Stretch and Reset Techniques for Cramp Prevention
Passive stretching is the single intervention with the strongest randomized-controlled-trial evidence for reducing the frequency of nocturnal leg cramps in older adults. The Hallegraeff 2012 trial showed that a simple bedtime calf and hamstring stretch routine cut nocturnal cramp frequency by approximately 60% over 6 weeks in adults over 55. That effect size is larger than what magnesium achieves in the same population in most trials — making stretching the first-line intervention by an evidence-based standard, not the after-thought it is often treated as. For acute cramps, contract-relax (PNF) stretching of the cramping muscle terminates the cramp within 10-30 seconds by activating Golgi tendon organ inhibition. For chronic cramping in athletes or patients with myofascial restrictions, foam rolling adds a complementary self-myofascial release component. This page covers the protocol, the mechanism, the variations, and the limits of stretching as a cramp-prevention tool.
Interactive Visualization Magnesium — the mineral that makes ATP work Bare ATP is useless and enzymes reject it. Watch magnesium clamp the phosphates and switch it on, plug the NMDA channel, and let a cramping muscle finally let go. Launch →
Table of Contents
- The Hallegraeff Bedtime Stretch Protocol
- Why Stretching Works — The Golgi Tendon & Length-Tension Mechanisms
- Calf-Stretch Anatomy — Gastrocnemius vs Soleus
- Contract-Relax (PNF) for Acute Cramp Termination
- Hamstring Stretches for Posterior-Chain Cramping
- Foot Arch & Plantar Cramps
- Foam Rolling & Self-Myofascial Release
- Pre-Workout vs Post-Workout Stretching
- Chronic Calf Shortening & Why Sedentary Lifestyle Drives Cramps
- Combining Stretching With Magnesium and Other Interventions
- Cautions
- Key Research Papers
- Connections
- Featured Videos
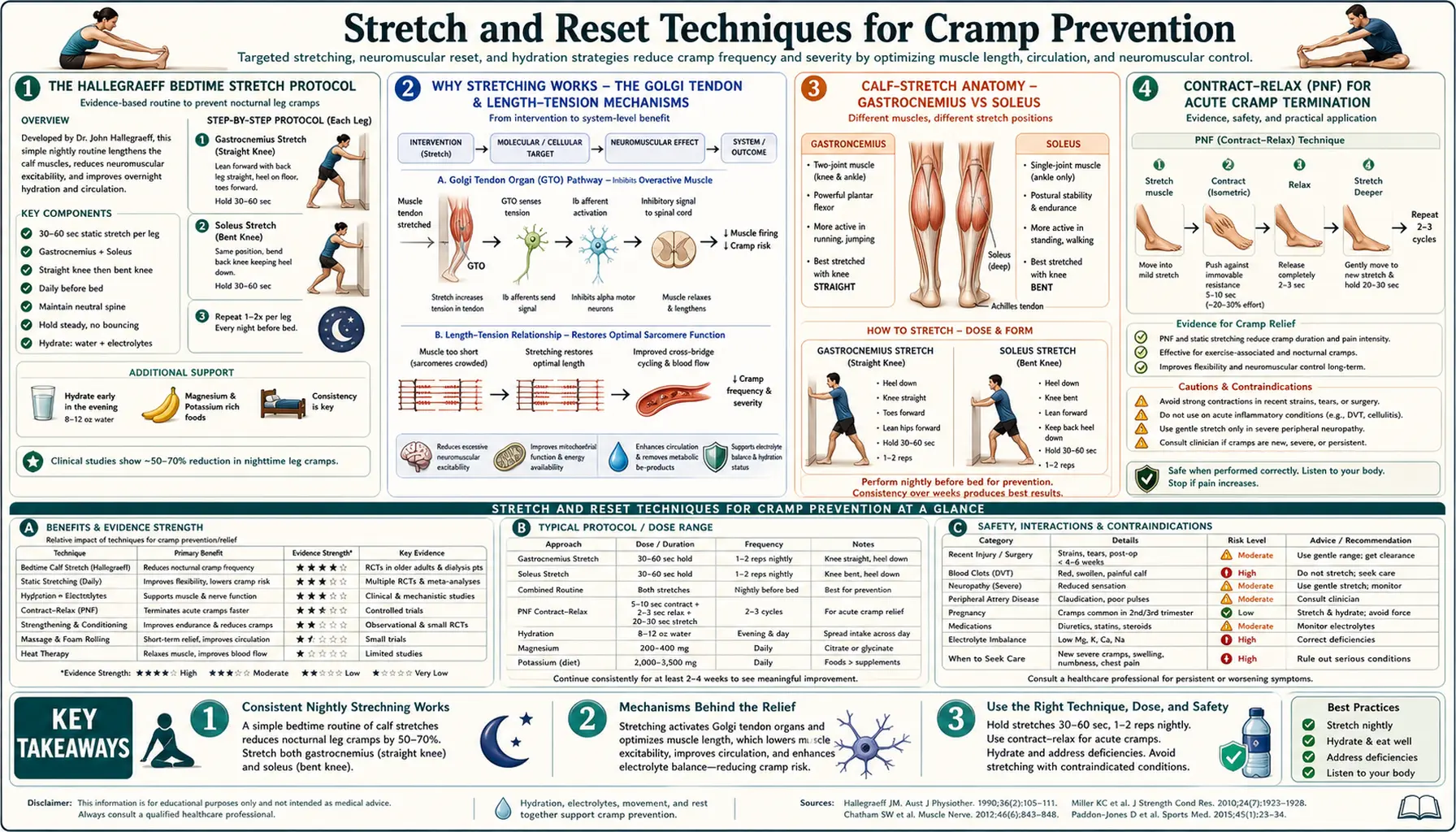
The Hallegraeff Bedtime Stretch Protocol
Joannes Hallegraeff and colleagues at the Saxion University of Applied Sciences in the Netherlands published the most influential modern stretching-for-cramps trial in 2012 in Journal of Physiotherapy. The study design and results:
- Population: 80 adults over 55 with frequent nocturnal leg cramps (more than 1 per week on average)
- Intervention arm: standardized bedtime stretching of the calves and hamstrings, performed within 5 minutes of going to bed, every night for 6 weeks
- Control arm: no specific intervention
- Outcomes: nocturnal cramp frequency and severity
- Results: the stretching group had a substantial reduction in cramp frequency (the mean number of nocturnal cramps per week dropped from ~3.0 to ~1.2) and a reduction in cramp severity. Control group cramp frequency was essentially unchanged.
