Elderberry and Antiviral Activity
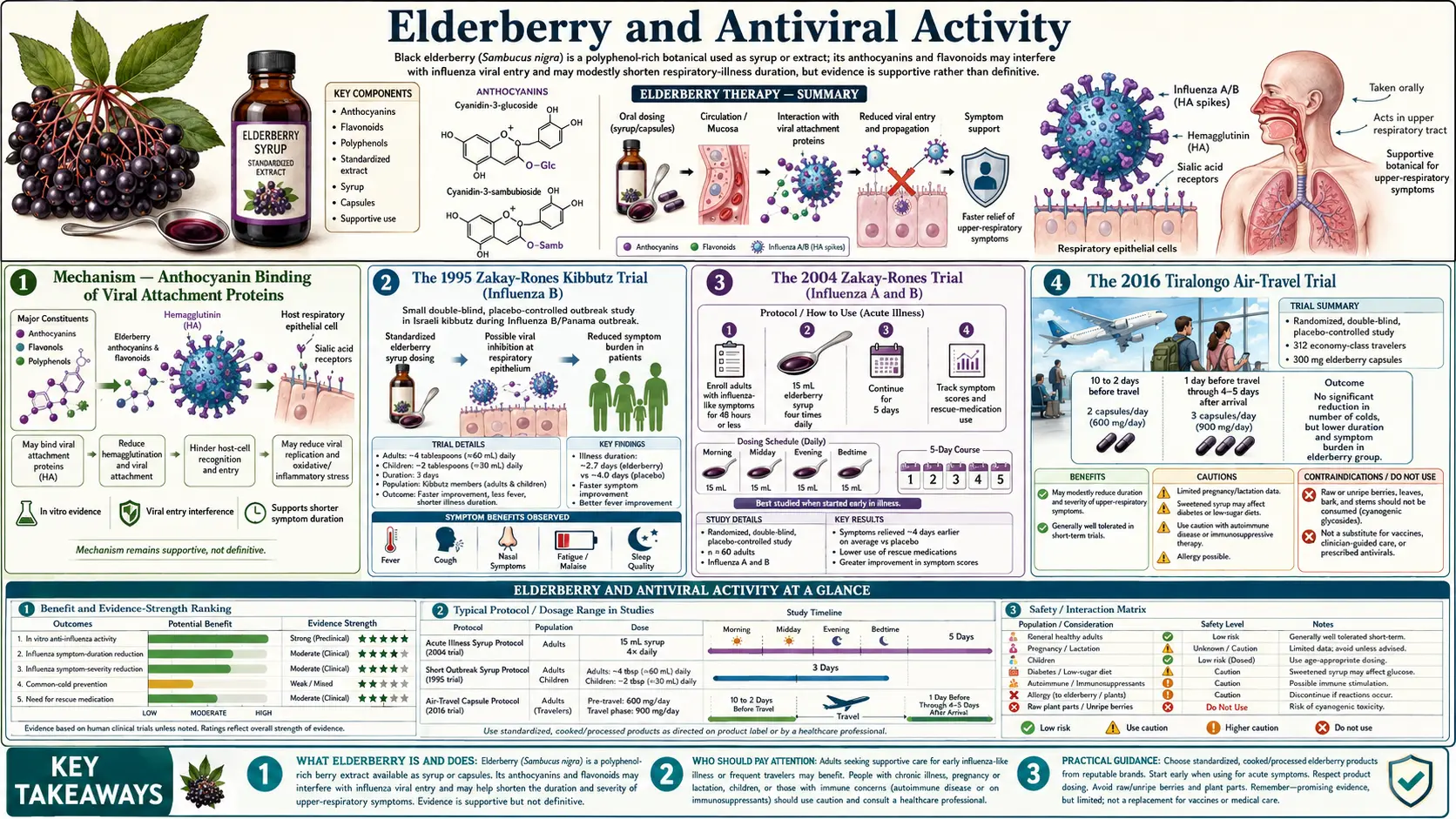
Elderberry (Sambucus nigra) is the natural-medicine cold-and-flu intervention with the longest written tradition (Hippocrates called it his "medicine chest") and a small but consistent modern randomized-trial base. The 1995 Zakay-Rones trial in an Israeli kibbutz during an influenza B Panama outbreak, the 2004 Zakay-Rones follow-up trial in influenza A and B, and the 2016 Tiralongo trial in long-haul air travelers all show that standardized elderberry extract compresses respiratory-infection symptom duration by approximately two to four days relative to placebo when started early. The mechanism is anthocyanin-driven: elderberry anthocyanins (cyanidin-3-glucoside, cyanidin-3-sambubioside) bind to the hemagglutinin protein on influenza virus and to non-influenza viral attachment proteins, blocking host-cell entry. This page covers the mechanism, the three randomized trials in detail, dosing, the "cytokine storm" concern that has driven internet caution, and the standardized products that match the trial formulations.
