Cold and Flu Natural Treatments — Benefits Deep Dive
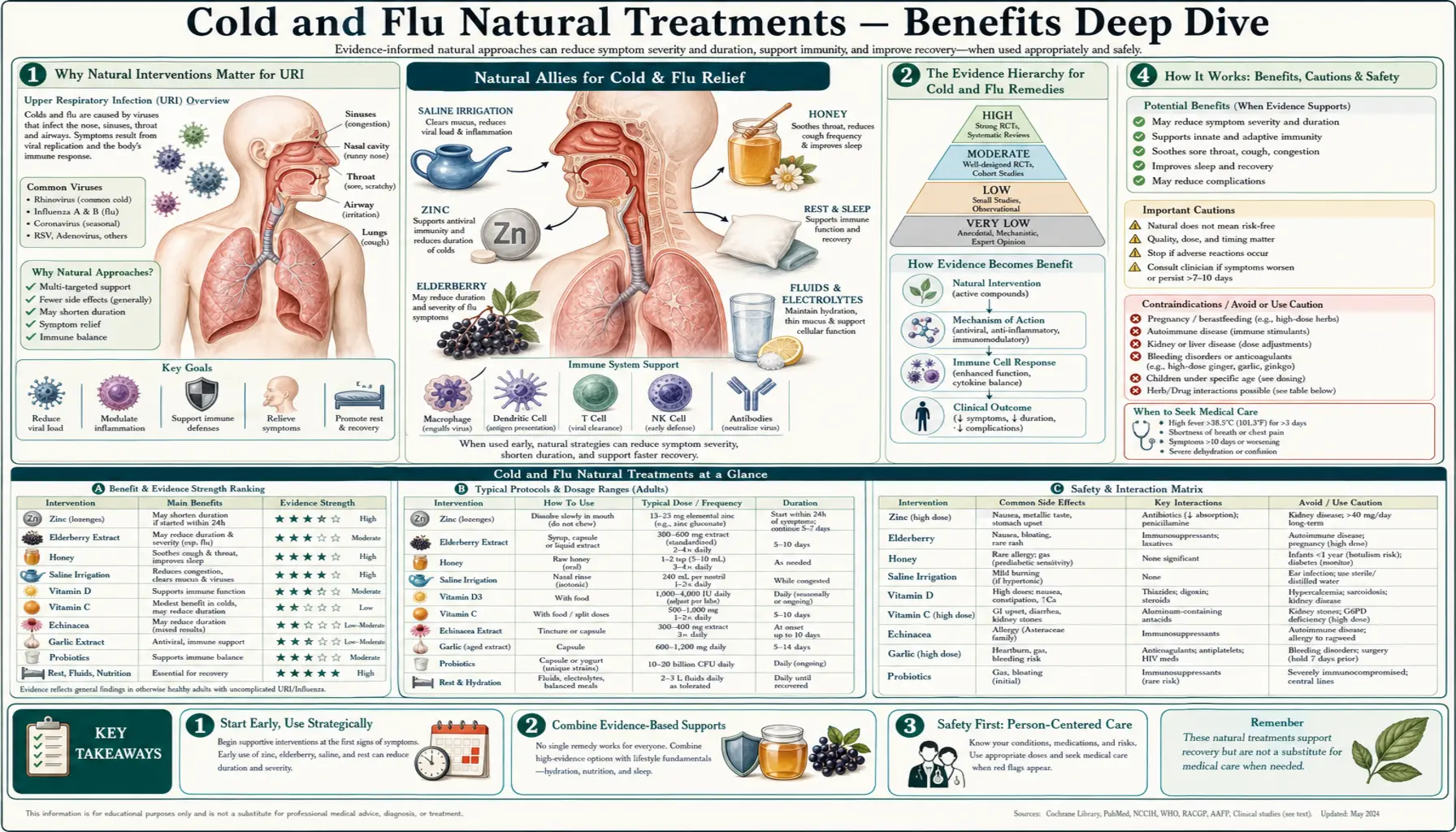
Acute upper respiratory infection (URI) is the single most common reason American adults miss work and children miss school. Roughly 200 distinct virus serotypes (rhinoviruses, influenza A/B, respiratory syncytial virus (RSV), parainfluenza, adenoviruses, and seasonal endemic coronaviruses) cycle through the population each year, and the typical adult experiences two to four episodes annually. Conventional medicine offers oseltamivir (Tamiflu) and baloxavir (Xofluza) for confirmed influenza inside a 48-hour treatment window, and no specific antiviral therapy at all for the common cold. That treatment gap is what creates the demand for the four evidence-supported natural interventions explored in the deep-dive pages below — zinc acetate lozenges that shorten cold duration by approximately 33%, Vitamin D repletion that halves acute respiratory infection risk in deficient adults, elderberry extract that compresses influenza symptom duration in randomized trials, and the mechanical interventions (steam inhalation, hypertonic saline rinses, neti-pot irrigation) that physically clear viral particles and reduce sinus burden.