The exact protocol Hallegraeff used (worth reproducing because the trial result depends on consistency):
- Calf stretch (gastrocnemius) — stand facing a wall at arm's length. Place hands on the wall at shoulder height. Step one foot back, keeping the heel on the floor and the back leg straight. Lean forward at the hips until a clear stretch is felt in the back calf. Hold for 10 seconds. Switch legs. Repeat once on each side (total 4 holds, 2 per side).
- Hamstring stretch — sit on the floor with one leg extended straight forward and the other bent with the sole resting against the inner thigh. Reach forward toward the extended foot, keeping the back relatively straight (do not round the spine). Hold for 10 seconds. Switch legs. Repeat once on each side.
- Total time: approximately 3-5 minutes
- Timing: within 5 minutes of going to bed (proximity matters — the stretches done in the morning do not appear to produce the nocturnal-cramp protection)
- Frequency: every night, indefinitely. Skipping nights reduces the cumulative benefit.
The simplicity of the protocol is what makes it work. It takes less than 5 minutes, requires no equipment, and the only practical barrier is consistency. Many patients prefer to do it as the last step before lying down; doing it immediately after a hot shower (warm tissue stretches more easily) is also reasonable.
Daniel HW had described essentially the same protocol decades earlier in a 1979 case-report paper in JAMA, "Simple cure for nocturnal leg cramps." Daniel reported anecdotal but consistent cramp resolution in his clinical practice using a similar wall-lean calf stretch performed three times daily. The Hallegraeff trial provided the RCT confirmation 33 years later.
Why Stretching Works — The Golgi Tendon & Length-Tension Mechanisms
Two physiological mechanisms explain why stretching reduces nocturnal cramp frequency:
- Acute Golgi tendon organ inhibition — the Golgi tendon organ (GTO) is a mechanoreceptor in the musculotendinous junction that senses tension in the tendon. When stretched, the GTO sends signals via Ib afferents to inhibitory Ib interneurons in the spinal cord, which inhibit the alpha-motoneurons that supply the same muscle. This is the autogenic inhibition reflex. Passive stretching activates this loop and reduces motoneuron excitability for the next 15-60 minutes. Performing the stretch within 5 minutes of going to bed brings the calf alpha-motoneuron pool into the sleep period with reduced baseline excitability, raising the threshold for spontaneous cramp.
