Hydration Beyond Water for Cramp Prevention
The advice to "drink more water" is one of the most over-prescribed and under-thought interventions in lay nutrition. For muscle cramp prevention, drinking large volumes of plain water in a heat-stress or endurance-exercise context can actually worsen outcomes by producing exercise-associated hyponatremia (EAH) — a now well-documented and occasionally fatal complication of marathon and ultra-event participation. The Almond et al. 2005 NEJM study found that 13% of Boston Marathon finishers had hyponatremia (serum sodium <135 mmol/L), and the strongest predictor was weight gain during the race — the over-drinkers, not the dehydrated. Real hydration management depends on matching fluid composition to fluid losses, accounting for sodium content of sweat, building proper oral rehydration solutions, and recognizing the conditions where dehydration genuinely matters versus the more common situation where electrolyte balance dominates. This page works through the math.
Interactive Visualization Magnesium — the mineral that makes ATP work Bare ATP is useless and enzymes reject it. Watch magnesium clamp the phosphates and switch it on, plug the NMDA channel, and let a cramping muscle finally let go. Launch →
Table of Contents
- Why Plain Water Is Not Hydration
- Sweat Composition and Why It Varies
- Exercise-Associated Hyponatremia (EAH)
- Building a Proper Oral Rehydration Solution
- Commercial Products — LMNT, Nuun, Liquid IV, Gatorade
- Matching Fluid Choice to Context
- Hydration in Older Adults — The Other End of the Spectrum
- The Nocturnal-Cramp Context (Hydration Is Usually NOT the Answer)
- Rehydration After GI Illness
- Cautions
- Key Research Papers
- Connections
- Featured Videos
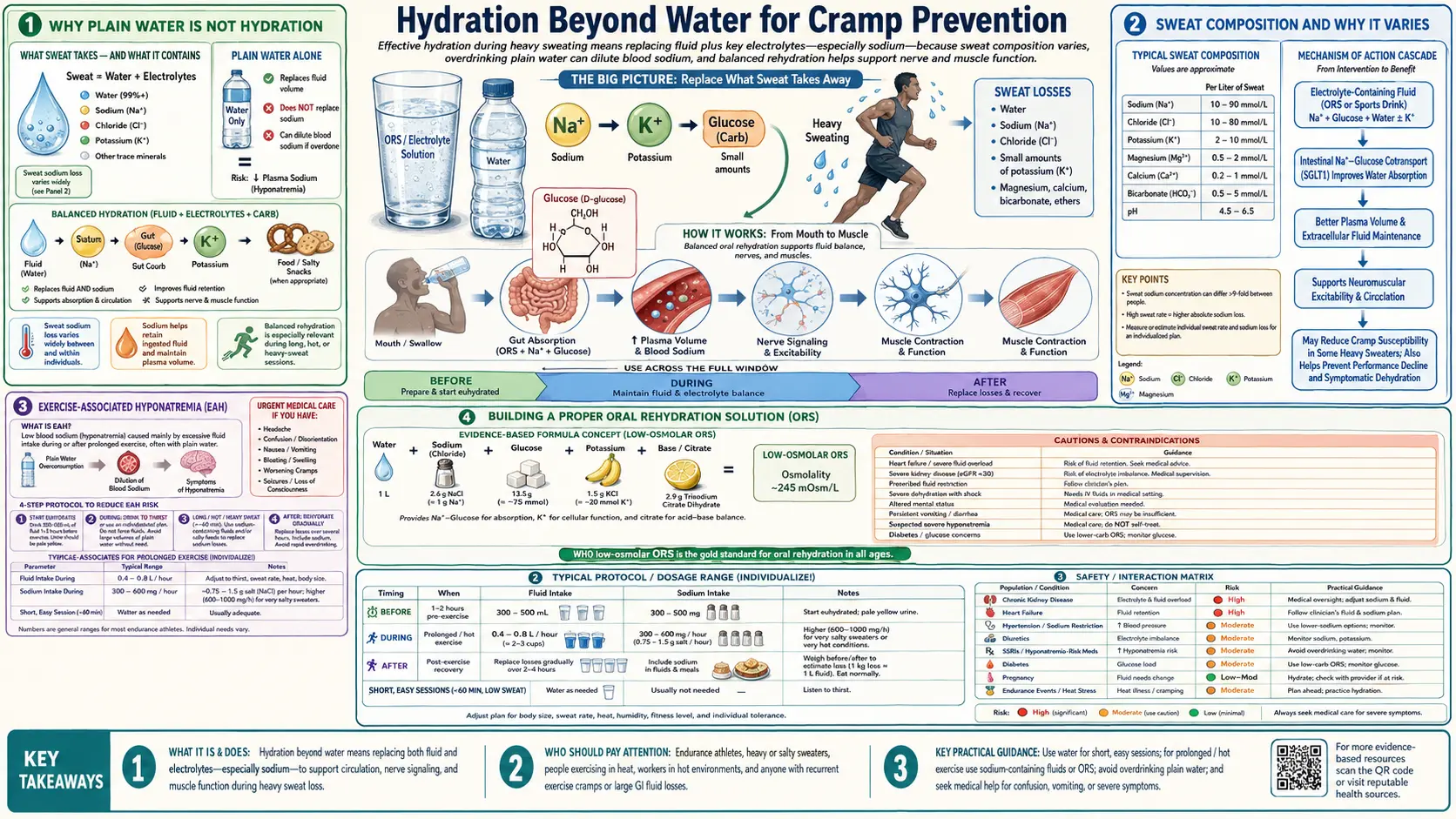
Why Plain Water Is Not Hydration
Drinking water alone is hydration if and only if total body water is being lost at the same composition as plain water. That essentially never happens. Sweat, urine, and gastrointestinal losses all contain electrolytes in addition to water. Replacing the lost volume with electrolyte-free water increases total body water faster than it increases extracellular electrolyte content, which dilutes plasma sodium.
The body has a narrow tolerance for plasma sodium. The reference range is 135-145 mmol/L. Below 130 mmol/L muscle cramps, weakness, and confusion appear; below 125 mmol/L seizure and altered mental status; below 120 mmol/L cerebral edema, brainstem herniation, and death are all real risks. Exercise-associated hyponatremia (EAH) has produced several documented athlete deaths in the modern marathon era.
The root error in the popular "drink more water" advice is the failure to distinguish three distinct scenarios:
