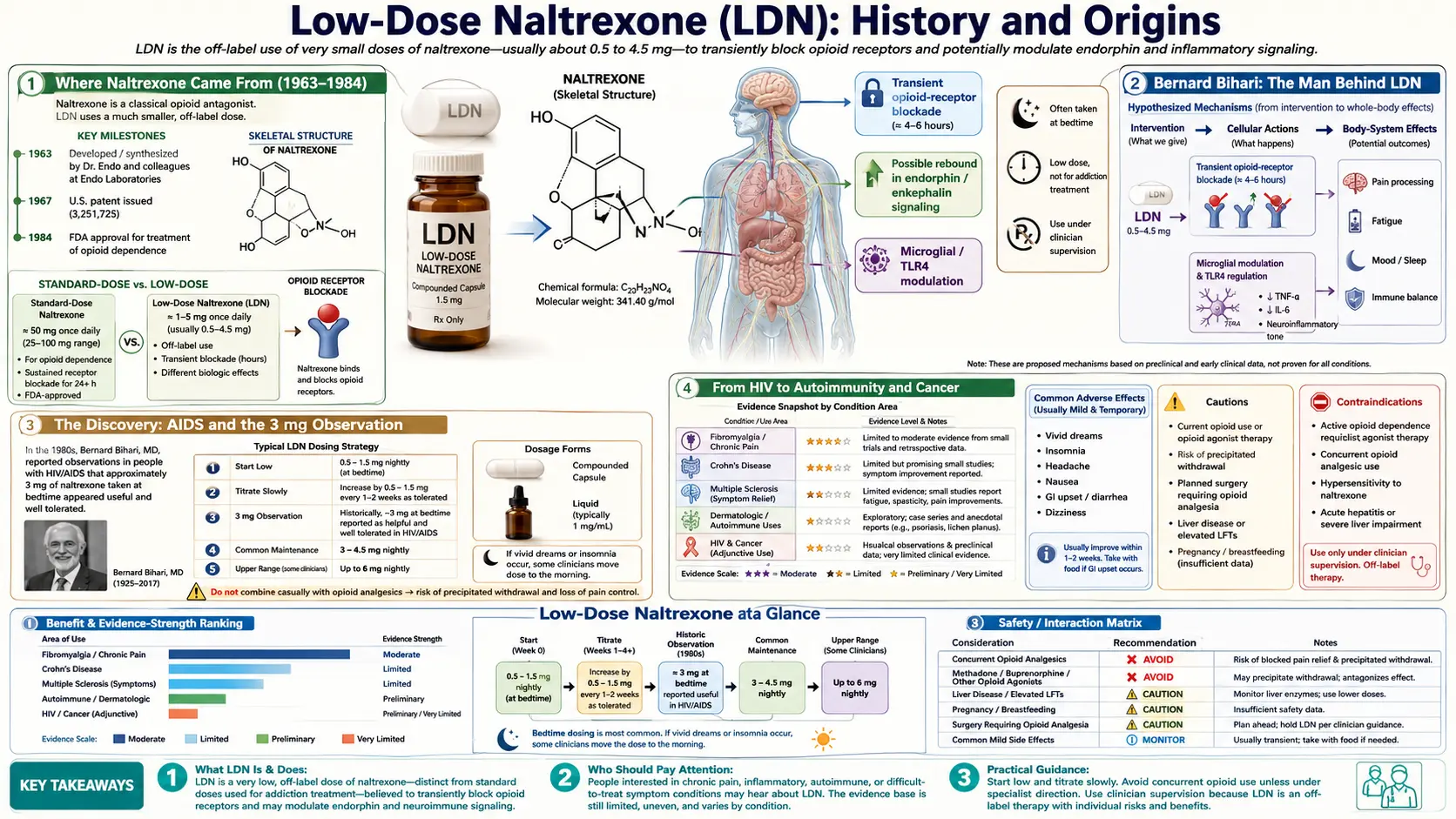
Where Naltrexone Came From (1963–1984)
The story begins not with low doses but with a conventional drug-development effort. Naltrexone was first synthesised in the early-to-mid 1960s at Endo Laboratories, a pharmaceutical company on Long Island, New York. The compound — carried under the laboratory code EN-1639A — was characterised as an orally active, long-acting, potent opioid antagonist, meaning it blocks opioid receptors rather than activating them. Endo patented it in 1967. In 1969, the larger chemical firm DuPont acquired Endo Laboratories, and naltrexone's development passed to DuPont.