- Chronic length-tension reset — muscles that are kept chronically short (calves in habitual high-heel wearers, hamstrings in habitual sitters) develop sarcomere adaptation: the number of sarcomeres in series decreases over months to years, and the resting length of the muscle shortens. A shortened muscle operates further to the right of its optimal length-tension curve, becomes less efficient, and is more prone to cramping under any provocation. Consistent daily stretching slowly reverses this adaptation by adding sarcomeres in series and lengthening the muscle's resting state, which both reduces baseline tension and shifts the operating point back toward the optimal length-tension region.
The acute Golgi tendon mechanism explains why the timing matters — the inhibitory effect of an evening stretch persists into the early hours of sleep, when most nocturnal cramps occur. The chronic length-tension reset explains why benefit builds over weeks of consistent practice rather than appearing on the first night.
The same Golgi tendon mechanism is the basis for the Khan and Burne 2007 demonstration that direct electrical stimulation of a tendon will abort a cramp in the corresponding muscle. The Bertolasi et al. 1993 work showed that muscle lengthening directly inhibits cramp generation in real time. The stretch-for-cramps practice has solid physiological grounding even before the RCT evidence.
Calf-Stretch Anatomy — Gastrocnemius vs Soleus
The "calf" is two muscles, not one, with different cramping patterns and different optimal stretches:
- Gastrocnemius — the larger, superficial calf muscle. Crosses both the knee and ankle joints. Has two heads (medial and lateral) that originate from the femoral condyles and converge to the Achilles tendon. Because it crosses the knee, it is fully stretched only with the knee extended (straight). The Hallegraeff wall-lean stretch with the back leg straight is a gastrocnemius stretch.
- Soleus — the deeper, broader calf muscle. Originates from the tibia and fibula below the knee. Joins the gastrocnemius at the Achilles tendon. Because it does not cross the knee, the soleus is selectively stretched by bending the knee while keeping the heel on the floor. The bent-knee wall lean (or seated stretch with the foot pulled toward the body) targets the soleus.
Most nocturnal calf cramps involve both muscles, and the standard protocol should include both stretches:
- Straight-knee wall lean (gastrocnemius) — 10 seconds × 2-3 reps per side
- Bent-knee wall lean (soleus) — 10 seconds × 2-3 reps per side
- Combined session: 2-4 minutes per night
A particularly common mistake is to do only the straight-knee stretch and ignore the soleus. The soleus is the postural calf muscle (it does most of the standing work) and is the more chronically shortened muscle in sedentary adults. Including the bent-knee variation in the routine catches the soleus.
For runners and walkers, an alternative single-position stretch is the runner's calf stretch off a step: stand with the toes on the edge of a step and let the heels drop below the level of the step. Hold 15-30 seconds. This stretches both gastrocnemius (knee straight) and soleus (slight knee bend variant) and is a useful pre-run warmup.
Contract-Relax (PNF) for Acute Cramp Termination
For an acute cramp already in progress, simple passive stretching often terminates it, but proprioceptive neuromuscular facilitation (PNF) is faster. PNF exploits two reflex pathways simultaneously: autogenic inhibition (the GTO loop from contracting the cramping muscle) and reciprocal inhibition (from contracting the antagonist).
For an acute gastrocnemius cramp, the contract-relax-stretch protocol:
- Find a position where you can hold the foot and pull the forefoot toward the shin (dorsiflexing the ankle). Sitting on the bed grabbing the toes is the standard nocturnal position; in a race, leaning against a wall with the heel on the floor and toes against the wall works.
- Contract phase: contract the cramping muscle isometrically for 5-10 seconds against light resistance — push the ball of the foot down into your hand or against the floor. This sounds counterintuitive (you would think you want to relax the cramping muscle, not contract it) but the sustained contraction provokes the Golgi tendon reflex and triggers autogenic inhibition.