- Mild voluntary dehydration in a sedentary or low-activity setting — the typical "I haven't been drinking enough" scenario. Total body water is modestly low; sodium concentration is essentially normal. Plain water is adequate, in moderate amounts. Drinking 2-3 liters per day in this setting is fine. Drinking 5+ liters per day is excessive and risks hyponatremia in some patients.
- Significant volume depletion with electrolyte loss — sweat-driven losses from endurance exercise or heat exposure, GI losses from diarrhea or vomiting, diuretic-driven losses. Both water AND electrolytes are being lost. Replacement must include sodium and (often) potassium. Plain water alone makes the electrolyte deficit worse.
- Pure free-water deficit — high-sugar/high-protein meal load that creates an osmolar burden, diabetic ketoacidosis, hypertonic enteral feeds, central diabetes insipidus. Water replacement is appropriate. This is uncommon in everyday practice.
For cramp prevention specifically, the second scenario dominates and is the one where electrolyte composition matters as much as fluid volume.
Sweat Composition and Why It Varies
Sweat is not pure water and is not consistent between individuals. Typical composition:
- Sodium: 200-2000 mg per liter (highly variable, with a typical range for trained athletes of 400-1200 mg/L)
- Chloride: approximately equimolar with sodium (sodium chloride is the dominant osmotic constituent)
- Potassium: 100-300 mg/L (much lower variability)
- Magnesium: 2-10 mg/L (small)
- Calcium: 10-50 mg/L (small)
The sodium concentration varies enormously between individuals and is the dominant factor in determining who is at risk for sweat-driven hyponatremia. Several factors affect sweat sodium:
- Genetic baseline — some individuals are constitutional "salty sweaters" with sodium concentrations of 1500-2000 mg/L (their dried sweat leaves visible white salt rings on clothing). Others run 200-400 mg/L.
- Heat acclimation — 10-14 days of progressive heat exposure causes the body to conserve sodium by reabsorbing more in the sweat duct. Sweat sodium can drop by 50% over a successful acclimation period. This is one reason that early-season cramping in a hot race is so much more common than mid-season cramping at the same intensity.
- Aldosterone status — chronic dietary sodium restriction or aldosterone-driving conditions increase sweat sodium conservation. The "low-sodium hypertensive" eating a strict DASH diet may have reduced sweat sodium losses, but the chronic low-sodium state also lowers their reserves.
- Cystic fibrosis — defective CFTR chloride channels prevent sodium reabsorption in the sweat duct. CF patients have markedly elevated sweat sodium (>60 mmol/L is part of the diagnostic criteria) and are at high risk for sodium loss during heat exposure.
