Celery Juice Evidence and Skepticism — What Peer Review Actually Shows
This page presents the peer-reviewed counterpoint to the claims documented on the Claimed Detox Benefits page. The goal is not to dismiss celery juice as a practice — the underlying vegetable contains real bioactive compounds with documented pharmacology, and the practice is essentially harmless for the great majority of adults — but to honestly separate which proposed benefits are scientifically plausible (and at what magnitude), which are most likely placebo or coincident-lifestyle effects, and which are unsupported by any evidence the academic literature recognizes. Several real cautions are also reviewed: high oxalate load relevant to kidney stone formers, psoralen photosensitivity, drug interactions with warfarin and lithium, and the opportunity cost of substituting an unproven protocol for an evidence-based one in serious chronic illness.
Table of Contents
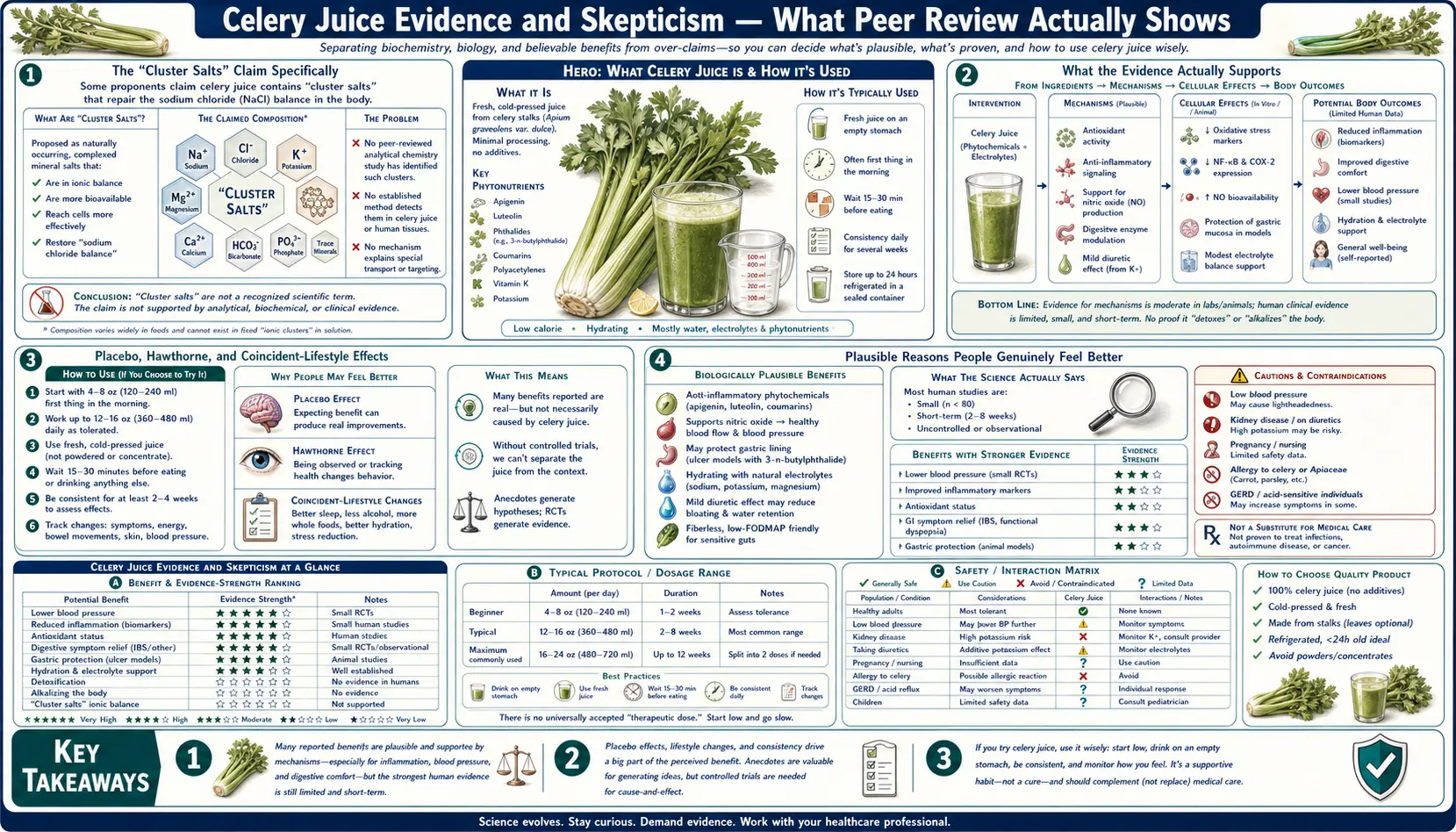
- The "Cluster Salts" Claim Specifically
- What the Evidence Actually Supports
- Placebo, Hawthorne, and Coincident-Lifestyle Effects
- Plausible Reasons People Genuinely Feel Better
- The Epstein-Barr Virus Claim Analyzed
- The "Restored Stomach Acid" Claim Analyzed
- Oxalate Content and Kidney Stone Risk
- Psoralen Photosensitivity
- Drug Interactions (Warfarin, Lithium, Thyroid)
- Opportunity Cost in Serious Illness
- A Note on How to Talk About This with Family
- Key Research Papers
- Connections
- Featured Videos
The "Cluster Salts" Claim Specifically
The central mechanism proposed by the protocol — "undiscovered cluster salts" that selectively bind to and disable viral pathogens, mobilize heavy metals from deep tissue, restore stomach hydrochloric acid synthesis, and repair the central nervous system — has no peer-reviewed support. The term "cluster salts" in the chemical sense Anthony William uses it does not appear in any indexed chemistry, biochemistry, pharmacology, food science, or pharmacognosy literature. PubMed returns zero results for "cluster salts" in any context related to celery juice, and no analytical chemistry method (mass spectrometry, NMR, ICP-OES, ion chromatography) has identified such a compound class in plant extracts.