Deep-Dive Articles
Zinc Acetate Lozenges
The Hemila meta-analyses, the 80–92 mg/day elemental zinc dosing window, why acetate or gluconate (not citrate or oxide), the 24-hour symptom-onset rule, why ionic free Zn2+ in the oropharynx matters more than systemic zinc status, the rhinovirus ICAM-1 docking mechanism, palatability tradeoffs, and the consensus that lozenges shorten the common cold by roughly one-third.
Vitamin D Status and Respiratory Infection
The Martineau IPD meta-analysis (25,000+ participants) showing daily or weekly Vitamin D reduces acute respiratory infection risk by approximately 12% overall and roughly 70% in profoundly deficient adults, the cathelicidin LL-37 antimicrobial peptide mechanism, the 25-hydroxyvitamin D target of 40–60 ng/mL, daily/weekly dosing superior to monthly boluses, and the seasonal latitude pattern that drives the winter respiratory-infection peak.
Elderberry and Antiviral Activity
The Sambucus nigra randomized trials (Zakay-Rones 1995 Israel, Zakay-Rones 2004, Tiralongo 2016 air travel), the anthocyanin-driven hemagglutinin inhibition mechanism, the standardized syrup (Sambucol) and lozenge dosing, why the autoimmune-cytokine concern is theoretical rather than observed, the 48-hour symptom compression in influenza, and how to distinguish standardized extracts from low-anthocyanin commodity products.
Steam Inhalation and Saline Rinses
The mechanical removal of viral particles, antigens, and inflammatory mediators from the nasal mucosa by hypertonic saline irrigation, the ELVIS pragmatic trial showing reduced symptom duration and onward transmission, neti-pot vs squeeze-bottle vs powered irrigation, the safe sterile-water rule (boiled, distilled, or commercial saline only — never tap), Eucalyptus / Tea Tree adjuncts, steam-tent technique, humidifier hygiene, and where the evidence for menthol decongestion stands.
Table of Contents
- Deep-Dive Articles
- Why Natural Interventions Matter for URI
- The Evidence Hierarchy for Cold and Flu Remedies
- Research Papers: Zinc Lozenges
- Research Papers: Vitamin D and Respiratory Infection
- Research Papers: Elderberry and Antiviral Activity
- Research Papers: Steam, Saline, and Mechanical Interventions
- Research Papers: Cross-Cutting (Cold/Flu Epidemiology, Adjunct Nutrients)
- External Authoritative Resources
- Connections
- Featured Videos
Why Natural Interventions Matter for URI
Acute upper respiratory infection is one of the few illness categories where evidence-supported natural interventions consistently outperform what conventional medicine offers. There are four reasons.
- The conventional toolkit is thin. Oseltamivir (Tamiflu) and baloxavir (Xofluza) are useful only for laboratory-confirmed influenza A or B inside a 48-hour treatment window. By the time most people see a doctor for "flu-like illness," that window has closed and the typical patient does not have a virologically confirmed influenza strain anyway — they have one of dozens of circulating respiratory viruses (rhinovirus, RSV, parainfluenza, seasonal endemic coronavirus, metapneumovirus). For the common cold (overwhelmingly rhinovirus), there is no approved specific antiviral therapy at all in 2026.
- The pathophysiology is favorable for nutritional intervention. URI symptoms arise less from direct viral cytopathic effect and more from the host inflammatory response — cytokine release, mucus hypersecretion, vasodilation. Interventions that modulate barrier function (Vitamin D, mucosal IgA via Vitamin A), reduce viral attachment (zinc binding to rhinovirus ICAM-1), or directly inhibit viral entry (elderberry anthocyanins blocking hemagglutinin) all operate on this pathophysiology rather than requiring strain-specific antiviral activity.
- The risk profile is excellent. Zinc lozenges, Vitamin D repletion, elderberry syrup, and saline nasal irrigation all have established safety profiles spanning decades of use. The narrowest therapeutic windows are zinc (chronic intake >40 mg/day depletes copper) and Vitamin D (intake >10,000 IU/day for months risks hypercalcemia), but neither is approached by typical cold/flu dosing.
