Vanadium: Trace Mineral, Insulin Mimetic, and Supplement Hype
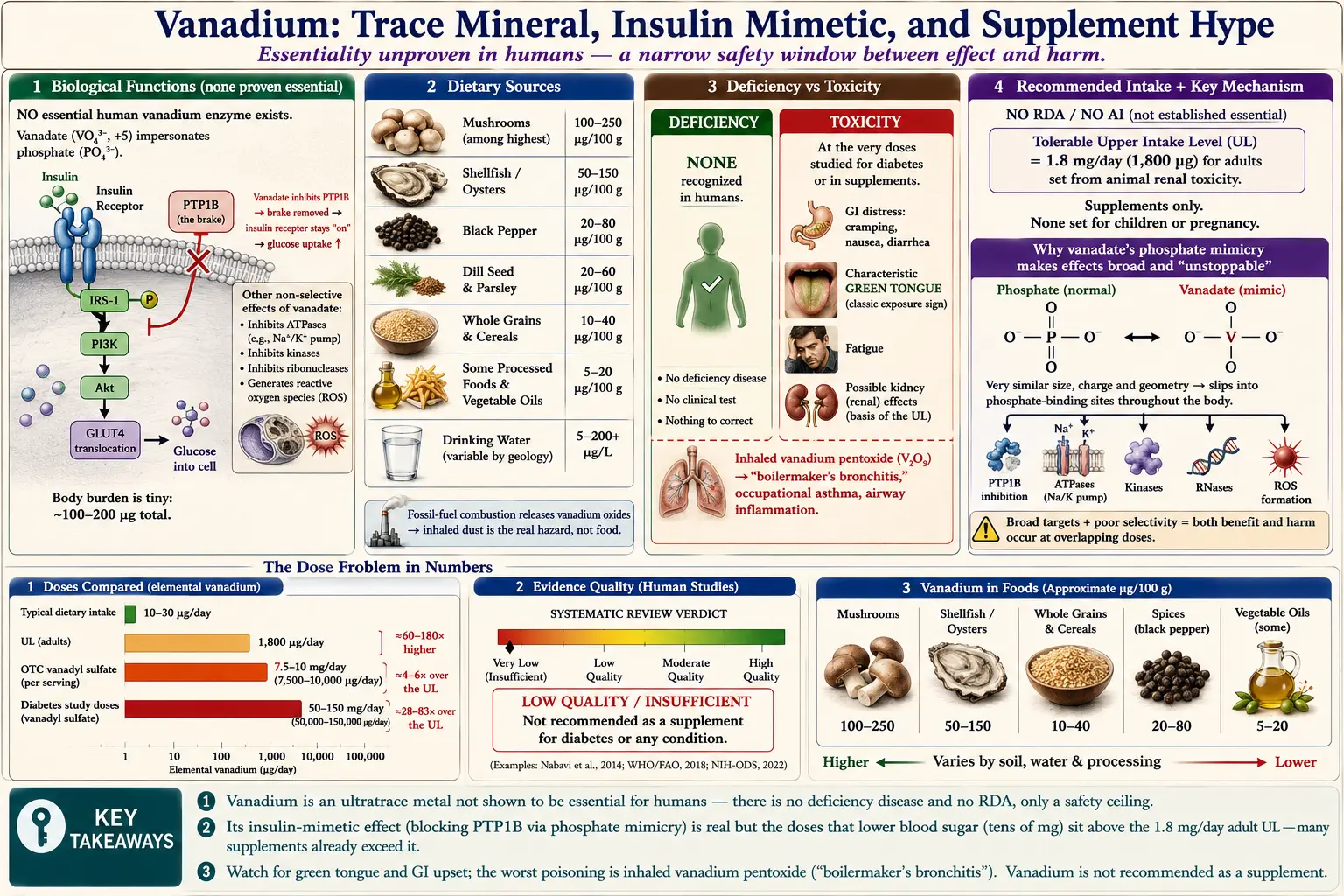
Table of Contents
- Overview
- Biological Functions
- Dietary Sources
- Deficiency
- Recommended Intake
- Supplementation & Forms
- Toxicity & Upper Limit
- Special Considerations
- Key Research Papers
- Connections
- Featured Videos
1. Overview
Vanadium is a silvery-gray transition metal (chemical symbol V, atomic number 23) named after Vanadis, an Old Norse name for the goddess Freyja, because its compounds form a striking range of colors. In the body it is an ultratrace element: a typical adult carries only on the order of 100–200 micrograms (µg) of vanadium total — a few millionths of a gram — far less than the grams of calcium or the hundreds of milligrams of magnesium we hold. Most people take in roughly 10–30 µg per day from ordinary food and water, and the body absorbs only a small fraction of that.