- Relax phase: stop the contraction. The muscle is now reflexively inhibited.
- Stretch phase: immediately stretch the muscle further (pull the toes toward the shin more aggressively) while the inhibition is active. Hold for 15-20 seconds.
- Reciprocal contract: while in the stretch, contract the antagonist (the tibialis anterior, which dorsiflexes the foot) actively. This adds reciprocal inhibition to the autogenic inhibition.
- Typically the cramp releases within one PNF cycle. Repeat once if needed.
For other muscle cramps, the same principle applies:
- Hamstring cramp: sit, extend the leg, gently pull the toes toward the body (lengthening the hamstring). Contract the hamstring by pushing the heel down for 5 seconds. Relax. Pull deeper into the stretch. Add an active quad contraction (extending the knee further) for reciprocal inhibition.
- Quadriceps cramp: stand, hold one ankle behind the buttock to flex the knee fully (lengthening the rectus femoris). Contract the quad by pushing the foot down against the hand. Relax, deepen the stretch. Add active hamstring contraction.
- Foot arch cramp: place the heel on the floor, lift the toes upward (extending the toes and stretching the plantar fascia and intrinsic foot muscles). Contract the foot muscles by trying to curl the toes against resistance. Relax, deepen the stretch.
The Sharman et al. 2006 review in Sports Medicine covers PNF mechanisms in detail. The technique is widely used in sports physiotherapy and is the fastest reliable method to terminate an acute cramp through mechanical means alone.
Hamstring Stretches for Posterior-Chain Cramping
Hamstring cramps are less common than calf cramps in the general population but are very common in cyclists, hockey players, and sprinters whose training emphasizes posterior-chain power output. The Hallegraeff protocol included hamstring stretches because the hamstrings are a frequent secondary cramp site that often accompanies calf cramping in older adults.
Useful hamstring stretches:
- Seated forward fold — sit on the floor with both legs extended forward. Reach for the toes, keeping the back relatively straight (do not round the lumbar spine). Hold 15-30 seconds. Most basic, accessible, and the variant used in Hallegraeff.
- Single-leg seated reach — sit with one leg extended and the other bent, sole against the inner thigh. Reach for the extended foot. Allows asymmetric work if one side is tighter.
- Doorway leg lift — lie on the floor in a doorway. Lift the inside leg straight up the door frame, keeping the outside leg flat through the doorway. The wall supports the lifted leg passively without needing to actively hold it up. Hold 1-3 minutes per side. A more sustained stretch suitable for chronic tight hamstrings.
- Standing forward fold — stand with feet hip-width apart, slowly bend forward at the hips with knees soft (slightly bent). Let the upper body hang. Stretches hamstrings and lower back together. Hold 30-60 seconds. Particularly good first thing in the morning to release overnight tightness.
For people with low back pain or disc issues, the loaded seated forward fold can aggravate the back; the doorway leg lift is a safer alternative because it doesn't require lumbar flexion against gravity.
Foot Arch & Plantar Cramps
Plantar foot cramps (cramps in the arch of the foot) are a distinct presentation that often gets lumped with calf cramps but has its own pattern. Common in people who stand for long periods (teachers, nurses, cooks), high-arched runners, and people with chronic plantar fasciitis.
Stretches and exercises that target the plantar fascia and intrinsic foot muscles:
- Standing toe extension — stand with the toes of one foot bent up against a wall or step, heel on the floor. Lean forward to deepen the stretch. Hold 30 seconds. Targets the plantar fascia.
- Frozen water bottle roll — sit, place a frozen water bottle under the arch of the foot, and roll the foot back and forth over the bottle for 1-2 minutes. Combines stretching with cold therapy. Particularly good for plantar fasciitis-driven foot cramping.
- Toe spreads — actively spread the toes apart and hold for 5 seconds, then release. Repeat 10 times. Strengthens the intrinsic foot muscles and reduces their cramping tendency. Many people have nearly atrophied intrinsic foot muscles from a lifetime of wearing shoes that immobilize the toes; toe spreads are a basic rehabilitative exercise.
- Towel curls — sit with a small towel flat on the floor in front of you. Use the toes to scrunch the towel toward you. Continue until the towel is fully gathered. Strengthens intrinsic foot muscles.
