Pickle Juice and the Neural Reflex for Cramp Relief
A 1-ounce sip of pickle juice stops an electrically induced muscle cramp in about 85 seconds — roughly 45% faster than the same volume of plain water. That was the headline result of Kevin Miller's landmark 2010 trial at North Dakota State University. The finding sat oddly with the conventional electrolyte-replacement story because 1 ounce of pickle brine, swallowed, cannot meaningfully alter blood sodium or plasma volume in 85 seconds — the gastric emptying alone takes longer. The most parsimonious explanation is a neural reflex: the strong sour-salty stimulus on the oropharynx triggers TRPV1 and TRPA1 receptors in the upper digestive tract, which descend-inhibit the alpha-motoneuron pool through brainstem pathways and interrupt the cramping signal. The same mechanism explains why mustard, vinegar, ginger, and even capsaicin work, and why the relief lasts only briefly — you have interrupted a reflex, not corrected an underlying deficit. This page covers the trial evidence, the proposed mechanism, the practical application, and the limits.
Interactive Visualization Magnesium — the mineral that makes ATP work Bare ATP is useless and enzymes reject it. Watch magnesium clamp the phosphates and switch it on, plug the NMDA channel, and let a cramping muscle finally let go. Launch →
Table of Contents
- The Miller 2010 Trial — What It Actually Showed
- Why It Cannot Be Electrolyte Replacement
- The TRP Receptor Mechanism
- The Altered-Neuromuscular-Control Model
- What Else Works by the Same Reflex — Mustard, Ginger, Capsaicin
- Practical Use During Exercise
- HotShot, Hot Cramp Stop, and Other Commercial Products
- What It Does NOT Do
- Combining With Other Strategies
- Cautions
- Key Research Papers
- Connections
- Featured Videos
The Miller 2010 Trial — What It Actually Showed
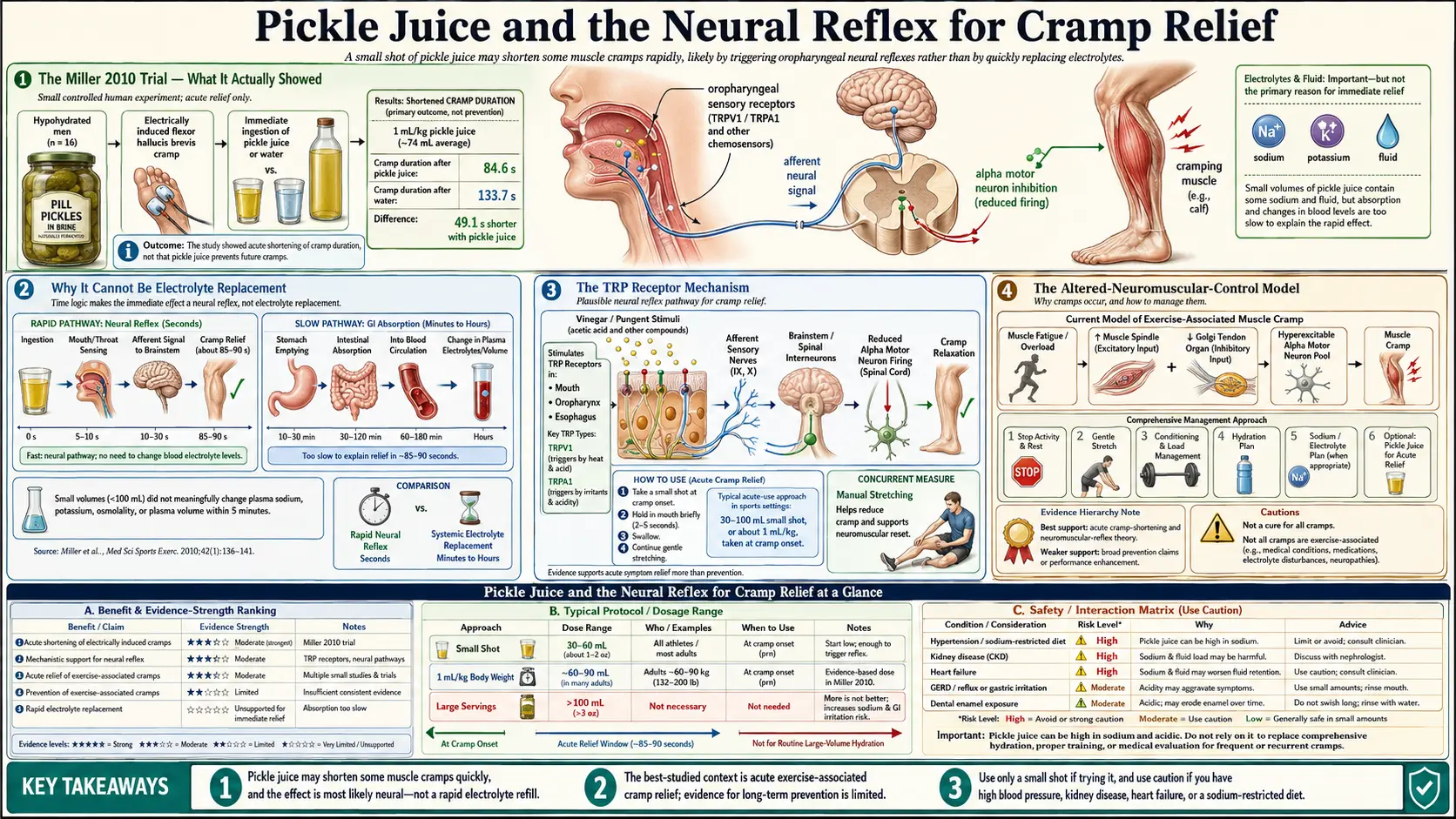
Kevin C. Miller and colleagues published in Medicine & Science in Sports & Exercise in 2010 a controlled experimental study with a design specifically engineered to test the dehydration/electrolyte hypothesis. Ten healthy, hydrated male volunteers were dehydrated by ~3% body mass via thermal stress and exercise. Once dehydrated, they had the dominant foot's flexor hallucis brevis muscle electrically stimulated through the tibial nerve at high frequency to induce a cramp.
Immediately after cramp onset, subjects swallowed either 1 mL/kg body mass (~75 mL, about 2.5 ounces) of pickle juice or the same volume of deionized water. Cramp duration was recorded as the time from cramp onset to cessation of EMG activity.