Here is the honest headline that frames everything below: vanadium has not been shown to be an essential nutrient for humans. A nutrient is called "essential" only when removing it from the diet produces a reproducible deficiency disease that the nutrient then cures. That experiment has been done for iron, zinc, and iodine — but not, convincingly, for vanadium. Vanadium is required by certain bacteria, marine algae, and some lower animals (for example, sea squirts concentrate it to remarkable levels, and some nitrogen-fixing bacteria use a vanadium-based enzyme). In a few experimental animals, diets extremely low in vanadium produced subtle effects, but the findings have been inconsistent and have never established a clear human requirement. The U.S. National Academies, in setting Dietary Reference Intakes for trace elements, concluded that there was no basis for an essential role of vanadium in humans and therefore set no recommended intake.
So why does vanadium have a reputation at all? Almost entirely because of one pharmacological property, discovered over a century ago and intensively studied since the 1980s: certain vanadium compounds mimic insulin and lower blood sugar in animals and in small human studies. That single observation launched decades of chemistry aimed at turning vanadium into a diabetes drug, and — separately — a wave of 1990s bodybuilding marketing for "vanadyl sulfate." This page separates the real, peer-reviewed biology from the supplement-aisle hype, and is candid where the evidence is weak or the risks outweigh the promise.
Why this page treats vanadium cautiously
Two facts recur throughout and are worth stating up front. First, the doses of vanadium that move blood sugar in people are close to the doses that cause harm — a problem chemists call a "narrow therapeutic window." Second, vanadium’s biological tricks come from the way one of its forms imitates phosphate, a chemistry that does not switch itself off neatly inside cells. Both points mean that "a little might help" does not safely scale to "more is better."
2. Biological Functions
Unlike iron (which carries oxygen) or zinc (which is built into hundreds of human enzymes), no essential vanadium-dependent enzyme has been identified in humans. Whatever vanadium does in our cells, it does as a chemical interloper rather than as a designed-in cofactor. To understand its effects you have to understand its chemistry.
Vanadate looks like phosphate
In water and in body fluids, vanadium exists mainly in two forms relevant to biology: vanadyl (the +4 oxidation state, written VO2+) and vanadate (the +5 state, written VO43−). The vanadate ion has almost the same size, shape, and charge distribution as the everyday phosphate ion (PO43−). Because so much of cellular machinery is built to grab, move, and release phosphate — ATP energy transfer, signaling switches, ion pumps — vanadate can slip into those phosphate-shaped pockets and interfere. This single structural resemblance is the root of nearly all of vanadium’s biological and toxic effects.
The insulin-mimetic mechanism: inhibiting PTP1B
Insulin works by docking onto the insulin receptor on a cell’s surface, which switches the receptor "on" by attaching phosphate groups to tyrosine amino acids (a process called tyrosine phosphorylation). Cells turn that signal off using enzymes called protein tyrosine phosphatases — molecular erasers that remove those phosphate marks. The best-studied of these is protein tyrosine phosphatase 1B (PTP1B), a brake on insulin signaling.
Vanadate, because it impersonates the phosphate that these enzymes act on, jams the eraser. Laboratory work has shown that vanadate forms a tight, transition-state-like complex in the active site of tyrosine phosphatases, blocking them; the even more potent oxidized species "pervanadate" does so essentially irreversibly. With the brake disabled, the insulin receptor and its downstream signals stay switched on longer, so glucose is pushed into cells and out of the blood. Crucially, vanadium does this downstream of insulin and partly independent of it — in animal experiments it can lower glucose even when insulin is scarce, which is what earned it the label "insulin-mimetic" (imitating insulin) rather than merely "insulin-sensitizing."
Other phosphate-related effects
The same phosphate mimicry lets vanadate inhibit a long list of other enzymes in the test tube — ATPases (including the sodium-potassium pump that maintains cell voltage), ribonucleases, and various phosphatases and kinases. These broad, non-selective actions are exactly why vanadium is a poor candidate for a clean drug: a molecule that interferes with phosphate handling in general will inevitably touch many processes besides blood-sugar control, which is one source of its side effects. Vanadium compounds also generate reactive oxygen species and can promote oxidative stress at higher exposures, contributing to toxicity rather than benefit.