- Sweat rate — at very high sweat rates (~3 L/hour) the duct has less time to reabsorb sodium and the sweat is closer to plasma in sodium content.
Practical implication: an endurance athlete losing 1.5 L/hour of sweat at 800 mg sodium/L loses 1.2 g of sodium per hour. Over a 6-hour Ironman bike-and-run, that is 7.2 g of sodium — about a third of total exchangeable extracellular sodium. Replacing only water during such a workout is a guaranteed path to hyponatremia and likely cramping.
Conversely, a sedentary office worker walking to lunch on a mild day with minimal sweat does not need electrolyte replacement. The mistake is applying endurance-athlete advice to the office worker (over-supplementing sodium) or vice versa (advising the marathon runner to "just drink water"). Context matters.
Exercise-Associated Hyponatremia (EAH)
EAH is defined as serum sodium below 135 mmol/L occurring during or within 24 hours of prolonged endurance exercise. It is the dominant medical complication of long-distance endurance racing in the modern era, having displaced heat stroke as the leading cause of in-race medical emergency in many ultra-events.
The seminal modern study is Almond et al., NEJM 2005, "Hyponatremia among Runners in the Boston Marathon." Findings:
- 13% of 488 marathon finishers had EAH (serum sodium <135)
- 0.6% had critical hyponatremia (<120)
- The strongest predictor was substantial weight gain during the race (suggesting fluid overload, not depletion)
- Slower finishing times were associated with higher EAH risk (more time for over-drinking)
- Female sex, lower BMI, and use of NSAIDs were additional risk factors
- Race-day fluid intake correlated with EAH; sodium intake (relative to fluid intake) protected against EAH
The Hew-Butler et al. Third International EAH Consensus (2015) updated treatment guidance: confirmed acute symptomatic EAH should be treated with hypertonic saline (100 mL of 3% saline IV, repeated as needed), not with conservative fluid restriction alone, because of the risk of cerebral edema. This is opposite to the "drink water" intuition.
The mechanism in distance events is straightforward:
- Athlete loses sweat at typical 1.0-1.5 L/hour with 400-1000 mg/L sodium
- Athlete drinks plain water or low-sodium sports drink at 1.0-1.5 L/hour
- Net result: total body water roughly maintained or expanded, but sodium is replaced at a fraction of loss rate
- Plasma sodium falls, plasma osmolality falls, intracellular water shifts into cells (cerebral edema in the brain, swelling in muscle), neurologic and muscular dysfunction follow
The fix is to either (a) reduce fluid intake to less than sweat loss (mild dehydration is tolerable; over-hydration is dangerous) or (b) include adequate sodium with the fluid. Recreational marathon and triathlon participants tend to do neither, hence the EAH epidemic.
Building a Proper Oral Rehydration Solution
The WHO Oral Rehydration Solution (ORS) is the gold-standard formulation for serious sodium-and-water replacement. The reduced-osmolarity 2002 reformulation:
- Sodium: 75 mmol/L (~1725 mg/L)
- Glucose: 75 mmol/L (~13.5 g/L)
- Potassium: 20 mmol/L (~780 mg/L)
- Chloride: 65 mmol/L
- Citrate: 10 mmol/L
- Total osmolarity: 245 mOsm/L (slightly hypotonic to plasma at 285)
The 1:1 sodium-to-glucose molar ratio is critical: glucose-coupled sodium absorption in the small intestine (the SGLT1 transporter) is the most rapid pathway for getting sodium into the body. Without glucose, sodium absorption is slow and incomplete; without sodium, intestinal glucose absorption is slow. Together, they synergize and water follows osmotically.
A homemade WHO ORS:
- 1 liter of water
- 1/2 teaspoon (~2.6 g) of table salt
- 6 teaspoons (~27 g) of sugar (sucrose or glucose)
- Optional: 1/2 cup of orange juice or coconut water for potassium
This is the standard formulation for diarrhea-related dehydration in pediatric settings worldwide and has saved millions of lives. For exercise-induced sodium depletion the same formulation is appropriate but the sodium concentration is often higher than athletes find palatable in race conditions, which is why most commercial sports drinks dilute it heavily.
For acute cramp scenarios, a more concentrated rescue formulation: 16 oz of water plus 1/4 teaspoon table salt (~580 mg sodium) plus 2 tablespoons of sugar or honey (~25 g glucose) plus 1/4 cup orange juice (~120 mg potassium) is a reasonable race-belt remedy that can be mixed at the aid station. The 580 mg of sodium is well above typical sports drink and is appropriate for someone who has already started cramping from depletion.