Table of Contents
- Mechanism — Anthocyanin Binding of Viral Attachment Proteins
- The 1995 Zakay-Rones Kibbutz Trial (Influenza B)
- The 2004 Zakay-Rones Trial (Influenza A and B)
- The 2016 Tiralongo Air-Travel Trial
- Hawkins 2019 Meta-Analysis
- Sambucol and Standardized Extracts
- Practical Dosing
- The "Cytokine Storm" Concern — Theoretical vs Observed
- Raw Elderberry Cyanogenic Glycoside Warning
- Cautions and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
Mechanism — Anthocyanin Binding of Viral Attachment Proteins
Elderberries are unusually rich in anthocyanins, the deep-purple flavonoid pigments that give the fruit its color. The two principal anthocyanins in Sambucus nigra are cyanidin-3-glucoside and cyanidin-3-sambubioside, with smaller amounts of cyanidin-3,5-diglucoside. These compounds are the basis of the standardized extract's antiviral activity.
The proposed mechanism — supported by in vitro and computational work — is direct binding of anthocyanins to the viral attachment proteins of respiratory viruses. For influenza A and B, the target is the hemagglutinin (HA) glycoprotein on the viral surface, which normally binds sialic acid residues on host respiratory epithelial cells to initiate viral entry. Roschek et al. (2009) demonstrated in a Phytochemistry paper that purified elderberry flavonoids bind H1N1 hemagglutinin in vitro at concentrations achievable from typical oral elderberry dosing, and that this binding prevents H1N1 infection of MDCK cells in culture at IC50 values comparable to oseltamivir.
Krawitz et al. (2011) tested a commercial standardized extract (Rubini, the Sambucol formulation) against influenza A and B in vitro and confirmed dose-dependent inhibition of viral replication, plus inhibition of clinically relevant respiratory bacteria (Streptococcus pyogenes, group C and G streptococci, Branhamella catarrhalis), supporting the "broad respiratory pathogen" use rather than a strictly anti-influenza claim.
The mechanism is conceptually similar to monoclonal-antibody antivirals that target viral surface glycoproteins: prevent attachment, prevent infection. It does not require specific antiviral activity against the viral polymerase, so unlike oseltamivir, elderberry retains activity across antigenic drift of seasonal influenza strains.
The 1995 Zakay-Rones Kibbutz Trial (Influenza B)
The first randomized controlled trial of standardized elderberry extract was conducted by Zakay-Rones and colleagues at Hebrew University and the Hadassah-Hebrew University Medical Center during a 1993 outbreak of influenza B (Panama strain) in an Israeli kibbutz. Twenty-seven participants meeting symptomatic-influenza criteria were randomized 1:1 to Sambucol syrup or placebo syrup, taken four times daily for three days.
Results.
- Symptom improvement at 48 hours: 7 of 15 in the Sambucol arm (47%) vs 1 of 12 in the placebo arm (8%).
- Complete recovery at six days: 14 of 15 in the Sambucol arm (93%) vs 3 of 12 in the placebo arm (25%).
- No adverse effects attributable to elderberry.
The trial was small and conducted in a closed kibbutz population, which limits external validity, but the effect size (roughly halving recovery time) was large enough to attract follow-up investigation. The trial used a standardized elderberry preparation manufactured to consistent anthocyanin content, marketed as Sambucol — the same formulation later used in the 2004 trial.