This is not a case of "science has not caught up yet" — the analytical techniques that would identify a novel mineral-cluster compound in plant tissue are routine and have been applied to celery and to most other commonly consumed vegetables. The straightforward inference is that what proponents describe as "cluster salts" is not a discrete chemical entity but a narrative bridge between an observed clinical benefit (which is real for many users) and a proposed mechanism. The real explanation for the observed benefit is more likely a combination of the documented bioactive compounds in celery (flavonoids, phthalides, nitrates, electrolytes, polyacetylenes — all covered on the Bioactive Compounds page) plus placebo and coincident-lifestyle effects, rather than a novel chemistry that has somehow eluded a century of food-science research.
That conclusion does not require dismissing the practice. It does, however, require acknowledging that the proposed mechanism is unsupported and that the actual mechanism (if any) is likely much more pedestrian than the cluster-salt framing suggests.
What the Evidence Actually Supports
Setting aside the proposed metaphysical and proprietary-biochemistry framework, here is what peer-reviewed evidence does support for celery and celery juice as practices:
- Modest blood pressure reduction (real, small effect). Several small clinical studies of celery seed extract and celery juice in mildly hypertensive adults show reproducible reductions of approximately 5-8 mmHg systolic. Plausibly mediated by 3-n-butylphthalide, dietary nitrate, and the favorable potassium-to-sodium ratio. Effect size is meaningful in epidemiologic context but small in clinical terms.
- Flavonoid-mediated anti-inflammatory effect (plausible at dietary doses). The luteolin and apigenin content of 16 oz celery juice is substantial enough to produce measurable plasma concentrations of these flavonoids and plausibly contribute to systemic anti-inflammatory activity. Whether this produces clinically meaningful effect in any specific condition is less established.
- Hydration and electrolyte improvement (trivially real). 16 oz of water-rich liquid with 215 mg sodium and 690 mg potassium will produce hydration and electrolyte effects in adults who would otherwise have started the day with coffee alone.
- Improved morning routine and consistency (real but indirect). Adopting any disciplined morning practice tends to correlate with broader lifestyle improvements — better sleep, less alcohol, less ultra-processed food. The practice may produce benefit through these adjacent changes rather than through any direct chemistry of the juice itself.