Commercial Products — LMNT, Nuun, Liquid IV, Gatorade
The electrolyte-drink commercial landscape is highly variable in sodium content and corresponding suitability for different uses:
- Gatorade Original (12 oz) — 160 mg sodium, 50 mg potassium, 21 g sugar. Designed for moderate-intensity exercise, somewhat under-dosed in sodium for endurance racing in heat. Adequate for an hour-long workout at moderate temperature, insufficient for marathon or Ironman conditions in heavy sweat.
- Liquid IV (1 stick in 16 oz water) — 500 mg sodium, 380 mg potassium, 11 g sugar. Marketed as a "hydration multiplier" using the WHO ORS sodium-glucose pathway. Reasonable for moderate sweat-loss scenarios; sodium content is appropriate for low-to-moderate sweat athletes but may still be light for heavy sweaters in extreme heat.
- LMNT (1 stick in 16 oz water) — 1000 mg sodium, 200 mg potassium, 60 mg magnesium, no sugar. The highest sodium content of the popular commercial sticks. Designed explicitly for low-carb / keto users (who lose more sodium due to reduced insulin-driven sodium retention) and for endurance athletes. The absence of carbohydrate is good for keto users but reduces the SGLT1-coupled sodium absorption rate; in pure athletic application, a small amount of co-administered carbohydrate improves uptake.
- Nuun Sport (1 tablet in 16 oz water) — 300 mg sodium, 150 mg potassium, 25 mg magnesium, 1 g sugar. A middle-of-the-road option. Light enough to drink throughout a long workout, adequate for moderate sweat losses.
- SaltStick capsules — concentrated electrolyte pills. SaltStick Plus has 215 mg sodium, 63 mg potassium, 22 mg calcium, 11 mg magnesium per capsule. Pair with plain water or low-sodium drink. Useful when sweat losses exceed what palatable drink concentrations can replace.
- Coconut water — 1 cup has 600 mg potassium, 250 mg sodium, 60 mg magnesium, 6 g sugar. Naturally formulated electrolyte solution. Not optimal for very high sweat-rate athletes (sodium is below sweat sodium) but a reasonable everyday hydration choice.
The general principle: match drink sodium content to sweat sodium content. If you are a heavy sweater (visible salt residue on clothing), you need a high-sodium drink (LMNT, SaltStick, or homemade strong ORS). If you are a light sweater, a moderate-sodium drink (Nuun, Liquid IV, coconut water) is fine. Plain Gatorade is fine for moderate workouts of an hour or less in mild conditions.
Matching Fluid Choice to Context
A decision tree by use-case:
- Office worker, normal day, 70°F: water is fine. 2-3 liters per day total fluid intake is more than adequate. Coffee and tea count toward total fluid; the "caffeine is dehydrating" myth has been disproven in habitual users.
- Recreational gym session, 45-60 minutes: water is sufficient. Electrolyte drink is not needed for hydration purposes (though some users prefer it for taste or carbohydrate for performance).
- Outdoor walk or moderate hike, 2-4 hours, mild weather: water plus a snack containing some sodium (a salted nut, a piece of cheese, etc.) is adequate.
- Endurance run, ride, or hike of 90+ minutes: use a sports drink or water plus salt tablet. Match electrolyte content to sweat rate. A reasonable target is 500-1000 mg sodium per hour of sustained exercise in heat.
- Marathon or Ironman race in heat: commit to a specific electrolyte strategy in training and execute it on race day. Common pitfall is over-drinking at the aid stations (drinking at each station "just in case") — this is the EAH pathway.
- Recovery from GI illness with vomiting or diarrhea: WHO ORS (commercial Pedialyte or homemade) is the appropriate fluid. Plain water alone delays recovery and can worsen electrolyte imbalance.
- Recovery from heavy alcohol use: water plus sodium plus carbohydrate (e.g., sports drink, broth-based soup with crackers) is more effective than water alone. Alcohol is a diuretic that depletes sodium, potassium, and magnesium.
- Older adult with chronic decreased thirst sensation: structured fluid intake on a schedule (a glass with each meal, mid-morning, mid-afternoon) rather than reliance on thirst. The elderly thirst mechanism is unreliable.