The results:
- Pickle juice condition: mean cramp duration was approximately 85 seconds
- Water condition: mean cramp duration was approximately 134 seconds
- The pickle juice cramps resolved ~37% faster than the water cramps (p < 0.05)
- Plasma sodium concentrations did not change measurably in either group during the trial window
- Plasma osmolality, hematocrit, and plasma volume did not change in either group
The plasma measurements are the crucial finding. The cramps abated in the pickle juice group long before any of the sodium from the brine could have reached the bloodstream — not just because gastric emptying takes 10-30 minutes for fluids of this volume, but because the relief was observed within the time frame where most of the swallowed fluid was still in the stomach.
Miller's 2013 follow-up trial (Journal of Athletic Training) confirmed and extended the finding: pickle juice ingestion produced no measurable changes in plasma electrolytes, osmolality, or plasma volume within 60 minutes of ingestion in hydrated or dehydrated subjects. Whatever was abolishing the cramps was acting through a non-electrolyte pathway.
Why It Cannot Be Electrolyte Replacement
The math kills the electrolyte hypothesis. A standard ounce of dill pickle brine contains approximately 180-360 mg of sodium and about 60 mg of potassium. The typical "stop the cramp" dose of pickle juice in athletic practice is 2-3 ounces. So the total electrolyte payload is roughly 500-1000 mg of sodium and 100-200 mg of potassium.
Two reasons that payload cannot be the mechanism:
- The timing is wrong. A 75-mL bolus of acidic, sodium-rich liquid swallowed into an empty stomach takes 15-45 minutes for the sodium to begin to reach systemic circulation. Cramps in the Miller trial abated in 60-90 seconds. Even allowing generous absorption kinetics, the pickle brine sodium had not yet reached the small intestine, let alone the bloodstream, when the cramps stopped.
- The dose is too small to matter at the muscle. Total body sodium content in a 70-kg adult is approximately 100 grams (~4,000 mmol). Adding 500 mg of sodium represents 0.5% of the total body sodium. The muscle cell's membrane potential is dominated by intracellular potassium and the sodium-potassium gradient, neither of which can be meaningfully shifted by a fraction of a percent change in total body sodium — particularly when the sodium has not yet had time to equilibrate across cellular compartments.