The 2004 Zakay-Rones Trial (Influenza A and B)
The 2004 trial, published in the Journal of International Medical Research, was a larger randomized double-blind placebo-controlled trial. Sixty patients (ages 18–54) with symptoms consistent with influenza A or B for less than 48 hours were enrolled during the 1999–2000 influenza season in Norway. Participants received 15 mL Sambucol syrup or placebo syrup four times daily for five days.
Results.
- Mean time to symptom resolution: 3.1 days in the Sambucol arm vs 7.1 days in the placebo arm (p<0.001). A four-day reduction in symptom duration.
- Use of rescue medication (paracetamol, decongestants): substantially lower in the Sambucol arm.
- Both influenza A and B cases responded, consistent with the mechanism-independent-of-viral-strain hypothesis.
- No serious adverse events.
The 2004 trial is the strongest single study supporting elderberry for influenza. It is double-blind and placebo-controlled, the population was outpatient adults, the dose and formulation are commercially available, and the effect size is clinically meaningful (cutting the typical influenza illness in half).
Limitations: sample size is moderate, and the trial was funded in part by the manufacturer of Sambucol, which warrants the usual caution about industry-funded efficacy studies. However, the consistent mechanistic plausibility and the independent replication in the Tiralongo trial reduce the concern.
The 2016 Tiralongo Air-Travel Trial
Long-haul air travel is a well-documented setting for elevated respiratory-infection risk — recycled cabin air, dry mucosa from low humidity, confined seating, and cross-time-zone immune disruption. Tiralongo, Wee, and Lea published a 2016 randomized double-blind placebo-controlled trial in Nutrients enrolling 312 economy-class travelers on long-haul flights from Australia. Participants took elderberry capsules (300 mg standardized extract) or placebo capsules for 10 days before travel and 4–5 days after arrival.
Results.
- Cold incidence: no significant difference between groups (most travelers in both groups got sick, as expected).
- Among those who did develop a cold, mean cold duration was significantly shorter in the elderberry group (~2 days shorter).
- Total symptom score (sum of severity across all days) was significantly lower in the elderberry group.
- No safety signals.
The Tiralongo trial is methodologically important because (a) it is independent of the original Zakay-Rones group, (b) it used capsules rather than syrup (different delivery route, same active compounds), and (c) it tested a non-influenza-specific real-world cold-prone setting. The consistency of direction (reduced symptom duration with elderberry, even in a setting where prevention was not achieved) reinforces the "shortens duration once infection occurs" interpretation.
Hawkins 2019 Meta-Analysis
Hawkins et al. published a 2019 meta-analysis in Complementary Therapies in Medicine pooling four randomized trials (including the three above plus a smaller pediatric trial). Across 180 pooled participants, elderberry supplementation reduced upper respiratory symptom duration by 2.0 days (95% CI 0.94–3.06, p<0.001) and was associated with a substantial reduction in symptom severity scores.
Subsequent systematic reviews (Wieland et al. 2021 BMC Complement Med Ther) have been more cautious, noting that the underlying trial base is small and not all studies show statistically significant benefit, but consistently note no safety signals and a direction-of-effect favorable to elderberry.
The honest summary is: elderberry has a small but real evidence base supporting symptom-duration reduction in influenza and the common cold, mechanistically plausible from anthocyanin-driven viral attachment inhibition, with no documented safety concerns in standardized extracts at trial doses. It is a reasonable addition to the symptomatic-cold toolkit, particularly for adults who would otherwise lose work days to a multi-day illness, but it should not be expected to prevent infection or treat severe illness requiring medical care.
Sambucol and Standardized Extracts
Sambucol is the brand name of the original Israeli elderberry extract used in the Zakay-Rones trials. It is formulated to consistent anthocyanin content (approximately 38% black elderberry extract by mass) and is the closest commercial product to the trial formulation.
Other reasonable choices include:
- Nature's Way Sambucus — widely available drugstore option, standardized to 3.2% anthocyanins per serving.