3. Dietary Sources
Vanadium is widespread in the food supply at very low concentrations, so most people get their small daily intake from a broad mix of ordinary foods rather than from any single rich source. Total intake estimates for adults generally fall in the range of about 10–30 µg per day, though figures vary widely between surveys and regions because soil and water content differ and because measuring such tiny amounts accurately is difficult.
Foods that contribute the most
- Mushrooms — among the higher-vanadium foods.
- Shellfish — oysters and other shellfish concentrate trace metals from seawater.
- Black pepper, dill seed, and parsley — certain spices and herbs are surprisingly vanadium-dense by weight, though the amounts actually eaten are small.
- Whole grains and cereal products — modest per-serving amounts, but large contributors to total intake because they are eaten in quantity.
- Some prepared and processed foods, fats, and vegetable oils — can carry measurable vanadium.
Drinking water and the environment
Drinking water can add a variable amount depending on local geology; in most municipal supplies the contribution is small, but some groundwater near volcanic or mineral-rich rock contains more. Vanadium also enters the wider environment through the burning of fossil fuels — heavy crude oils and residual fuel oils are relatively rich in vanadium, and combustion releases vanadium oxides into air. This is the bridge to the occupational concern discussed in the Toxicity section: people are far more likely to encounter a hazardous dose of vanadium by inhaling industrial dust or fume than by eating food.
For practical purposes, a varied diet supplies vanadium automatically and effortlessly. There is no recognized reason to seek out high-vanadium foods, and no dietary deficiency to guard against.
4. Deficiency
There is no recognized vanadium-deficiency disease in humans: no symptoms, lab finding, or condition has been reliably linked to low dietary vanadium, and no essential function has been proven. The practical takeaway is that you do not need to worry about getting "enough" vanadium. For a full, patient-friendly guide to what low-vanadium claims really mean, see Vanadium Deficiency: What the Evidence Shows and, for the far more relevant question of getting too much, Vanadium Toxicity: What the Evidence Shows.
5. Recommended Intake
Because vanadium has not been established as essential, there is no Recommended Dietary Allowance (RDA) and no Adequate Intake (AI) for vanadium at any age, for either sex, or during pregnancy and lactation. The U.S. National Academies (formerly the Institute of Medicine), in the Dietary Reference Intakes report covering trace elements, explicitly declined to set a required intake because the data did not support an essential role in humans.
What the National Academies did set
The only reference value the National Academies established for vanadium is a Tolerable Upper Intake Level (UL) — a ceiling for safety, not a target to reach. For adults aged 19 and older, the UL is 1.8 milligrams of elemental vanadium per day (1.8 mg = 1,800 µg), and it was derived from supplemental vanadium, not from food (see the Toxicity section). No UL was set for children, adolescents, or pregnant and lactating women, mainly because of a lack of data — which is itself a reason for those groups to avoid vanadium supplements entirely.
It is worth appreciating the scale here. The UL of 1,800 µg/day is a safety ceiling for supplements, yet it sits roughly 60–180 times higher than typical dietary intake of 10–30 µg/day. Ordinary eating comes nowhere near the ceiling; only deliberate supplementation can approach or exceed it. In short, there is nothing to "hit" with vanadium — only something to stay below.
6. Supplementation & Forms
Despite the absence of any requirement, vanadium is sold as a dietary supplement, usually marketed for blood-sugar support or, historically, for muscle building. The most common form is vanadyl sulfate (VOSO4); sodium metavanadate (NaVO3) and sodium orthovanadate have been used in research. Chemists have also designed more sophisticated organic complexes — most famously bis(maltolato)oxovanadium(IV), abbreviated BMOV — to make vanadium better absorbed, less irritating to the gut, and active at lower doses. BMOV and its relatives reached early-phase pharmaceutical development but none became an approved medicine.
How much is in a supplement — and how that compares to study doses
Consumer vanadyl sulfate products commonly provide on the order of 7.5 to 10 mg or more of elemental vanadium per daily dose. Read that against the previous section: the adult safety ceiling (UL) is 1.8 mg/day. Many over-the-counter vanadium products therefore deliver several times the upper limit in a single recommended serving — an unusual and alarming situation for a supplement. The human diabetes studies that reported glucose-lowering used even larger amounts, frequently in the range of roughly 50 to 150 mg of vanadyl sulfate per day (tens of milligrams of elemental vanadium), for several weeks. In other words, the doses that did something to blood sugar were squarely in territory the National Academies considers unsafe, and side effects (especially gastrointestinal) were common at those doses.