Through the 1970s, naltrexone was put through clinical trials for opioid dependence, in part through a collaboration between DuPont and the U.S. National Institute on Drug Abuse. The logic was straightforward: a person taking a daily opioid blocker could not get high from heroin or other opioids, which might support recovery. That work culminated in 1984, when the U.S. Food and Drug Administration approved oral naltrexone for opioid dependence under the brand name Trexan, at a standard daily dose of 50 mg. (The same molecule was later re-branded ReVia when it was approved for alcohol dependence in 1995, and an extended-release injectable form, Vivitrol, followed in 2006 for alcohol and 2010 for opioid dependence.)
This ordinary history matters for one reason: by 1984 naltrexone was a known, approved, off-patent drug with a well-mapped safety profile at 50 mg. Everything that follows — the entire LDN story — is about a physician noticing that roughly one-tenth of that approved dose seemed to do something completely different. Because the patent had long expired, no drug company ever had a commercial reason to fund the large trials that would normally settle whether such an observation was real. That funding gap is the single most important fact for understanding why, decades later, the evidence for LDN is still thin.
Bernard Bihari: The Man Behind LDN
The figure at the centre of LDN's history is Dr. Bernard Bihari, born November 11, 1931 and died May 16, 2010. He was, by training and career, a mainstream academic physician, not a fringe practitioner — a point worth emphasising because it shapes how his observations should be weighed. He earned a B.A. from Cornell University (1949–1953) and his M.D. from Harvard Medical School (1953–1957). He interned and trained in internal medicine at Beth Israel Hospital in Boston, did a neurology residency at Massachusetts General Hospital, spent two years as a research associate at the National Institute of Mental Health, and completed a psychiatry residency at Columbia-Presbyterian / the New York State Psychiatric Institute. He became board certified by the American Board of Psychiatry and Neurology in 1970.
Bihari's working life was largely devoted to addiction medicine and public health in New York City. He held senior public posts — serving as New York City's Addiction Services Commissioner in the late 1970s and then as a Deputy Commissioner in the city's Department of Health overseeing substance-abuse services — and he directed alcoholism and drug-dependence programmes at what is now SUNY Downstate Health Sciences University in Brooklyn, where he held a long clinical-faculty appointment. He had earlier held academic appointments at Harvard, Mount Sinai, and elsewhere. In short, he was an experienced clinician-administrator steeped in how opioids and opioid-blocking drugs behave — exactly the background that put him in a position to notice something unexpected about naltrexone.
It was this addiction-treatment work that placed naltrexone in his hands in the first place. As a clinician using opioid antagonists with people recovering from drug dependence, Bihari was already familiar with the 50 mg dose. What turned him toward low doses was a tragedy unfolding in his own patient population in the early-to-mid 1980s: the arrival of AIDS.
The Discovery: AIDS and the 3 mg Observation
In the mid-1980s, the patients Bihari treated for drug addiction in New York were among the hardest hit by the emerging HIV/AIDS epidemic, and many were dying of immune collapse. Reasoning from the then-new idea that the body's own opioid-like chemicals (endorphins and enkephalins) might influence immune function, Bihari explored whether briefly and partially blocking opioid receptors could prompt the body to increase its own endorphin output and, in turn, support a failing immune system. The crucial move was to use a dose far below the 50 mg approved level.
The widely repeated origin detail is that at roughly 3 mg, Bihari measured a large rise in endorphin levels — reported as roughly a tripling within a few hours of a bedtime dose — without the full receptor blockade that a 50 mg dose produces. He served as principal investigator for a study titled "Low Dose Naltrexone in AIDS Treatment" at SUNY Downstate's medical centre in 1985–1986, in which he reported that patients taking the low dose appeared to fare better than those who did not. This is the moment LDN, as a distinct idea, was born: same molecule, roughly one-tenth the dose, taken at night, aimed not at addiction but at the immune system.
Two honest caveats belong right here. First, this early AIDS work was small and conducted in the pre-antiretroviral era; it did not establish LDN as an effective HIV treatment, and modern HIV care rests on entirely different, proven medications. Second, the specific "endorphins tripled / immune system normalised" framing comes largely from Bihari's own reports and later advocacy literature, not from large independent trials. What is firmly documented is the historical fact that Bihari originated and named the low-dose approach in this period — not that he proved it worked.
From HIV to Autoimmunity and Cancer
Having observed an apparent immune effect, Bihari spent the following decades extending LDN to a wide range of conditions in his New York practice. He came to believe that an "immune-normalising" agent should help wherever the immune system was misbehaving — whether it was underactive (as in infection or cancer surveillance) or overactive and self-attacking (as in autoimmune disease). Over the 1990s and 2000s he reported using LDN in patients with multiple sclerosis, Crohn's disease, autoimmune thyroid disease, lupus and other autoimmune conditions, and various cancers, and he described treating thousands of patients over his career.