- Calf raises — standing calf raises (rising onto the toes and lowering slowly) build calf strength and indirectly support the arch. 3 sets of 15-20 reps daily.
For chronic plantar cramps, the combination of stretching (plantar fascia and toes), strengthening (towel curls, toe spreads), and footwear modification (shoes with adequate toe-box width and modest arch support, but not maximal cushioning that immobilizes the foot) addresses the underlying mechanical issue. Standing on a soft mat at work for those who spend hours on concrete floors reduces the chronic foot fatigue that drives plantar cramping.
Foam Rolling & Self-Myofascial Release
Foam rolling is a form of self-myofascial release that uses a cylindrical foam roller (or harder lacrosse ball for more focused pressure) to apply sustained compressive force to muscle and fascia. The mechanism is debated but appears to involve a combination of Golgi tendon activation, descending neural inhibition, fascial mobility improvement, and increased local blood flow.
For cramp prevention, foam rolling adds a complementary dimension to passive stretching:
- Calf roll — sit on the floor with the roller under the calves. Use the arms to lift the body slightly, then roll the calf over the roller from just below the knee to just above the Achilles. 1-2 minutes per side. Add pressure by crossing the other leg over the calf being rolled.
- Hamstring roll — sit with roller under the hamstrings. Roll from the glute crease to just above the knee. 1-2 minutes per side.
- Quad roll — lie face-down with the roller under the front of the thighs. Roll from the hip to just above the knee. Use the elbows to control the body weight applied. 1-2 minutes per side.
- Plantar fascia ball — stand or sit and roll a tennis or lacrosse ball under the foot arch. 1-2 minutes per side.
The Cheatham et al. 2015 systematic review in International Journal of Sports Physical Therapy found that foam rolling produces short-term improvements in flexibility without subsequent strength loss, and may reduce delayed-onset muscle soreness after exercise. Specific cramp-prevention RCTs of foam rolling are scarce, but the mechanism is plausible and the practice is low-risk.
The timing of foam rolling: pre-workout (1-2 minutes per major muscle group) as part of warm-up, and/or post-workout for recovery. For nocturnal cramp prevention, evening foam rolling (15-30 minutes before bed, combined with the Hallegraeff stretches) is a reasonable addition to the protocol.
Pre-Workout vs Post-Workout Stretching
The role of stretching around workouts has been controversial for two decades. The current evidence-based picture:
- Static stretching immediately before high-power exertion (sprinting, heavy lifting, plyometrics) modestly reduces immediate power output for the next 15-30 minutes. The mechanism is post-stretch reduction in tendon stiffness and motor unit recruitment. Magnitude of effect is small (typically <5%) but real. For pure-power athletes, static stretching is better placed after the workout than before.
- Dynamic stretching before exercise (leg swings, walking lunges, dynamic mobility drills) has no power-decrement effect and may improve performance through warm-up effects. This is the preferred pre-workout protocol for sports requiring power output.
- Static stretching after exercise does not appear to meaningfully reduce delayed-onset muscle soreness (DOMS), contrary to long-held belief. The Cochrane review on stretching for DOMS prevention is essentially negative. But post-workout stretching does help maintain flexibility over time and may reduce post-workout muscle tightness.
- Static stretching for nocturnal cramp prevention (Hallegraeff protocol) is the application where static stretching has clear RCT evidence. Done at bedtime, separated from any athletic performance window, the negative power effects are irrelevant.
The "do not stretch before running" advice that swept popular fitness writing in the 2010s is overstated. For recreational endurance running at sub-maximal intensity, the modest power decrement from pre-run stretching does not matter. For competitive sprinting, it matters. Use context to decide.
For cramp prevention specifically, the relevant stretching window is daily and bedtime, not workout-adjacent. The Hallegraeff protocol works regardless of athletic context or athletic timing.
Chronic Calf Shortening & Why Sedentary Lifestyle Drives Cramps
The deeper mechanism behind nocturnal leg cramps in older adults is chronic calf shortening from a lifetime of habitual postures: sitting at a desk, sleeping with toes pointed down (the prone or side-lying position naturally plantarflexes the foot for 6-8 hours per night), and wearing shoes with even modest heel elevation that keeps the calf in a slightly shortened position throughout the day.