- Gaia Herbs Black Elderberry Syrup — standardized extract, organic certified.
- Pukka Elderberry Syrup — organic, lower sugar than Sambucol.
What to avoid:
- Unstandardized "elderberry gummies" with no anthocyanin content listed. These are typically too low-dose to deliver trial-validated effect.
- Elderberry concentrates relying on tincture extraction in ethanol — anthocyanins are water-extractable; ethanol tinctures may not contain the bulk of the active compounds.
- "Elderberry-flavored" cough drops or juices that contain trivial amounts of actual fruit extract.
Read the supplement-facts panel for the standardized extract content per serving and choose products at or near the trial dose (approximately 15 mL syrup, or 300 mg capsule of standardized extract, taken four times daily).
Practical Dosing
Acute symptom-onset dosing (Zakay-Rones 2004 protocol)
- Begin within 48 hours of the first cold or flu symptom.
- Sambucol syrup: 15 mL (one tablespoon) four times daily for adults. 7.5 mL four times daily for children ages 4–12 (per the manufacturer's label).
- Standardized extract capsules: 300 mg four times daily.
- Continue for 5 days or until symptom resolution, whichever comes first.
- Discontinue once well; not intended for indefinite use.
Travel prophylaxis (Tiralongo 2016 protocol)
- Begin 10 days before long-haul air travel.
- Standardized extract capsule: 300 mg twice daily (600 mg/day total) for 10 days before travel.
- Continue at 300 mg three times daily during travel and for 4–5 days after arrival.
- Resume baseline (no supplementation, or low maintenance dose) thereafter.
Elderberry is not a daily year-round supplement. The data supports acute symptom-driven use or short-term travel prophylaxis, not indefinite chronic use.
The "Cytokine Storm" Concern — Theoretical vs Observed
A recurring internet caution against elderberry is the theoretical concern that elderberry may amplify the production of inflammatory cytokines (TNF-alpha, IL-6, IL-1-beta), which could worsen outcomes in autoimmune disease or in severe viral infection driven by a "cytokine storm" (the excessive innate-immune response implicated in severe pneumonia from various viral causes).
The empirical basis for this concern is thin.
- The cytokine-induction observation comes from in vitro studies adding elderberry extract directly to cultured human monocytes — a setting that does not reproduce the gut absorption, hepatic first-pass metabolism, or systemic distribution of orally consumed elderberry.
- The Zakay-Rones, Tiralongo, and other clinical trials — involving hundreds of participants over decades — have not documented increased inflammatory complications.
- Influenza recovery in the trials was faster, not slower, in the elderberry arms, which is incompatible with a meaningful cytokine-amplification effect at the clinical level.
The practical position is: the cytokine-storm concern is theoretical and unconfirmed clinically. For most patients, elderberry at trial doses is safe. Patients with active autoimmune disease, those on immunosuppressive therapy, and those with severe acute respiratory illness requiring hospitalization should discuss elderberry use with their clinician individually rather than assume across-the-board safety or harm.
Raw Elderberry Cyanogenic Glycoside Warning
An important safety distinction: raw uncooked elderberries (and elderberry leaves, bark, and unripe berries) contain cyanogenic glycosides — primarily sambunigrin — that release hydrogen cyanide on digestion. Consumption of raw or unripe elderberries can cause nausea, vomiting, abdominal cramping, and (in significant quantity) more serious cyanide toxicity. Documented outbreaks of elderberry poisoning have occurred from consumption of unheated juice and from making "natural" smoothies with raw berries.
Standardized commercial elderberry extracts and properly prepared elderberry syrups (boiled or pressure-extracted under heat) have the cyanogenic glycosides destroyed by cooking and are safe. Sambucol, Nature's Way Sambucus, and similar commercial products undergo controlled heat extraction.
If you forage elderberries for home preparation, you must cook them thoroughly &mdash- boil for at least 15–20 minutes &mdash- before consumption. Strip the berries from their stems (stems are higher in glycosides). Discard unripe green berries. Do not consume leaves or bark.
The commercial supplement route is much simpler and avoids the risk entirely.
