Hexavalent Chromium (Chromium-6) Toxicity: The Erin Brockovich Carcinogen
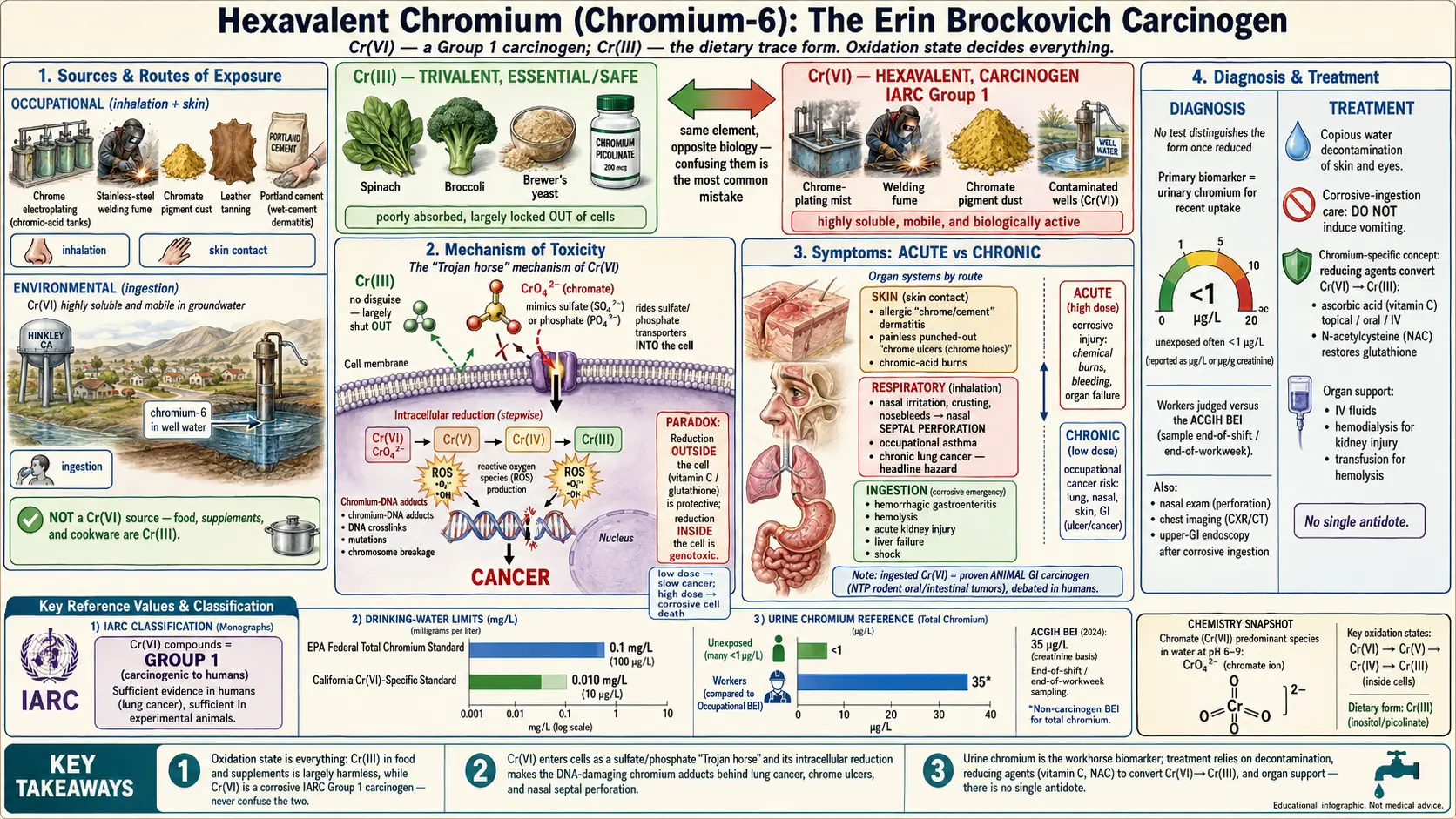
Table of Contents
- Overview
- Sources & Routes of Exposure
- Toxicokinetics
- Mechanism of Toxicity
- Symptoms & Health Effects
- Diagnosis & Laboratory Testing
- Treatment & Management
- Prevention & Risk Reduction
- Related Topics
- Key Research Papers
- Connections
- Featured Videos
1. Overview
Chromium is a single chemical element, but in the human body it leads a double life, and the difference between its two faces is the difference between a trace nutrient and a recognized human carcinogen. Everything turns on a property chemists call the oxidation state — how many electrons the chromium atom has given up. Trivalent chromium, written Cr(III), is the form found in food, soil, and the supplement bottle. It is the (still-debated) form that may play a minor role in how the body handles blood sugar, and on its own it is relatively non-toxic; cells absorb it poorly. Hexavalent chromium, written Cr(VI) and known popularly as chromium-6, is a different beast entirely: a corrosive, intensely reactive industrial chemical that the International Agency for Research on Cancer (IARC) classifies as a Group 1 carcinogen — the category reserved for agents with sufficient evidence of causing cancer in humans.