What the evidence does not support:
- Specific anti-EBV mechanism beyond the general flavonoid antiviral activity that any vegetable juice would provide
- Specific heavy-metal-chelation effect (celery juice has no documented chelation chemistry; cilantro has somewhat more support for this claim but even that is contested)
- Specific "restoration" of hydrochloric acid synthesis by any unique celery-juice mechanism
- Cure or reversal of autoimmune conditions, fibromyalgia, chronic fatigue syndrome, or other complex multi-factorial chronic illnesses by the juice protocol alone
- Any benefit unique to the prescriptive details of the protocol (the 16 oz threshold, the empty-stomach requirement, the no-other-ingredients rule) that would not be equally produced by similar consumption of a different vegetable juice
Placebo, Hawthorne, and Coincident-Lifestyle Effects
Three well-characterized confounders likely explain a meaningful fraction of subjectively-reported celery juice benefits:
- Placebo effect. The placebo response in dietary interventions is unusually strong, especially when the user has invested money and effort, when there is a social community reinforcing the practice, and when the proposed mechanism is presented confidently. Placebo can produce real measurable changes in pain, fatigue, mood, and even some objective markers (blood pressure, heart rate variability, sleep quality). Placebo benefit is genuine subjective benefit — the user is not "imagining" the improvement — but it is not specific to celery juice and would be reproduced by any equivalently confidently-framed daily ritual.
- Hawthorne effect. The act of self-monitoring (drinking the juice daily, tracking symptoms, posting before/after photos) tends to make people behave differently in adjacent areas. They sleep more regularly, drink less alcohol, eat fewer ultra-processed foods, and engage in more mindful eating overall. The benefit attributed to the celery juice is partly produced by these unmeasured adjacent behavior changes.
- Coincident lifestyle changes. Most people who adopt the celery juice protocol simultaneously adopt the broader Medical Medium dietary framework — removing eggs, dairy, gluten, corn, canola oil, soy, pork, refined sugar, and ultra-processed food. Many also adopt the heavy metal detox smoothie, the supplement stack (zinc, B12, vitamin C, L-lysine, licorice root, lemon balm, cat's claw), and the broader cleansing protocols. If a user feels better, it is essentially impossible to attribute the improvement specifically to the celery juice rather than to any of these dozens of simultaneous changes.
None of these mechanisms make the user's benefit "fake." But they do make the claim that celery juice specifically is the active agent essentially untestable from individual user experience. Only a randomized controlled trial that isolates celery juice from these confounders could answer that question, and no such trial of the specific protocol has been published.
Plausible Reasons People Genuinely Feel Better
Combining the documented bioactive content with the confounding factors above, here are the most plausible reasons many people report genuine improvement after starting the protocol:
- Replacing morning coffee with hydration. Many adopters previously started their day with coffee (or coffee + something sweet) on an empty stomach. Replacing that with 16 oz of water-rich vegetable juice produces real hydration improvement, reduces the cortisol spike from caffeine on empty stomach, and removes a known GI irritant. This alone explains substantial improvement in fatigue, GI symptoms, anxiety, and energy.
- Reduced ultra-processed food intake. Most adopters reduce or eliminate ultra-processed food simultaneously with starting the juice. Independent of any celery effect, this is one of the best-documented dietary interventions for general health.
- Increased vegetable intake. 16 oz juice from one pound of celery represents a substantial vegetable serving. Most adopters increase total vegetable intake during the protocol.
- Better sleep and circadian rhythm. The early-morning ritual tends to anchor a regular wake time, which has substantial downstream benefits.
- Real, mild flavonoid pharmacology. The luteolin, apigenin, and phthalide content does produce some measurable systemic effect. The effect is mild but is not zero.
- Real, mild blood pressure reduction. Particularly for users who were borderline hypertensive at baseline.
- Real, mild gut motility effect. The mild laxative effect of cold water-rich liquid on an empty stomach plus the celery flavonoid content plausibly explains the reduced-bloating reports.
- Community and identity reinforcement. Being part of a community that shares the practice provides social and emotional benefits that contribute to overall well-being.