This is the period in which LDN's now-familiar reputation took shape — as a cheap, well-tolerated, broadly "immune-modulating" drug taken at bedtime for chronic, inflammation-linked illness. It is also the period that most requires honesty. Bihari's expansion of LDN to cancer and autoimmune disease rested on clinical experience and case observation, not on the kind of randomised controlled trials that establish whether a treatment truly works. Accumulated clinical impressions are a legitimate reason to investigate a drug; they are not proof of benefit, and the history of medicine is full of treatments that looked promising in one enthusiastic clinic and did not hold up when tested rigorously. The value of Bihari's work was that it generated a clear, testable hypothesis. Whether that hypothesis survives testing is the subject of the Evidence and Mainstream Reception section below.
The Penn State Science: Opioid Growth Factor
For years, the most common objection to LDN was that there was no plausible mechanism for how a tiny dose of an opioid blocker could affect the immune system or tumour growth. A line of laboratory research from Pennsylvania State University College of Medicine in Hershey, led by the biologists Ian S. Zagon and Patricia J. McLaughlin (working over many years, beginning in the 1980s), offered one candidate answer that is independent of Bihari's clinical claims.
Zagon and McLaughlin studied an endogenous opioid peptide, [Met5]-enkephalin, which they termed the opioid growth factor (OGF) because it acts as a natural brake on cell proliferation through its own receptor (OGFr). Their proposed model for LDN is the "intermittent blockade" idea: a brief, low-dose block of the OGF–OGFr pathway is followed by a rebound — the body compensates by producing more OGF and more receptors — which can then slow the division of certain cells, including some cancer and immune cells. This laboratory work, in cell cultures and animal models, gives LDN a biologically coherent candidate mechanism and links it to measurable molecules rather than to vague "immune balancing."
It is important to keep the categories straight. The OGF research is real, peer-reviewed cell-and-animal science, and Zagon and McLaughlin's laboratory has published extensively on it. But a mechanism that works in a petri dish or a mouse is a reason to run human trials, not a substitute for them — many mechanistically elegant ideas fail in people. The OGF work explains how LDN might act; it does not, by itself, prove that LDN helps patients with any given disease. (A separate, much-discussed idea — that LDN also blocks Toll-like receptor 4 (TLR4) on the brain's microglia and so dampens neuro-inflammation and chronic pain — is covered on the main Low-Dose Naltrexone page and in the Benefits articles.)
How LDN Spread: Patients, Pharmacies, and a Charity
Because no company stood to profit from a generic drug used off-label, LDN spread in an unusual way: largely through patients, sympathetic physicians, compounding pharmacists, and the internet rather than through pharmaceutical marketing. A practical obstacle shaped everything — manufactured naltrexone tablets are 50 mg, so an LDN dose of roughly 1.5–4.5 mg has to be made specially. Compounding pharmacies, which prepare customised formulations, therefore became central to LDN's availability, dispensing low-dose capsules or liquids against off-label prescriptions.
The most significant organised effort to spread and study LDN came from the United Kingdom. In 2004, Linda Elsegood — a multiple-sclerosis patient who reported substantial improvement after starting LDN in late 2003 — founded the LDN Research Trust, a UK-registered charity run by volunteers. The Trust has worked for two decades to raise awareness, connect patients with prescribers and pharmacies, host conferences, and encourage formal research, and it has helped publish patient-and-practitioner literature on the subject. Advocacy organisations like this one are why LDN became widely known to patients long before mainstream medicine engaged with it.
A note on honesty about sources: much of the enthusiastic information about LDN online comes from advocacy groups, compounding-pharmacy marketing, and patient testimonial, all of which have an interest — financial or emotional — in LDN's success. None of this makes LDN a scam; it has a plausible mechanism, a benign safety profile at low doses, and some encouraging early trials. But it does mean a reader should weight patient-advocacy claims differently from peer-reviewed controlled trials, which is exactly the distinction the next section draws.
Evidence and Mainstream Reception
Here is the plain truth a non-profit health site owes its readers: LDN is not approved by the FDA (or other major regulators) for any of the autoimmune, pain, or chronic-illness conditions it is used for, and it remains investigational. Every such use is off-label. The evidence base is genuinely mixed — more than empty, far less than conclusive.
The most-cited positive trials are small but real. Jill P. Smith and colleagues at Penn State ran an open-label pilot in active Crohn's disease (17 patients, 2007) reporting that most improved, and then a larger randomised, placebo-controlled trial (40 patients, 2011) reporting that 4.5 mg naltrexone improved clinical activity and promoted mucosal healing compared with placebo. In fibromyalgia, Jarred Younger and colleagues at Stanford conducted small randomised crossover trials (2013) showing meaningful reductions in daily pain. These are encouraging, methodologically sound, small studies.