Schwellnus and colleagues at the University of Cape Town had already published the case against the dehydration-electrolyte model of exercise-associated muscle cramps in 2004 and 2009 in British Journal of Sports Medicine. They studied South African Ironman triathletes and found that cramping athletes did not have lower serum sodium, potassium, magnesium, or calcium than non-cramping athletes from the same race. They proposed instead the "altered neuromuscular control" model: cramps arise from sustained involuntary alpha-motoneuron discharge driven by muscle fatigue, not from any specific electrolyte deficit. The pickle juice mechanism fits naturally into this model.
The TRP Receptor Mechanism
The proposed mechanism is a reflex arc through the transient receptor potential (TRP) channel family in the oropharyngeal epithelium. Two TRP family members are particularly relevant:
- TRPV1 (transient receptor potential vanilloid 1) — the receptor activated by capsaicin (the heat compound in chili peppers), high temperature (>43°C), low pH, and a variety of inflammatory mediators. TRPV1 is densely expressed in the trigeminal sensory innervation of the mouth, pharynx, and upper esophagus.
- TRPA1 (transient receptor potential ankyrin 1) — the receptor activated by allyl isothiocyanate (the pungent compound in mustard and horseradish), cinnamaldehyde, allicin (from garlic), low temperature, and various electrophilic irritants. Also densely expressed in oropharyngeal sensory innervation.
Both TRPV1 and TRPA1 are activated strongly by pickle brine: the low pH (~3.0) and high osmolality stimulate both receptors. The mustard, capsaicin, ginger, and cinnamaldehyde products that work for the same purpose activate these receptors more specifically.
The reflex arc, in the Behringer and Craighead hypothesis:
- TRPV1/TRPA1 activation in oropharyngeal sensory afferents
- Afferent signal travels via the trigeminal nerve to the nucleus of the solitary tract in the brainstem
- Brainstem polysynaptic descending pathways inhibit the alpha-motoneuron pool in the spinal cord, specifically targeting the over-firing motor units producing the cramp
- The cramping muscle releases as the descending inhibition overcomes the local hyperexcitability
The mechanism is consistent with the rapid time course (consistent with central neural processing rather than peripheral chemistry), the relatively short duration of effect (the brainstem inhibition wears off as the oropharyngeal stimulus fades), and the cross-effectiveness of several TRP agonists (vinegar, mustard, ginger, capsaicin all work because they all activate the same receptors).
Craighead et al. (2017) provided supportive evidence in a controlled trial: ingestion of a proprietary TRP agonist beverage attenuated electrically induced muscle cramps in healthy volunteers, with the magnitude of effect comparable to pickle juice. The Behringer 2017 trial showed similar effects for capsaicin-containing solutions.
The Altered-Neuromuscular-Control Model
To understand why a brainstem reflex would matter for muscle cramps, the underlying pathophysiology of exercise-associated muscle cramping (EAMC) is worth understanding. The current best model, developed by Martin Schwellnus and refined by subsequent investigators, posits:
- Sustained submaximal muscular work produces metabolic fatigue in motor units
- The Golgi tendon organ inhibitory feedback (which normally protects against excessive contraction by activating Ib inhibitory interneurons in the spinal cord) is progressively reduced with fatigue
- Muscle spindle afferent feedback (the Ia afferent loop that drives the stretch reflex) becomes progressively more facilitated
- The net effect is rising alpha-motoneuron excitability in the absence of conscious volitional drive
- Eventually some critical mass of motor units fires sustained involuntary action potential trains
- The visible result is a focal, hard, painful muscle cramp
The cramp is a spinal-cord-level phenomenon. It is not a muscle problem in the strict sense — the muscle is responding correctly to inappropriate motor neuron discharge. Anything that reduces alpha-motoneuron excitability can break the cycle. Three classes of intervention work this way:
- Mechanical Golgi tendon stimulation — passive stretching of the cramping muscle activates the Golgi tendon organs and recruits Ib inhibitory interneurons, breaking the cramp. This is why stretching the calf works for an acute calf cramp and is covered in Stretch & Reset Techniques.
- Reciprocal inhibition — voluntary contraction of the antagonist muscle inhibits the cramping agonist via reciprocal inhibition pathways. Pulling the toes up to the shin (dorsiflexing the ankle by contracting the tibialis anterior) reciprocally inhibits the gastrocnemius cramp.
- Descending brainstem inhibition — the TRPV1/TRPA1 oropharyngeal reflex described above. The neural reflex remedies (pickle juice, mustard, ginger) work here.