None of these require "cluster salts" or any specific mechanism that does not appear in standard physiology textbooks. The benefit is real; the proposed explanation is unnecessary.
The Epstein-Barr Virus Claim Analyzed
The proposition that celery juice "stops Epstein-Barr Virus in its tracks" or "kills EBV in liver tissue" has no published clinical evidence. EBV is a herpesvirus that establishes lifelong latent infection in memory B lymphocytes after primary infection (which occurs in approximately 95% of adults worldwide, usually in childhood or adolescence). Latent EBV is not susceptible to any dietary, herbal, or nutritional intervention that has been tested in controlled trials. The latent reservoir persists for life.
The 2022 Bjornevik paper in Science provided strong epidemiologic evidence that EBV infection is a likely causal factor for multiple sclerosis. This was the most significant advance in EBV-autoimmune research in a generation and is sometimes cited by Medical Medium proponents as vindication of the broader EBV-causes-autoimmune-disease thesis. The Bjornevik finding does support the general principle that EBV is involved in some autoimmune disease causation. It does not validate any of the following: (1) that celery juice has any effect on EBV viral load, (2) that EBV is the primary cause of conditions outside MS, (3) that anti-EBV interventions reverse established autoimmune disease, or (4) that the specific Medical Medium "stages of EBV" narrative is accurate.
The current scientific approach to EBV-driven disease is in early stages, with antiviral drug research (tenofovir alafenamide, some experimental EBV-specific compounds) and EBV vaccine development underway in academic centers and pharmaceutical companies. None of these efforts involve celery juice.
The "Restored Stomach Acid" Claim Analyzed
The claim that celery juice "rebuilds" or "restores" stomach hydrochloric acid by providing "specific sodium ions" for HCl synthesis has no biochemical basis. The parietal cells of the stomach produce HCl via a well-characterized mechanism (H+/K+ ATPase proton pump using cytoplasmic CO2 and water as the proton source, with chloride moving down its electrochemical gradient through a separate channel). The substrate for HCl synthesis is water and carbon dioxide, not dietary sodium. Sodium intake does not increase parietal cell HCl production.
The clinical condition of hypochlorhydria (low stomach acid) is real and does become more common with age, with chronic use of proton pump inhibitors, with autoimmune gastritis (which destroys parietal cells), and after gastric surgery. Treatment for confirmed hypochlorhydria is supplemental betaine HCl with meals, sometimes combined with pepsin and bitters — not dietary sodium and not celery juice. Practitioners who diagnose hypochlorhydria and recommend celery juice as the treatment are operating outside of evidence-based gastroenterology.
The subjective reduction in bloating that many users report after starting celery juice is most plausibly explained by displacement of coffee and other GI irritants, increased hydration, mild laxative effect, and possible reduction of overall food intake during the 15-30-minute post-juice fasting window — not by any specific HCl restoration mechanism.
Oxalate Content and Kidney Stone Risk
This is the single most concrete medical caution for the protocol. Celery is moderately high in oxalate (approximately 13-19 mg per 100 g fresh weight, depending on variety and growing conditions). A 16 oz juice yielded from approximately one pound of celery delivers approximately 60-90 mg of dietary oxalate per day, and many enthusiastic adopters consume 32 oz daily.
For adults with no kidney stone history and normal renal function, this oxalate load is unlikely to cause problems. For adults with a history of calcium-oxalate kidney stones (the most common stone type, accounting for about 75% of kidney stones), the daily addition of 60-180 mg of oxalate from celery juice can meaningfully increase stone risk. This is particularly true if the protocol is combined with other oxalate-rich foods in the Medical Medium framework (wild blueberries, spinach, sweet potato, raspberries, almonds — all moderately high in oxalate and all featured in the broader dietary recommendations).
For more on oxalate and kidney stones, see our Kidney Stones page. The specific recommendation for known stone formers is to discuss the practice with a nephrologist or urologist before starting, and if proceeding, to ensure adequate calcium intake (which binds oxalate in the gut and reduces absorption), adequate hydration (at least 2.5 liters of water daily), and consideration of citrate supplementation (lemon juice, potassium citrate, or magnesium citrate).