Honest summary of the evidence
The human trials of vanadyl sulfate in type 2 diabetes were small (typically a handful to a few dozen participants), short, and mostly without proper placebo controls or blinding. Some reported modest improvements in fasting glucose and insulin sensitivity; others were unimpressive. A formal systematic review of vanadium oral supplements for glycemic control in type 2 diabetes concluded that the evidence was of low quality and insufficient to recommend vanadium, and called for properly designed trials — which, decades on, have not materialized, precisely because the safe-dose problem makes them hard to justify. For these reasons, vanadium is not recommended for routine supplementation, and it has never been approved as a treatment for diabetes anywhere.
If a clinician and patient ever consider vanadium experimentally, it should be at the lowest dose, for a limited time, with monitoring — not self-prescribed from a bottle promising "natural blood-sugar support."
7. Toxicity & Upper Limit
Toxicity is the decisive practical issue with vanadium, because harm arrives at doses uncomfortably close to those claimed to help. The U.S. Tolerable Upper Intake Level for adults is 1.8 mg/day of elemental vanadium (from supplements, based on kidney effects in animals), yet many products exceed it; swallowing too much causes gastrointestinal distress, a characteristic green tongue, and possible kidney effects, while the most serious poisoning is occupational — inhaling vanadium pentoxide dust or fume ("boilermaker’s bronchitis"). For the full, patient-friendly guide to symptoms, the upper limit, and the occupational hazard, see Vanadium Toxicity: What the Evidence Shows; for the opposite (and largely theoretical) question of too little, see Vanadium Deficiency: What the Evidence Shows.
8. Special Considerations
This section gives the plain, honest bottom line, because vanadium is a topic where marketing has outrun the science.
For people with diabetes or prediabetes
It is understandable to be drawn to a "natural" compound that lowers blood sugar. But the gap between an apparently effective vanadium dose and a toxic one is small, the supporting human trials are weak and unblinded, no health authority endorses it, and many products on the shelf already exceed the official safety ceiling. Vanadium should not be used in place of proven diabetes care — lifestyle measures and medications such as metformin and other established drugs have strong, large-trial evidence for both blood-sugar control and long-term outcomes, which vanadium entirely lacks. Anyone managing diabetes who is curious about vanadium should raise it with their clinician rather than self-treat, especially because vanadium could in theory add to the blood-sugar-lowering effect of insulin or other medications and contribute to low blood sugar (hypoglycemia).
The bodybuilding and "ergogenic" claims
In the 1990s, vanadyl sulfate was marketed aggressively to athletes and bodybuilders on the logic that, because insulin drives nutrients and glycogen into muscle, an "insulin-like" mineral should build muscle and boost performance. Controlled studies do not support this. A randomized trial of oral vanadyl sulfate in weight-training participants found no meaningful benefit to body composition, and any apparent strength gains were attributable to training itself rather than the supplement. In healthy people with normal insulin function, there is no good reason to expect vanadium to improve muscle, strength, or athletic performance — and real reason to avoid the gastrointestinal side effects and the safety-ceiling problem.
Who should be especially cautious
- Pregnant and breastfeeding women, infants, children, and adolescents — no safe supplemental dose has been established; avoid vanadium supplements.
- People with kidney disease — because the upper limit is based on kidney toxicity, impaired kidneys are a particular concern.
- People taking diabetes medications or insulin — potential additive glucose-lowering.
- Workers in oil-fired boiler cleaning, metallurgy, or catalyst manufacture — the real-world vanadium risk for most people is occupational inhalation; follow workplace exposure controls.
The honest recommendation
For the general public, the sensible position on vanadium is simple: a varied diet already supplies the trace amounts present in food, no deficiency exists to correct, and vanadium is not recommended as a routine supplement. Its one genuinely interesting property — mimicking insulin — is also the source of its danger, because the helpful and harmful doses overlap. Vanadium is a fascinating case study in how a real laboratory mechanism can be inflated into supplement-aisle promises that the evidence does not support. Anyone still considering it should do so only in consultation with a clinician.