The honest counterweight is how the systematic-review evidence reads. A 2018 Cochrane systematic review of LDN for inducing remission in Crohn's disease concluded that there was insufficient evidence to draw firm conclusions about its efficacy and safety, rating the overall quality of the evidence as low because the trials were so small. Standard medical references similarly note that solid evidence for recommending LDN is lacking and that larger, well-designed trials are needed. In multiple sclerosis — one of the conditions most associated with LDN — trials have generally been small and have not established a clear effect on the disease itself, though some report quality-of-life or symptom benefit.
So the fair summary is this. LDN is a low-cost, generally well-tolerated, off-label drug with a coherent candidate mechanism and a handful of promising small trials, championed by a credentialed physician and a grassroots patient movement — but it has not been proven effective for the conditions it is popularly used for, and the largest, most rigorous syntheses of the data describe the evidence as low-quality and insufficient. Anyone considering LDN should treat it as an investigational option to discuss with a knowledgeable clinician, weigh the real (if modest) evidence honestly, and be especially cautious about the central drug interaction: because naltrexone blocks opioid receptors, LDN must not be combined with prescription opioid pain medication. The detailed mechanism, dosing, side effects, and condition-by-condition evidence are covered on the main Low-Dose Naltrexone page and in the Benefits articles; this history is concerned with how the remedy came to be.
Research Papers and References
The list below combines key peer-reviewed studies and reviews on low-dose naltrexone with curated PubMed topic-search links into the historical and clinical literature. Author names, titles, and journals are given as plain text; only the stable DOI, PMID, or archive link is hyperlinked, and each opens in a new tab. Biographical details for Dr. Bernard Bihari are drawn from his published curriculum vitae and obituary, cited as historical sources.
- Smith JP, Stock H, Bingaman S, Mauger D, Rogosnitzky M, Zagon IS. Low-dose naltrexone therapy improves active Crohn's disease. American Journal of Gastroenterology. 2007;102(4):820-828. — Search PubMed
- Smith JP, Bingaman SI, Ruggiero F, Mauger DT, Mukherjee A, McGovern CO, Zagon IS. Therapy with the opioid antagonist naltrexone promotes mucosal healing in active Crohn's disease: a randomized placebo-controlled trial. Digestive Diseases and Sciences. 2011;56(7):2088-2097. — PMID: 21380937
- Younger J, Noor N, McCue R, Mackey S. Low-dose naltrexone for the treatment of fibromyalgia: findings of a small, randomized, double-blind, placebo-controlled, counterbalanced, crossover trial assessing daily pain levels. Arthritis & Rheumatism. 2013;65(2):529-538. — doi:10.1002/art.37734
- Parker CE, Nguyen TM, Segal D, MacDonald JK, Chande N. Low dose naltrexone for induction of remission in Crohn's disease. Cochrane Database of Systematic Reviews. 2018;(4):CD010410. — PMID: 29607497
- Younger J, Parkitny L, McLain D. The use of low-dose naltrexone (LDN) as a novel anti-inflammatory treatment for chronic pain. Clinical Rheumatology. 2014;33(4):451-459. — PMID: 24526250
- Toljan K, Vrooman B. Low-dose naltrexone (LDN) — review of therapeutic utilization. Medical Sciences (Basel). 2018;6(4):82. — PMID: 30248938
- Bernard Bihari, M.D. — Curriculum Vitae (biographical primary source). — lowdosenaltrexone.org — Bihari CV
- Low-dose naltrexone history and mechanism PubMed: low-dose naltrexone history and mechanism
- Opioid growth factor (OGF), [Met5]-enkephalin, and naltrexone PubMed: opioid growth factor and naltrexone (Zagon, McLaughlin)
External Authoritative Resources
Connections
- All Remedies
- Low-Dose Naltrexone for Fibromyalgia — the same drug in its best-studied indication, where the Younger/Stanford trials were run — the fullest account of titration schedules, morning-versus-bedtime timing, and compounding costs.
- Low-Dose Naltrexone for POTS — the same drug and dose range aimed at dysautonomia rather than widespread pain — who responds, who should avoid it, and how it is layered onto beta-blockers, ivabradine, and salt loading.
- Low-Dose Naltrexone
- Low-Dose Naltrexone Benefits
- Crohn's Disease
- Fibromyalgia
- Multiple Sclerosis
- Hashimoto's Thyroiditis
- Anti-Inflammatory Diet