- Cost and accessibility favor self-care. A bottle of zinc acetate lozenges, a bottle of standardized elderberry syrup, a Vitamin D blood test plus a year of D3 capsules, and a neti pot together cost less than a single urgent-care copay in the United States. For a household experiencing 6–12 URI episodes per year between children and adults, the math is compelling.
The four deep-dive pages below each explore one intervention in detail: the mechanism, the randomized-trial evidence, the dosing window that worked in trials, the populations who benefited most, and the cautions.
The Evidence Hierarchy for Cold and Flu Remedies
Not all "natural cold remedies" have the same evidence base. A useful three-tier hierarchy:
Tier 1 — Multiple randomized trials and meta-analyses
- Zinc acetate / gluconate lozenges (Hemila Cochrane review 2013, JRSM Open 2017 meta-analysis): roughly 33% reduction in common-cold duration when started within 24 hours of symptom onset at 80–92 mg/day elemental zinc divided across the day.
- Vitamin D supplementation (Martineau et al. individual-patient-data meta-analysis 2017, BMJ): approximately 12% overall reduction in acute respiratory infection risk, rising to ~70% in profoundly deficient adults receiving daily or weekly D3.
- Hypertonic saline nasal irrigation (Ramalingam et al. ELVIS trial 2019, Scientific Reports): reduced URI duration by 1.9 days and reduced household transmission by ~35% in a pragmatic randomized trial.
Tier 2 — Small randomized trials with consistent direction of effect
- Elderberry extract (Zakay-Rones 1995, 2004; Tiralongo 2016): symptom-duration compression in influenza, consistent direction across small trials, mechanistic plausibility from anthocyanin hemagglutinin inhibition.
- Echinacea purpurea (Karsch-Volk Cochrane 2014): heterogeneous trials, some positive for prevention but small effect sizes; species and preparation matter (E. purpurea aerial parts vs E. angustifolia root).
- Andrographis paniculata: several small trials showing symptom reduction in URI.
- Pelargonium sidoides (EPs 7630, Umckaloabo): meta-analyses suggesting modest benefit in acute bronchitis.
Tier 3 — Mechanism plus historical use, sparse modern trial data
- Garlic (allicin), ginger, oregano oil, propolis, Vitamin A repletion for measles or low-status populations, larch arabinogalactan, beta-glucans.
The four deep-dive pages on this site focus on Tier 1 (zinc, Vitamin D, saline irrigation) plus the strongest Tier 2 entrant (elderberry), because that is where the evidence-to-effort ratio is most favorable for the average patient. Other interventions are discussed on their own topic pages but are not given dedicated benefits deep-dives.
Research Papers: Zinc Lozenges
- Hemila H, Petrus EJ, Fitzgerald JT, Prasad A. Zinc acetate lozenges for treating the common cold: an individual patient data meta-analysis. Br J Clin Pharmacol 2016 — PubMed 27378206
- Hemila H. Zinc lozenges and the common cold: a meta-analysis comparing zinc acetate and zinc gluconate, and the role of zinc dosage. JRSM Open 2017 — PubMed 28515951
- Singh M, Das RR. Zinc for the common cold. Cochrane Database Syst Rev 2013 — Search PubMed
- Prasad AS, Beck FW, Bao B, et al. Duration and severity of symptoms and levels of plasma interleukin-1 receptor antagonist, soluble tumor necrosis factor receptor, and adhesion molecules in patients with common cold treated with zinc acetate. J Infect Dis 2008 — PubMed 18279051
- Eby GA, Davis DR, Halcomb WW. Reduction in duration of common colds by zinc gluconate lozenges in a double-blind study. Antimicrob Agents Chemother 1984 — PubMed 6367635
- Mossad SB, Macknin ML, Medendorp SV, Mason P. Zinc gluconate lozenges for treating the common cold. A randomized, double-blind, placebo-controlled study. Ann Intern Med 1996 — PubMed 8678384
- Novick SG, Godfrey JC, Godfrey NJ, Wilder HR. How does zinc modify the common cold? Clinical observations and implications regarding mechanisms of action. Med Hypotheses 1996 — Search PubMed
- Hulisz D. Efficacy of zinc against common cold viruses: an overview. J Am Pharm Assoc 2004 — Search PubMed