These three pathways are independent and additive. The fastest way to break an acute exercise cramp is to combine all three: take a swallow of pickle juice or mustard, simultaneously stretch the cramping muscle, and reciprocally contract the antagonist. Most experienced endurance athletes have developed some version of this protocol intuitively.
What Else Works by the Same Reflex — Mustard, Ginger, Capsaicin
If the mechanism is TRP receptor activation in the oropharynx, then any potent TRP agonist should work. Practical alternatives to pickle juice, in approximate order of how widely they have been used or studied:
- Yellow mustard — a packet of fast-food yellow mustard (~5 mL) contains allyl isothiocyanate (TRPA1 agonist) and vinegar (acid + osmotic load). Widely used among long-distance cyclists and ultrarunners. The "swallow a mustard packet" remedy predates the Miller pickle juice trial by decades; the mechanism is now understood to be the same. Some athletes carry restaurant mustard packets in race belts specifically for this purpose.
- Apple cider vinegar — 1-2 tablespoons, neat or in water. Activates the same low-pH pathway as pickle juice. Lower oropharyngeal stimulus intensity than concentrated brine; some users find it less reliably effective.
- Capsaicin / hot sauce — the original TRPV1 agonist. A small spoonful of hot sauce (Tabasco, sriracha, etc.) triggers a strong TRPV1 response. The HotShot commercial product (see below) is essentially a high-quality formulated capsaicin/ginger/cinnamon beverage built around this mechanism.
- Ginger (fresh root or extract) — activates TRPV1 and TRPA1. Generally used as a strong ginger tea or a ginger candy chewed at the onset of cramping. Less acute punch than mustard or capsaicin but more palatable for prolonged or repeated use.
- Cinnamon (cinnamaldehyde) — TRPA1 agonist. Cinnamon oil is too strong neat but cinnamon in solution (cinnamon tea, cinnamon-flavored ginger beverage) contributes.
- Garlic (allicin) — TRPA1 agonist. Rarely used as a stand-alone cramp remedy but a component of some folk formulas.
The unifying feature is intense oropharyngeal stimulation that the brain registers as strongly novel and aversive. Bland liquids (water, sports drinks, milk) do not work because they do not activate TRPV1/TRPA1 strongly enough to trigger the reflex.
Some users have noted that the strong sensory stimulus alone (rinsing the mouth briefly with hot mustard but not swallowing) also breaks cramps, supporting the oropharyngeal-reflex hypothesis over any gastric or systemic mechanism. This is consistent with the broader physiology — the descending inhibition from brainstem is triggered by the sensory signal, not by absorption.
Practical Use During Exercise
For an athlete prone to exercise-associated muscle cramping, a practical protocol:
- Carry a single-serve remedy in the race belt, jersey pocket, or hydration vest. Options that travel well: a 2-3 oz pickle juice "shot" (sold by Pickle Juice Sport, HotShot, and others in compact pouches), 3-4 restaurant mustard packets, or 1-2 ginger chews. Refrigerated pickle juice and mustard packets stay stable for the duration of any race.
- Take at the first sign of muscle twinging, not after the full cramp has set in. Most experienced athletes recognize a "pre-cramp" tightness 30-60 seconds before the actual cramp. Intervening at that point often prevents the cramp from fully developing.
- If the full cramp has set in, do all three interventions simultaneously: swallow the pickle juice/mustard, stretch the cramping muscle, and reciprocally contract the antagonist. For a calf cramp: pull toes toward shin, lean forward against a wall to stretch the calf, swallow the remedy. Expect resolution in 60-120 seconds.
- Do not over-rely on the reflex remedies for prevention. The neural reflex stops a cramp once it has started; it does not prevent the next one. The Schwellnus model predicts (and observation confirms) that an athlete who cramps once during a race is at high risk of additional cramps over the next 30-60 minutes. Reducing race pace to relieve muscle fatigue is the dominant prevention strategy.
- Use sparingly. Repeated mustard or pickle juice within minutes loses efficacy as the oropharynx adapts. One dose per cramp event, then wait 10-15 minutes before another attempt if needed.
For training rather than racing, prevention is more useful than treatment: progressive overload, proper warm-up, adequate sodium intake during heat exposure, and adequate recovery between sessions. Heat acclimation over 10-14 days reduces sweat sodium losses by 50% or more, dramatically reducing cramp risk in hot-weather endurance events.