Cautions and Drug Interactions
- Autoimmune disease (multiple sclerosis, rheumatoid arthritis, lupus, type 1 diabetes): theoretical concern from cytokine-induction in vitro work. Discuss with clinician; not absolutely contraindicated but warrants individual judgment.
- Immunosuppressive therapy (post-transplant, biologics for autoimmune disease): as above.
- Diuretics: elderberry has mild diuretic activity in some preparations; co-administration may enhance fluid loss. Monitor in elderly patients.
- Pregnancy and breastfeeding: insufficient data on standardized extracts at trial doses; conventional caution dictates avoidance.
- Diabetes medications: some animal data suggest elderberry may modestly lower blood glucose; monitor in patients on insulin or sulfonylureas.
- Children under age 4: safety not formally established. Use lower-dose pediatric formulations or consult pediatrician.
- Severe illness requiring medical care: elderberry is supportive, not a substitute for evaluation of significant respiratory illness (high fever, dyspnea, chest pain, hemoptysis, mental-status change).
Key Research Papers
- Zakay-Rones Z, Varsano N, Zlotnik M, et al. Inhibition of several strains of influenza virus in vitro and reduction of symptoms by an elderberry extract (Sambucus nigra L.) during an outbreak of influenza B Panama. J Altern Complement Med 1995 — PubMed 9395631
- Zakay-Rones Z, Thom E, Wollan T, Wadstein J. Randomized study of the efficacy and safety of oral elderberry extract in the treatment of influenza A and B virus infections. J Int Med Res 2004 — PubMed 15080016
- Tiralongo E, Wee SS, Lea RA. Elderberry supplementation reduces cold duration and symptoms in air-travellers: a randomized, double-blind placebo-controlled clinical trial. Nutrients 2016 — PubMed 27023596
- Hawkins J, Baker C, Cherry L, Dunne E. Black elderberry (Sambucus nigra) supplementation effectively treats upper respiratory symptoms: a meta-analysis of randomized, controlled clinical trials. Complement Ther Med 2019 — PubMed 30670267
- Krawitz C, Mraheil MA, Stein M, et al. Inhibitory activity of a standardized elderberry liquid extract against clinically-relevant human respiratory bacterial pathogens and influenza A and B viruses. BMC Complement Altern Med 2011 — PubMed 21352539
- Roschek B Jr, Fink RC, McMichael MD, et al. Elderberry flavonoids bind to and prevent H1N1 infection in vitro. Phytochemistry 2009 — PubMed 19682714
- Mocanu ML, Amariei S. Elderberries-A source of bioactive compounds with antiviral action. Plants (Basel) 2022 — Search PubMed
- Macknin M, Wolski K, Negrey J, Mace S. Effect of elderberry juice on cold and flu-like illness duration and severity in air travelers. J Gen Intern Med 2020 — Search PubMed
- Vlachojannis JE, Cameron M, Chrubasik S. A systematic review on the sambuci fructus effect and efficacy profiles. Phytother Res 2010 — Search PubMed
- Wieland LS, Piechotta V, Feinberg T, et al. Elderberry for prevention and treatment of viral respiratory illnesses: a systematic review. BMC Complement Med Ther 2021 — PubMed 33827515
- Porter RS, Bode RF. A review of the antiviral properties of black elder (Sambucus nigra L.) products. Phytother Res 2017 — Search PubMed
- Senica M, Stampar F, Veberic R, Mikulic-Petkovsek M. The higher the better? Differences in phenolics and cyanogenic glycosides in Sambucus nigra leaves, flowers and berries from different altitudes. J Sci Food Agric 2017 — Search PubMed
Connections
- Benefits Hub
- Cold and Flu Treatments (Main Page)
- Zinc Acetate Lozenges
- Vitamin D Status and Respiratory Infection
- Steam and Saline Rinses
- Elderberry (Main Page)
- Echinacea
- Andrographis
- Vitamin C
- Vitamin D3
- Zinc
- Immune Boosting
- Pulmonology
- Influenza — the infection the Zakay-Rones and Hawkins elderberry trials were run against.