- Wang MX, Win SS, Pang J. Zinc supplementation reduces common cold duration among healthy adults: a systematic review and meta-analysis. Am J Trop Med Hyg 2020 — PubMed 32342851
- Science M, Johnstone J, Roth DE, et al. Zinc for the treatment of the common cold: a systematic review and meta-analysis of randomized controlled trials. CMAJ 2012 — PubMed 22566526
Research Papers: Vitamin D and Respiratory Infection
- Martineau AR, Jolliffe DA, Hooper RL, et al. Vitamin D supplementation to prevent acute respiratory tract infections: systematic review and meta-analysis of individual participant data. BMJ 2017 — PubMed 28202713
- Jolliffe DA, Camargo CA Jr, Sluyter JD, et al. Vitamin D supplementation to prevent acute respiratory infections: a systematic review and meta-analysis of aggregate data from randomised controlled trials. Lancet Diabetes Endocrinol 2021 — PubMed 33798465
- Urashima M, Segawa T, Okazaki M, et al. Randomized trial of vitamin D supplementation to prevent seasonal influenza A in schoolchildren. Am J Clin Nutr 2010 — PubMed 20219962
- Liu PT, Stenger S, Li H, et al. Toll-like receptor triggering of a vitamin D-mediated human antimicrobial response. Science 2006 — PubMed 16497887
- Cannell JJ, Vieth R, Umhau JC, et al. Epidemic influenza and vitamin D. Epidemiol Infect 2006 — Search PubMed
- Bergman P, Lindh AU, Bjorkhem-Bergman L, Lindh JD. Vitamin D and respiratory tract infections: a systematic review and meta-analysis of randomized controlled trials. PLoS One 2013 — Search PubMed
- Charan J, Goyal JP, Saxena D, Yadav P. Vitamin D for prevention of respiratory tract infections: a systematic review and meta-analysis. J Pharmacol Pharmacother 2012 — Search PubMed
- Camargo CA Jr, Ganmaa D, Frazier AL, et al. Randomized trial of vitamin D supplementation and risk of acute respiratory infection in Mongolia. Pediatrics 2012 — Search PubMed
- Ginde AA, Mansbach JM, Camargo CA Jr. Association between serum 25-hydroxyvitamin D level and upper respiratory tract infection in the Third National Health and Nutrition Examination Survey. Arch Intern Med 2009 — PubMed 19237723
- Hewison M. Antibacterial effects of vitamin D. Nat Rev Endocrinol 2011 — Search PubMed
Research Papers: Elderberry and Antiviral Activity
- Zakay-Rones Z, Varsano N, Zlotnik M, et al. Inhibition of several strains of influenza virus in vitro and reduction of symptoms by an elderberry extract (Sambucus nigra L.) during an outbreak of influenza B Panama. J Altern Complement Med 1995 — PubMed 9395631
- Zakay-Rones Z, Thom E, Wollan T, Wadstein J. Randomized study of the efficacy and safety of oral elderberry extract in the treatment of influenza A and B virus infections. J Int Med Res 2004 — PubMed 15080016
- Tiralongo E, Wee SS, Lea RA. Elderberry supplementation reduces cold duration and symptoms in air-travellers: a randomized, double-blind placebo-controlled clinical trial. Nutrients 2016 — PubMed 27023596
- Hawkins J, Baker C, Cherry L, Dunne E. Black elderberry (Sambucus nigra) supplementation effectively treats upper respiratory symptoms: a meta-analysis of randomized, controlled clinical trials. Complement Ther Med 2019 — PubMed 30670267
- Krawitz C, Mraheil MA, Stein M, et al. Inhibitory activity of a standardized elderberry liquid extract against clinically-relevant human respiratory bacterial pathogens and influenza A and B viruses. BMC Complement Altern Med 2011 — PubMed 21352539
- Roschek B Jr, Fink RC, McMichael MD, et al. Elderberry flavonoids bind to and prevent H1N1 infection in vitro. Phytochemistry 2009 — PubMed 19682714
- Mocanu ML, Amariei S. Elderberries-A source of bioactive compounds with antiviral action. Plants (Basel) 2022 — Search PubMed
- Macknin M, Wolski K, Negrey J, Mace S. Effect of elderberry juice on cold and flu-like illness duration and severity in air travelers. J Gen Intern Med 2020 — Search PubMed
- Vlachojannis JE, Cameron M, Chrubasik S. A systematic review on the sambuci fructus effect and efficacy profiles. Phytother Res 2010 — Search PubMed