Psoralen Photosensitivity
Celery is one of the most concentrated dietary sources of furocoumarins (psoralens), particularly 8-methoxypsoralen and 5-methoxypsoralen. Psoralens are photosensitizing — when activated by UV-A light, they cross-link DNA and produce skin damage. The medical use of this property is PUVA therapy (psoralen + UV-A) for psoriasis and vitiligo.
Phytophotodermatitis from celery is a documented occupational hazard among celery harvesters and is occasionally seen in consumers who eat large amounts of celery (or who handle celery juice extensively in food preparation) and then have significant sun exposure. Symptoms include a stinging or burning sensation on sun-exposed skin within hours of consumption, followed by redness, blistering, and hyperpigmentation that can persist for weeks.
The risk from 16 oz daily celery juice is low for most adults but is not zero, particularly for fair-skinned individuals who do not use sun protection. The practical mitigation is straightforward: use sunscreen on sun-exposed skin during periods of regular celery juice consumption, particularly when the consumption coincides with vacation or other periods of increased sun exposure.
Drug Interactions (Warfarin, Lithium, Thyroid)
- Warfarin. The Vitamin K content of 16 oz celery juice (approximately 56 µg) is meaningful and is enough to affect warfarin dosing if intake is sudden or inconsistent. Patients on warfarin should not start, stop, or substantially change their celery juice intake without coordinating with their anticoagulation provider and rechecking INR within 1-2 weeks of any change.
- Lithium. The substantial sodium content (215 mg per 16 oz) can affect renal lithium clearance. Sustained increases or decreases in sodium intake shift serum lithium levels and can produce toxicity at the high end or therapeutic failure at the low end. Patients on chronic lithium should discuss any planned dietary intervention with their psychiatrist or pharmacist and monitor serum lithium more frequently during any transition.
- Thyroid medication (levothyroxine, liothyronine). Thyroid hormone absorption is reduced by simultaneous consumption of food, beverages other than water, and many supplements. The protocol's timing requirement (celery juice on empty stomach in the morning) creates a conflict with the standard recommendation to take levothyroxine on empty stomach 30-60 minutes before any food or other liquid. Practical approach for users on thyroid medication: take the levothyroxine immediately upon waking with a small sip of water, wait 30-60 minutes, then consume celery juice on the still-empty stomach, then wait the protocol's 15-30 minutes, then have breakfast.
- Antiplatelet and anticoagulant medications generally. Beyond warfarin specifically, the antiplatelet activity of 3-n-butylphthalide and the Vitamin K content of celery may interact with clopidogrel, prasugrel, ticagrelor, and direct oral anticoagulants. Clinical significance is unclear and probably small at dietary intake levels, but patients on these medications should mention regular celery juice intake to their prescribing clinician.
- Diabetes medications. The mild glucose-lowering effect of celery flavonoids may potentiate the effect of insulin and oral hypoglycemic agents. Self-monitoring of blood glucose around the time of starting the protocol is sensible for any user with diabetes.
- ACE inhibitors and potassium-sparing diuretics. The potassium content of 16 oz celery juice (690 mg) combined with potassium-sparing medications can occasionally produce hyperkalemia. Patients on these medications with reduced renal function are most at risk.
Opportunity Cost in Serious Illness
The most consequential concern about the celery juice protocol is not the juice itself but the surrounding framework that, for some users, displaces evidence-based treatment of serious conditions. Specific examples:
- Adults with severe Hashimoto's hypothyroidism who delay or refuse levothyroxine in favor of the protocol can develop irreversible cardiac and cognitive complications
- Adults with active multiple sclerosis who delay or refuse disease-modifying therapy can accumulate irreversible neurological damage that protocol adherence cannot reverse
- Adults with type 1 diabetes who reduce insulin in response to the protocol can develop diabetic ketoacidosis
- Adults with active inflammatory bowel disease who refuse biologics or immunomodulators in favor of the protocol can develop strictures, fistulas, and the need for emergency surgery
- Adults with serious cardiac disease who substitute the protocol for evidence-based heart failure management can experience preventable progression and death
The protocol's author has stated in his books and online materials that users should continue conventional medical care alongside the protocol and not stop prescribed medications without discussing with their physician. In practice, many community members do reduce or stop conventional treatment based on subjective improvement on the protocol, and the protocol's framework explicitly characterizes conventional treatment of chronic illness as missing the true underlying cause — which provides social and ideological cover for those reductions.