HotShot, Hot Cramp Stop, and Other Commercial Products
The pickle juice mechanism has spawned a small but real commercial category:
- HotShot — a 1.7-fl-oz proprietary blend of cinnamon, ginger, and capsicum extract designed by Bruce Bean (MD, PhD — neuroscientist at Harvard) and Roderick MacKinnon (Nobel laureate ion channel researcher). Marketed specifically to athletes for cramp prevention and treatment. The TRP-agonist mechanism is explicitly the basis of the formulation. Approximately $5 per shot; widely available online and in some specialty sports retailers.
- Pickle Juice Sport — 2.5-fl-oz or 8-fl-oz pickle brine bottles formulated for athletic use. Includes additional electrolytes. The original "pickle juice as athletic remedy" commercial product.
- Generic dill pickle brine — the cheapest option. Pour off the brine from a jar of dill pickles into a small flask. Effectiveness is comparable to commercial products if the pickles are vinegar-fermented; bear in mind that "pickles" in some American grocery stores are calcium-chloride-set vegetables that did not undergo true fermentation and may have less acid intensity.
- Restaurant mustard packets — effectively free, ship and store indefinitely, and small enough to carry several. The taste is unpleasant in concentration but the mechanism works.
- Crampfix — an Australian product with similar TRP-agonist formulation.
The branded products offer no proven advantage over a small bottle of pickle brine carried in a race belt; their value is convenience, portion control, palatability, and brand-trust signaling. For training and casual use, the home version is fine. For race-day insurance, the small, leak-proof commercial sachets are easier to carry than a bottle of brine.
What It Does NOT Do
The neural reflex remedies are powerful for one specific application and largely useless for several others. Things pickle juice does NOT do:
- Prevent nocturnal leg cramps in older adults — the geriatric cramp arises from chronic calf shortening, peripheral nerve hyperexcitability, and (often) functional magnesium deficiency. A swallow of pickle juice at bedtime does not address any of these mechanisms. The interventions with evidence here are passive stretching and magnesium repletion.
- Replace electrolytes lost in genuine sweat depletion — a 4-hour Ironman bike leg in 90°F humidity produces sweat sodium losses that 1 ounce of pickle brine cannot dent. For that volume of depletion, a proper sports drink or salt tablet plus water is needed in addition to the reflex remedy. The two strategies are complementary, not interchangeable.
- Treat pregnancy leg cramps — pregnancy cramps appear to be a magnesium / calcium / posture issue, not a neural-reflex issue. Magnesium glycinate and calf stretching are the evidence-based interventions.
- Treat drug-induced cramps — if statin myopathy or diuretic-driven potassium depletion is producing the cramps, identifying and addressing the drug cause is the only durable solution.
- Treat true tetany from severe hypocalcemia or hypomagnesemia — medical emergency requiring intravenous calcium or magnesium, not a swallow of brine.
- Treat neurological cramping (ALS, motor neuron disease, severe peripheral neuropathy) — cramping in these conditions arises from peripheral nerve pathology and requires medical management.
Combining With Other Strategies
The neural reflex remedies work best as part of a layered strategy:
- Baseline (always-on): adequate dietary potassium and magnesium, normal hydration, regular calf stretching, periodic strength training of the calves to build fatigue resistance.
- Race-day prophylaxis: appropriate pacing relative to fitness, adequate carbohydrate intake to delay metabolic fatigue, sodium replacement matched to expected sweat losses (see Hydration Beyond Water), heat acclimation in the 10-14 days before a hot race.
- Acute treatment: at first twinge, take the neural reflex remedy plus immediate stretch of the at-risk muscle. If the cramp progresses, add reciprocal antagonist contraction. If multiple cramps within 30 minutes, accept that the muscle is past its current fitness capacity and reduce pace.
For an endurance athlete who cramps reliably at the same point in events of similar length, the underlying issue is most often inadequate aerobic base, training-specificity mismatch, or pacing — not nutrition. Pickle juice may rescue the race but will not fix the recurrent pattern. The pattern itself is the signal to retrain for the event.
For more on the broader exercise nutrition picture, see Bananas (potassium), Sodium, and Potassium.
Cautions
- Hypertension and sodium-restricted diets — one ounce of pickle juice contains 180-360 mg of sodium. For an athlete on a sodium-restricted diet for hypertension or congestive heart failure, the occasional racing dose is unlikely to matter, but daily prophylactic use is not appropriate. Use commercial low-sodium TRP-agonist alternatives (mustard, ginger, capsaicin) instead.