Hydration in Older Adults — The Other End of the Spectrum
While the endurance-athlete population over-drinks, the elderly population under-drinks. After age 70, thirst sensation declines, mobility limitations reduce trips to get water, nighttime nocturia drives intentional fluid restriction in the evening, and concentrating capacity of the kidney drops — all of which combine to produce chronic mild dehydration in many older adults.
Effects on cramping:
- Chronic mild volume contraction reduces tissue perfusion and may contribute to nocturnal calf cramps by reducing oxygenation of the chronically positioned (shortened) calf during sleep
- Elderly diuretic use (very common for hypertension and heart failure) compounds the volume contraction
- Chronic mild hyponatremia in some elderly patients (SIADH from various medications, congestive heart failure, hypothyroidism) directly contributes to muscle cramping at the lower end of the sodium range
For an elderly patient with nocturnal cramps, the hydration intervention is typically more water (in the daytime; less in the 3 hours before bedtime to avoid nocturia), not less. The intervention is also generally moderate — pushing to 2.5-3 L/day rather than 1.0-1.5 L/day, not the 4-5 L/day that would risk hyponatremia. Adequate dietary sodium (do not over-restrict for hypertension to the point of producing hyponatremia) and dietary potassium also help.
The geriatric cramp picture is dominated by chronic muscle shortening and magnesium status more than by hydration per se. See Stretch & Reset Techniques and Magnesium & Electrolytes for the higher-yield interventions in this population.
The Nocturnal-Cramp Context (Hydration Is Usually NOT the Answer)
The 3 AM gastrocnemius cramp that wakes the 65-year-old is not, in most cases, a hydration problem. The mechanisms are predominantly:
- Chronic calf shortening from sedentary daytime posture and prolonged sleeping positions
- Peripheral motor nerve hyperexcitability (sometimes drug-induced, sometimes age-related)
- Functional magnesium and potassium insufficiency (often)
- Occasionally drug-induced (statins, diuretics, donepezil, etc.)
Drinking a glass of water before bed does not address any of these and may make nocturia worse, which is itself a frequent contributor to poor sleep quality in older adults. The proper interventions for nocturnal leg cramps in this population are passive calf stretching (3 times daily), magnesium glycinate at bedtime, and medication review. Hydration is a tertiary consideration unless there is documented volume depletion.
The exception is the older adult who has been told (often by a well-meaning relative or popular media source) to drink 8+ glasses of water per day and is genuinely over-hydrating to a hyponatremic level. Reducing fluid intake (and getting a serum sodium check) is the intervention in that case. Symptoms of hyponatremia in the elderly often present as falls, confusion, and weakness rather than the classic muscle cramps.
Rehydration After GI Illness
Gastroenteritis with vomiting or diarrhea is the most common everyday context where serious electrolyte repletion matters. The fluid losses include water, sodium, chloride, potassium, and bicarbonate. Replacement with plain water can produce hypochloremic metabolic alkalosis and worsening hyponatremia.
Practical approach:
- Mild illness (a few episodes of diarrhea, no vomiting, adult with normal renal function) — commercial Pedialyte, Drip Drop ORS, or homemade WHO ORS (1L water, 1/2 tsp salt, 6 tsp sugar, optional juice) by sips, 100-200 mL per hour as tolerated
- Moderate illness (frequent diarrhea, some vomiting, mild orthostasis) — full WHO ORS at 100-200 mL per hour, plus broth-based foods (chicken soup, miso soup) as oral intake resumes
- Severe illness (persistent vomiting, hypotension, oliguria, altered mental status) — medical care, likely IV rehydration with isotonic saline
Post-illness cramping is common in the recovery phase as electrolyte stores normalize. Magnesium, potassium, and chloride all get depleted in significant GI illness and may take a week or more to fully replete via diet. Adding a daily magnesium glycinate dose during the recovery week and emphasizing potassium-rich foods (potatoes, beans, bananas, citrus) speeds recovery.
Cautions
- Do not over-hydrate during prolonged exercise — this is the EAH pitfall. Plan fluid intake to be slightly less than sweat losses (typical guidance is 400-800 mL per hour for endurance events, not the "drink at every aid station" pattern). Acceptable race-day weight change is 0 to -2%; weight gain during a race is a warning sign for EAH.
- Sodium-restricted patients (severe heart failure, advanced CKD, refractory hypertension) should not bulk-load sodium-rich electrolyte drinks. Endurance exercise in these patients requires individualized advice from their physician.
- Hyperkalemia risk — patients on ACE inhibitors, ARBs, potassium-sparing diuretics, or with renal insufficiency are at risk of hyperkalemia from potassium-rich oral electrolyte solutions and coconut water in significant volumes. The risk is small at moderate intake but real at heavy use.