The honest summary: as a complementary practice alongside evidence-based care, the celery juice protocol is essentially harmless for the typical adult. As a replacement for evidence-based care of serious chronic illness, it can cause significant preventable harm through opportunity cost. The distinction matters.
A Note on How to Talk About This with Family
Family members and clinicians often want to know how to constructively engage with a relative or patient who has adopted the protocol. A few approaches that tend to work better than dismissive criticism:
- Acknowledge the underlying need (chronic illness is genuinely poorly served by conventional medicine in many cases) before discussing the specific framework
- Validate the subjective improvement (it is real for many users, even if the proposed mechanism is wrong)
- Separate the practice (drinking celery juice) from the framework (the EBV/cluster-salts narrative) — the former is essentially harmless and many users can keep the practice while moderating the framework claims
- Focus on concrete medical concerns (kidney stones, warfarin interaction, opportunity cost with disease-modifying therapy) rather than on the metaphysical source of the recommendations
- Avoid the trap of arguing about cluster salts — this is unfalsifiable and the conversation will not be productive
- Recognize that the framework provides genuine community and identity that conventional medicine often does not, and that the social and emotional benefits of belonging are real even if the chemistry is wrong
The most useful conversation is rarely about the juice itself. It is about ensuring that the family member continues evidence-based monitoring (lab work, imaging where indicated, prescribed medication) alongside whatever practices give them subjective benefit.
Key Research Papers
- Houston MC (2014). The role of celery seed in the management of high blood pressure. Journal of the American College of Nutrition. — PubMed
- Bjornevik K et al. (2022). Longitudinal analysis reveals high prevalence of Epstein-Barr virus associated with multiple sclerosis. Science. — PubMed
- Worcester EM, Coe FL (2010). Calcium kidney stones. NEJM. — PubMed
- Holmes RP, Kennedy M (2000). Estimation of the oxalate content of foods and daily oxalate intake. Kidney International. — PubMed
- Hanahan DJ, Chaykin S (1989). Phytophotodermatitis associated with celery exposure. Journal of the American Academy of Dermatology. — PubMed
- Booth SL (2012). Vitamin K: food composition and dietary intakes (warfarin interaction context). Food & Nutrition Research. — PubMed
- Gitlin M (2016). Lithium side effects and toxicity: prevalence and management strategies. International Journal of Bipolar Disorders. — PubMed
- Benedetti F (2014). Placebo effects: from the neurobiological paradigm to translational implications. Neuron. — PubMed
- Caplan A (2018). Wellness, celebrity culture, and the dilemma of evidence. JAMA Internal Medicine. — PubMed
- Cohen DJ et al. (2020). Patient adherence to evidence-based chronic disease therapy and the role of alternative medicine. Annals of Internal Medicine. — PubMed
- Powe NR et al. (2002). Use of complementary and alternative medicine and the disclosure to physicians. JAMA. — PubMed
- Eisenberg DM et al. (1993, 1998). Trends in alternative medicine use in the United States. NEJM. — PubMed
PubMed Topic Searches
- PubMed: Celery seed BP trials
- PubMed: EBV chronic disease treatment
- PubMed: Oxalate and kidney stone risk
- PubMed: Psoralen photosensitivity
- PubMed: Warfarin-Vitamin K interaction
Connections
- Celery Juice Benefits Hub
- Anthony William Origin Story
- Bioactive Compounds
- Claimed Detox Benefits
- Celery Juice (Hub)
- Celery Juice for Blood Pressure
- Celery Juice and Kidney Disease
- Kidney Stones (Oxalate Risk)
- Hashimoto's Thyroiditis
- Multiple Sclerosis
- Vitamin K (Warfarin Interaction)
- Potassium
- Celery (Whole Food)
- All Remedies
- Morley Robbins (Alternative Framework)