- Reflux disease (GERD) — the acidity of pickle juice (~pH 3.0) can aggravate GERD and esophagitis. For athletes with reflux, ginger candy or capsaicin-based commercial products are gentler.
- Acute gastritis or peptic ulcer — same caution as reflux. Highly acidic remedies on an already-inflamed stomach can be painful.
- Capsaicin and TRPV1 desensitization — chronic high-dose capsaicin exposure (much higher than the cramp-relief dose) can desensitize TRPV1 receptors. Not a concern at typical use frequencies but relevant for athletes considering daily prophylactic capsaicin.
- Allergies — ginger, mustard, and other TRP agonist sources are occasionally allergenic. Use a different agonist if hypersensitivity exists.
- Children and adolescents — the data on cramp-relief use are in adults. Pediatric muscle cramps should be evaluated for underlying medical cause (electrolyte disorder, neurologic condition, drug side effect) before adopting a symptomatic remedy strategy.
- The remedy does not address underlying causes — recurrent cramping warrants medical evaluation. Relying on pickle juice while ignoring statin-driven myopathy, peripheral neuropathy, or chronic kidney disease is not a good plan.
Key Research Papers
- Miller KC, Mack GW, Knight KL, Hopkins JT, Draper DO, Fields PJ, Hunter I (2010). Reflex inhibition of electrically induced muscle cramps in hypohydrated humans. Medicine & Science in Sports & Exercise. — Search PubMed
- Miller KC (2014). Plasma electrolyte and osmolality responses to pickle juice ingestion at rest and following exercise-induced dehydration. Journal of Athletic Training. — Search PubMed
- Behringer M, Nowak S, Leyendecker J, Mester J (2017). Effects of TRPV1 and TRPA1 channel activators on exercise-induced muscle cramp threshold frequency. European Journal of Applied Physiology. — Search PubMed
- Craighead DH, Shank SW, Volz KM, Alexander LM (2017). Ingestion of transient receptor potential channel agonists attenuates exercise-induced muscle cramps. Muscle & Nerve. — Search PubMed
- Schwellnus MP (2009). Cause of exercise associated muscle cramps (EAMC) — altered neuromuscular control, dehydration or electrolyte depletion? British Journal of Sports Medicine. — Search PubMed
- Schwellnus MP, Drew N, Collins M (2011). Increased running speed and previous cramps rather than dehydration or serum sodium changes predict exercise-associated muscle cramping. British Journal of Sports Medicine. — Search PubMed
- Schwellnus MP, Nicol J, Laubscher R, Noakes TD (2004). Serum electrolyte concentrations and hydration status are not associated with exercise associated muscle cramping in distance runners. British Journal of Sports Medicine. — Search PubMed
- Khan SI, Burne JA (2007). Reflex inhibition of normal cramp following electrical stimulation of the muscle tendon. Journal of Neurophysiology. — Search PubMed
- Bertolasi L, De Grandis D, Bongiovanni LG, Zanette GP, Gasperini M (1993). The influence of muscular lengthening on cramps. Annals of Neurology. — Search PubMed
- Miller KC, McDermott BP, Yeargin SW, Fiol A, Schwellnus MP (2022). An evidence-based review of the pathophysiology, treatment, and prevention of exercise-associated muscle cramps. Journal of Athletic Training. — Search PubMed
- Bean BP, MacKinnon R (2016). HotShot patent and TRP-channel cramp prevention mechanism PubMed: Bean/MacKinnon TRP cramp
PubMed Topic Searches
- PubMed: Pickle juice and exercise cramps
- PubMed: TRP receptor oropharyngeal reflex
- PubMed: EAMC altered neuromuscular control
- PubMed: Schwellnus EAMC research
- PubMed: Capsaicin/ginger/mustard for cramps
Connections
- Magnesium: The Mineral That Makes ATP Work — interactive animation
- Cramp Prevention Main Page
- Cramp Benefits Hub
- Magnesium & Electrolytes
- Hydration Beyond Water
- Stretch & Reset Techniques
- Ginger
- Cinnamon
- Garlic
- Hot Peppers (Capsaicin)
- Sodium
- Potassium
- Magnesium
- Apple Cider Vinegar
- All Remedies
- Restless Legs Syndrome