Over years, the gastrocnemius and soleus adapt by reducing the number of sarcomeres in series, shortening the resting length, and reducing maximal extensibility. The result is a calf muscle that operates at a shorter than optimal length during walking, runs out of safe range during stretching, and has less reserve before passing the threshold for cramping.
Interventions for chronic calf shortening:
- Daily passive stretching as described above (Hallegraeff protocol) — the slow, sustained approach
- Standing desks or sit-stand alternation — standing keeps the calf at a more functional length than sitting, particularly when standing with the heels flat (no shoes or flat shoes). Even small amounts of standing throughout the workday help.
- Zero-drop or minimalist footwear for daily wear — reducing the heel-to-toe drop in everyday shoes allows the calf to operate at its full functional length. The transition should be gradual (over weeks to months) to avoid Achilles tendinopathy from sudden lengthening.
- Sleeping position modification — some patients with severe nocturnal cramping benefit from sleeping with a small pillow under the feet that keeps the ankles in neutral (not plantarflexed) position, or from wearing a soft night splint that maintains a 90-degree ankle angle. The night-splint approach is more common in plantar fasciitis but is occasionally useful for cramp-prone calves.
- Avoiding high heels — for women who have worn heels regularly for years, the calf shortening can be substantial. Gradual transition to lower-heel footwear over months allows the calves to lengthen safely.
- Yoga and Pilates — the asana practice in yoga (downward dog, standing forward fold, gomukhasana) and many Pilates exercises target the same posterior-chain lengthening that the Hallegraeff stretches address, in a more comprehensive way. 2-3 sessions per week is a reasonable adjunct.
For more on the broader anti-sedentary lifestyle approach, see our Walking Exercise page.
Combining Stretching With Magnesium and Other Interventions
The clinically pragmatic approach to nocturnal leg cramps in adults over 55 is to start the Hallegraeff stretch protocol and a 6-week trial of magnesium glycinate simultaneously. The Cochrane review evidence base is stronger for stretching than for magnesium, but both are low-risk, both target different mechanisms (stretching addresses Golgi tendon excitability and chronic muscle shortening; magnesium addresses cellular ATP-Mg substrate availability and motoneuron NMDA-receptor excitability), and the combined effect appears greater than either alone in clinical practice.
A complete first-line cramp-prevention plan:
- Stretching: Hallegraeff calf + hamstring protocol at bedtime, every night, for 6 weeks minimum to assess effect
- Magnesium: magnesium glycinate 350-500 mg elemental at bedtime, for 6 weeks minimum
- Diet: emphasize magnesium-rich foods (pumpkin seeds, almonds, spinach, dark chocolate), potassium-rich foods (potatoes, beans, bananas, citrus, salmon), adequate but not excessive water
- Medication review: identify statins, diuretics, PPIs, donepezil, beta-agonists as potential contributors; discuss alternatives with prescribing clinician where possible
- Footwear: reduce heel height in daily shoes, consider zero-drop or minimalist shoes for casual wear
- Daytime calf use: standing desk, regular walking breaks, less sitting
- Sleep position: avoid sleeping with toes pointed down for prolonged periods; consider supine sleep with small pillow under knees
If after 6 weeks the cramps are unimproved, the next steps include: lab work (serum magnesium plus RBC magnesium, potassium, calcium, 25-OH-vitamin D, TSH, CBC, BMP), peripheral neurology evaluation if there are other neurologic features (weakness, sensory changes, fasciculations), sleep study for restless legs / Willis-Ekbom disease, and pharmacologic options under physician supervision (the Katzberg AAN guideline summarizes the limited options: gabapentin, mexiletine, naftidrofuryl, diltiazem — with quinine reserved for refractory cases due to the FDA thrombocytopenia warning).
Cautions
- Acute injury — do not stretch a freshly strained muscle. Stretching a torn muscle worsens the injury. Wait 48-72 hours after a significant strain before resuming stretching, and start gently.
- Achilles tendinopathy — aggressive calf stretching in the presence of an Achilles tendinopathy can flare the tendon. Use the eccentric heel-drop protocol (Alfredson protocol) instead under physical therapist guidance for that specific condition.
- Recent orthopedic surgery — defer to surgeon's post-op stretching protocols for the affected joint.