9. Key Research Papers
- Cohen N, Halberstam M, Shlimovich P, et al. Oral vanadyl sulfate improves hepatic and peripheral insulin sensitivity in patients with non-insulin-dependent diabetes mellitus. Journal of Clinical Investigation. 1995;95(6):2501–2509. doi:10.1172/jci117951
- Halberstam M, Cohen N, Shlimovich P, Rossetti L, Shamoon H. Oral vanadyl sulfate improves insulin sensitivity in NIDDM but not in obese nondiabetic subjects. Diabetes. 1996;45(5):659–666. doi:10.2337/diabetes.45.5.659
- Boden G, Chen X, Ruiz J, van Rossum GD, Turco S. Effects of vanadyl sulfate on carbohydrate and lipid metabolism in patients with non-insulin-dependent diabetes mellitus. Metabolism. 1996;45(9):1130–1135. doi:10.1016/s0026-0495(96)90013-x
- Goldfine AB, Patti ME, Zuberi L, et al. Metabolic effects of vanadyl sulfate in humans with non-insulin-dependent diabetes mellitus: in vivo and in vitro studies. Metabolism. 2000;49(3):400–410. doi:10.1016/s0026-0495(00)90418-9
- Cusi K, Cukier S, DeFronzo RA, Torres M, Puchulu FM, Redondo JCP. Vanadyl sulfate improves hepatic and muscle insulin sensitivity in type 2 diabetes. Journal of Clinical Endocrinology & Metabolism. 2001;86(3):1410–1417. doi:10.1210/jcem.86.3.7337
- Smith DM, Pickering RM, Lewith GT. A systematic review of vanadium oral supplements for glycaemic control in type 2 diabetes mellitus. QJM: An International Journal of Medicine. 2008;101(5):351–358. doi:10.1093/qjmed/hcn003
- Thompson KH, McNeill JH, Orvig C. Vanadium compounds as insulin mimics. Chemical Reviews. 1999;99(9):2561–2572. doi:10.1021/cr980427c
- Thompson KH, Orvig C. Design of vanadium compounds as insulin enhancing agents. Journal of the Chemical Society, Dalton Transactions. 2000;(17):2885–2892. doi:10.1039/b002753g
- Huyer G, Liu S, Kelly J, et al. Mechanism of inhibition of protein-tyrosine phosphatases by vanadate and pervanadate. Journal of Biological Chemistry. 1997;272(2):843–851. doi:10.1074/jbc.272.2.843
- Fawcett JP, Farquhar SJ, Walker RJ, Thou T, Lowe G, Goulding A. The effect of oral vanadyl sulfate on body composition and performance in weight-training athletes. International Journal of Sport Nutrition. 1996;6(4):382–390. doi:10.1123/ijsn.6.4.382
- Sakurai H. Vanadium distribution in rats and DNA cleavage by vanadyl complex: implication for vanadium toxicity and biological effects. Environmental Health Perspectives. 1994;102(suppl 3):35–36. doi:10.1289/ehp.94102s335
- Levy BS, Hoffman L, Gottsegen S. Boilermakers’ bronchitis: respiratory tract irritation associated with vanadium pentoxide exposure during oil-burning furnace cleaning. Journal of Occupational Medicine. 1984;26(8):567–570. doi:10.1097/00043764-198408000-00009
- National Institutes of Health, Office of Dietary Supplements. Vanadium — Health Professional Fact Sheet. ods.od.nih.gov/factsheets/Vanadium-HealthProfessional
- Institute of Medicine (now National Academies of Sciences, Engineering, and Medicine). Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc (Vanadium chapter; UL 1.8 mg/day for adults). National Academies Press, 2001. nap.nationalacademies.org/catalog/10026
- Agency for Toxic Substances and Disease Registry (ATSDR). Toxicological Profile for Vanadium. U.S. Department of Health and Human Services. atsdr.cdc.gov/toxprofiles/tp58.pdf
- National Institute for Occupational Safety and Health (NIOSH). Vanadium dust and Vanadium pentoxide — NIOSH Pocket Guide to Chemical Hazards. cdc.gov/niosh/npg (vanadium pentoxide)
Connections
- All Minerals
- Vanadium Deficiency: What the Evidence Shows
- Vanadium Toxicity: What the Evidence Shows
- Chromium — the other "blood-sugar" trace mineral
- Magnesium — an essential mineral tied to insulin sensitivity
- Zinc — essential trace mineral, insulin storage and signaling
- Selenium — essential trace mineral with a narrow safe range
- Boron — another ultratrace element of uncertain essentiality
- Toxic Minerals — metals where the risk outweighs any benefit
- Hexavalent Chromium — a toxic, oxidized metal form
- Heavy Metals — exposure, toxicity, and testing
- Diabetes — the condition vanadium has been studied to treat
- Lab Tests — how trace metals and blood sugar are measured