- Diabetics — commercial sports drinks contain significant carbohydrate (Gatorade has 21 g per 12 oz; Liquid IV has 11 g per stick). For type 1 diabetics on insulin pumps, this is manageable with bolus dosing. For non-insulin-dependent type 2 diabetics, the carbohydrate load can produce significant glucose spikes. Sugar-free electrolyte options (LMNT, zero-sugar Nuun, electrolyte capsules) are alternatives.
- Hypertension — chronic high-sodium intake worsens hypertension in salt-sensitive individuals. Routine daily use of high-sodium electrolyte drinks (LMNT, SaltStick) outside of high-sweat athletic context is not appropriate for hypertensive patients.
- Pregnancy — standard sports drinks and ORS are safe in pregnancy at usual exercise volumes. The EAH risk in pregnancy is similar to non-pregnant adults but maternal hyponatremia is dangerous to the fetus.
- Coffee, tea, and alcohol — coffee and tea at moderate intake (3-4 cups/day) contribute net positively to total body water in habituated users; the older "diuretic effect" claim has been overstated. Alcohol is genuinely diuretic and depletes electrolytes; the "rehydrate during drinking" guidance (alternate with water, drink with food, hydrate the morning after) is sound.
Key Research Papers
- Almond CSD, Shin AY, Fortescue EB et al. (2005). Hyponatremia among runners in the Boston Marathon. New England Journal of Medicine. — PubMed 15829535
- Hew-Butler T, Rosner MH, Fowkes-Godek S et al. (2015). Statement of the Third International Exercise-Associated Hyponatremia Consensus Development Conference, Carlsbad, California, 2015. Clinical Journal of Sport Medicine. — PubMed 26102445
- Sawka MN, Burke LM, Eichner ER, Maughan RJ, Montain SJ, Stachenfeld NS (2007). American College of Sports Medicine position stand: Exercise and fluid replacement. Medicine & Science in Sports & Exercise. — PubMed 17277604
- Noakes TD, Speedy DB (2006). Case proven: exercise-associated hyponatraemia is due to overdrinking. British Journal of Sports Medicine. — Search PubMed
- Lau WY, Kato H, Nosaka K (2019). Water intake after dehydration makes muscles more susceptible to cramp but electrolytes reverse that effect. BMJ Open Sport & Exercise Medicine. — Search PubMed
- Eichner ER (2007). The role of sodium in "heat cramping". Sports Medicine. — Search PubMed
- Bergeron MF (2003). Heat cramps: fluid and electrolyte challenges during tennis in the heat. Journal of Science and Medicine in Sport. — Search PubMed
- Speedy DB, Thompson JM, Rodgers I, Collins M, Sharwood K, Noakes TD (2002). Oral salt supplementation during ultradistance exercise. Clinical Journal of Sport Medicine. — Search PubMed
- Maughan RJ, Shirreffs SM (2010). Dehydration and rehydration in competitive sport. Scandinavian Journal of Medicine & Science in Sports. PubMed: Maughan rehydration
- Schwellnus MP, Nicol J, Laubscher R, Noakes TD (2004). Serum electrolyte concentrations and hydration status are not associated with exercise associated muscle cramping in distance runners. British Journal of Sports Medicine. — Search PubMed
- Rosner MH, Kirven J (2007). Exercise-associated hyponatremia. Clinical Journal of the American Society of Nephrology. — Search PubMed
- Maughan RJ, Watson P, Cordery PA, Walsh NP, Oliver SJ, Dolci A, Rodriguez-Sanchez N, Galloway SDR (2016). A randomized trial to assess the potential of different beverages to affect hydration status. American Journal of Clinical Nutrition. — Search PubMed
PubMed Topic Searches
- PubMed: EAH in endurance racing
- PubMed: ORS sodium-glucose coupling
- PubMed: Sweat sodium and acclimation
- PubMed: Elderly hydration
- PubMed: Heat cramps and sodium
Connections
- Magnesium: The Mineral That Makes ATP Work — interactive animation
- Cramp Prevention Main Page
- Cramp Benefits Hub
- Magnesium & Electrolytes
- Pickle Juice & Neural Reflex
- Stretch & Reset Techniques
- Sodium
- Potassium
- Magnesium
- Chloride
- Hyponatremia
- Dehydration
- Coconut Water
- Bananas
- Bone Broth
- All Remedies