- Wieland LS, Piechotta V, Feinberg T, et al. Elderberry for prevention and treatment of viral respiratory illnesses: a systematic review. BMC Complement Med Ther 2021 — PubMed 33827515
Research Papers: Steam, Saline, and Mechanical Interventions
- Ramalingam S, Graham C, Dove J, Morrice L, Sheikh A. A pilot, open labelled, randomised controlled trial of hypertonic saline nasal irrigation and gargling for the common cold (ELVIS pilot). Sci Rep 2019 — Search PubMed
- King D, Mitchell B, Williams CP, Spurling GK. Saline nasal irrigation for acute upper respiratory tract infections. Cochrane Database Syst Rev 2015 — PubMed 25892369
- Slapak I, Skoupa J, Strnad P, Hornik P. Efficacy of isotonic nasal wash (seawater) in the treatment and prevention of rhinitis in children. Arch Otolaryngol Head Neck Surg 2008 — Search PubMed
- Singh M, Singh M, Jaiswal N, Chauhan A. Heated, humidified air for the common cold. Cochrane Database Syst Rev 2017 — Search PubMed
- Ramalingam S, Cai B, Wong J, et al. Antiviral innate immune response in non-myeloid cells is augmented by chloride ions via an increase in intracellular hypochlorous acid levels. Sci Rep 2018 — Search PubMed
- Adam P, Stiffman M, Blake RL Jr. A clinical trial of hypertonic saline nasal spray in subjects with the common cold or rhinosinusitis. Arch Fam Med 1998 — Search PubMed
- Rabago D, Zgierska A. Saline nasal irrigation for upper respiratory conditions. Am Fam Physician 2009 — PubMed 19904896
- Tyrrell DA, Barrow I, Arthur J. Local hyperthermia benefits natural and experimental common colds. BMJ 1989 — Search PubMed
- Kassel JC, King D, Spurling GK. Saline nasal irrigation for acute upper respiratory tract infections. Cochrane Database Syst Rev 2010 — Search PubMed
- Yoder JS, Straif-Bourgeois S, Roy SL, et al. Primary amebic meningoencephalitis deaths associated with sinus irrigation using contaminated tap water. Clin Infect Dis 2012 — PubMed 22919000
Research Papers: Cross-Cutting (Cold/Flu Epidemiology, Adjunct Nutrients)
- Heikkinen T, Jarvinen A. The common cold. Lancet 2003 — Search PubMed
- Eccles R. Understanding the symptoms of the common cold and influenza. Lancet Infect Dis 2005 — PubMed 16253889
- Hemila H, Chalker E. Vitamin C for preventing and treating the common cold. Cochrane Database Syst Rev 2013 — Search PubMed
- Karsch-Volk M, Barrett B, Kiefer D, et al. Echinacea for preventing and treating the common cold. Cochrane Database Syst Rev 2014 — Search PubMed
- Lissiman E, Bhasale AL, Cohen M. Garlic for the common cold. Cochrane Database Syst Rev 2014 — Search PubMed
- Maggini S, Pierre A, Calder PC. Immune function and micronutrient requirements change over the life course. Nutrients 2018 — Search PubMed
- Mousa HA. Prevention and treatment of influenza, influenza-like illness, and common cold by herbal, complementary, and natural therapies. J Evid Based Complementary Altern Med 2017 — PubMed 27055821
- Schapowal A, Klein P, Johnston SL. Echinacea reduces the risk of recurrent respiratory tract infections and complications: a meta-analysis of randomized controlled trials. Adv Ther 2015 — PubMed 25784510
- Allan GM, Arroll B. Prevention and treatment of the common cold: making sense of the evidence. CMAJ 2014 — PubMed 24468694
- Hao Q, Dong BR, Wu T. Probiotics for preventing acute upper respiratory tract infections. Cochrane Database Syst Rev 2015 — PubMed 25927096
External Authoritative Resources
- CDC — Seasonal Influenza — vaccination guidance, antiviral recommendations, surveillance data
- CDC — Common Cold (general public information)
- Linus Pauling Institute — Immunity in Depth
- NIH ODS — Zinc Fact Sheet (Health Professionals)
- NIH ODS — Vitamin D Fact Sheet (Health Professionals)
- WHO — Seasonal Influenza Fact Sheet
- PubMed — Common cold treatment randomized trials
Connections
- Cold and Flu Natural Treatments (Main Page)
- Zinc Acetate Lozenges
- Vitamin D Status and Respiratory Infection
- Elderberry and Antiviral Activity
- Steam Inhalation and Saline Rinses
- Zinc
- Vitamin D3
- Vitamin A
- Vitamin C
- Elderberry
- Echinacea
- Andrographis
- Immune Boosting
- All Remedies
- Pulmonology (Respiratory Diseases)