- Hypermobility — patients with Ehlers-Danlos syndrome, hypermobility-spectrum disorder, or constitutional joint laxity may not benefit from aggressive stretching and can develop subluxations. Strengthening typically takes priority over stretching in this population.
- Osteoporosis — avoid forced-flexion stretches (deep forward folds with rounded back) which can stress the thoracolumbar spine and risk vertebral compression fracture. Modified stretches that keep the back relatively straight are safer.
- Pregnancy — in late pregnancy, avoid deep supine stretches (vena cava compression). Side-lying or seated variants are preferable. The Hallegraeff calf stretch (standing wall lean) is fine throughout pregnancy.
- Pain during stretching — stretching should produce a mild-to-moderate "good stretch" sensation, never sharp pain. Sharp pain indicates either overstretching or an underlying injury and should prompt stopping.
- Holding too long — in healthy adults, holds longer than 60 seconds per position do not produce additional benefit. The Hallegraeff 10-second protocol is at the short end of the range; up to 30-45 seconds per hold is fine if preferred. Beyond that, you are just spending time without additional gain.
- Consistency over duration — 5 minutes of stretching every night for 6 weeks beats 60 minutes of stretching three times in 6 weeks. The protocol depends on daily repetition.
Key Research Papers
- Hallegraeff JM, van der Schans CP, de Ruiter R, de Greef MH (2012). Stretching before sleep reduces the frequency and severity of nocturnal leg cramps in older adults: a randomised trial. Journal of Physiotherapy. — Search PubMed
- Daniel HW (1979). Simple cure for nocturnal leg cramps. JAMA. — Search PubMed
- Coppin RJ, Wicke DM, Little PS (2005). Managing nocturnal leg cramps—calf-stretching exercises and cessation of quinine treatment: a factorial randomised controlled trial. British Journal of General Practice. — Search PubMed
- Allen RE, Kirby KA (2012). Nocturnal leg cramps. American Family Physician. — Search PubMed
- Khan SI, Burne JA (2007). Reflex inhibition of normal cramp following electrical stimulation of the muscle tendon. Journal of Neurophysiology. — Search PubMed
- Bertolasi L, De Grandis D, Bongiovanni LG, Zanette GP, Gasperini M (1993). The influence of muscular lengthening on cramps. Annals of Neurology. — Search PubMed
- Sharman MJ, Cresswell AG, Riek S (2006). Proprioceptive neuromuscular facilitation stretching: mechanisms and clinical implications. Sports Medicine. — Search PubMed
- Page P (2012). Current concepts in muscle stretching for exercise and rehabilitation. International Journal of Sports Physical Therapy. — PubMed 22319684
- Cheatham SW, Kolber MJ, Cain M, Lee M (2015). The effects of self-myofascial release using a foam roll or roller massager on joint range of motion, muscle recovery, and performance: a systematic review. International Journal of Sports Physical Therapy. — PubMed 26618062
- Katzberg HD, Khan AH, So YT (2010). Assessment: symptomatic treatment for muscle cramps (an evidence-based review): report of the therapeutics and technology assessment subcommittee of the American Academy of Neurology. Neurology. — Search PubMed
- Garrison SR, Dormuth CR, Morrow RL, Carney GA, Khan KM (2012). Nocturnal leg cramps and prescription use that precedes them: a sequence symmetry analysis. Archives of Internal Medicine. — Search PubMed
- Maisonneuve H, Chambe J, Delacour C et al. (2016). Prevalence of cramps in patients over the age of 60 in primary care: a cross sectional study. BMC Family Practice. PubMed: Maisonneuve cramp prevalence
PubMed Topic Searches
- PubMed: Stretching nocturnal cramp RCTs
- PubMed: Golgi tendon autogenic inhibition
- PubMed: PNF stretching
- PubMed: Foam rolling research
- PubMed: Calf sarcomere adaptation
Connections
- Magnesium: The Mineral That Makes ATP Work — interactive animation
- Cramp Prevention Main Page
- Cramp Benefits Hub
- Magnesium & Electrolytes
- Pickle Juice & Neural Reflex
- Hydration Beyond Water
- Yoga
- Walking Exercise
- Pilates
- Plantar Fasciitis
- Achilles Tendinopathy
- Restless Legs Syndrome
- Peripheral Neuropathy
- Magnesium
- Potassium
- All Remedies