To keep the two straight, it helps to remember a simple rule of thumb: the chromium in your spinach, broccoli, and brewer's yeast is Cr(III) and is essentially the "safe" form, while the chromium in chrome-plating tanks, welding fumes, and certain contaminated wells is Cr(VI) and is the dangerous form. This page is about Cr(VI). For the nutritional story — food sources, the glucose-tolerance debate, and supplement safety — see the companion page on essential Chromium. Confusing the two is one of the most common and consequential mistakes in popular writing about this metal.
Most people first heard the phrase "hexavalent chromium" from the 2000 film Erin Brockovich, which dramatized a real case: the town of Hinkley, California, where the utility Pacific Gas and Electric Company (PG&E) had used Cr(VI) as a rust inhibitor in cooling towers and allowed the chromium-laden wastewater to seep into the groundwater that supplied residents' wells. The resulting litigation ended in a landmark settlement and turned "chromium-6 in the drinking water" into a household phrase. That story is the public face of a much older occupational hazard — lung cancer, nasal injury, and skin ulcers among chrome-platers, welders, pigment makers, and tannery workers — that physicians and public-health agencies have tracked for more than a century.
Why this distinction matters for ordinary readers
Because the words "chromium" and "chromium picolinate supplement" sound reassuring, people sometimes assume that any chromium exposure is harmless, or conversely panic that their multivitamin contains a carcinogen. Neither is correct. The supplement is Cr(III). The carcinogen is Cr(VI). Throughout this article, when you see "chromium-6," read it as the corrosive, cancer-causing industrial form — chemically and biologically distinct from the chromium you eat.
2. Sources & Routes of Exposure
Hexavalent chromium does not occur in large amounts in pristine nature; it is overwhelmingly a product of human industry, where chromium is deliberately oxidized to the Cr(VI) state because that form is useful for plating, pigments, and corrosion control. Understanding who is exposed, and by which route, is the key to understanding the very different patterns of illness it causes.
Occupational sources (mostly inhalation and skin)
- Chrome electroplating. Decorative and "hard" chrome plating uses chromic acid baths; the bubbling tanks release a fine acidic mist of Cr(VI) that workers breathe and that settles on skin. This is the classic high-exposure setting.
- Stainless-steel and high-alloy welding. Welding or cutting stainless steel generates fume in which some of the chromium is converted to Cr(VI). Welders are among the largest exposed populations worldwide.
- Chromate pigment production and use. Bright yellow, orange, and green chromate pigments (used historically in paints, inks, and plastics) are Cr(VI) compounds; making or sanding them releases respirable dust.
- Leather tanning. Chrome tanning uses chromium salts; although the tanning agent is mostly Cr(III), Cr(VI) can form in finished leather and in the workplace, and is a notable cause of skin disease.
- Portland cement and construction. Cement contains small amounts of Cr(VI) as an impurity. Wet cement on the skin is a leading cause of occupational chromium dermatitis in construction workers.
- Wood preservation, corrosion inhibitors, and chromate conversion coatings (for example on aircraft aluminum) round out the list.
Environmental and drinking-water sources (ingestion)
The general public's main concern is contaminated drinking water, the Hinkley scenario. Cr(VI) is highly soluble and mobile in groundwater, so industrial discharges, improper waste disposal, leaking plating operations, and certain natural geologic formations can raise Cr(VI) levels in wells and municipal supplies. Because Cr(VI) does not bind to soil the way many metals do, it can travel long distances underground. Unlike inhaled chromium, ingested chromium produces a different — and scientifically more contested — set of health concerns, discussed in the symptoms section below.
What is not a meaningful Cr(VI) source
Food is essentially a Cr(III) source, not a Cr(VI) source; cooking and stomach acid further favor the trivalent form. Chromium dietary supplements (chromium picolinate, chromium chloride, chromium polynicotinate) are Cr(III). Stainless-steel cookware leaches only trace, mostly trivalent chromium. The takeaway: Cr(VI) exposure is dominated by industrial air and skin contact for workers, and by contaminated water for communities — not by ordinary diet.
3. Toxicokinetics
"Toxicokinetics" is simply the story of what the body does to a poison — how it gets in, where it goes, how it is transformed, and how it leaves. For chromium, this story is dominated by one chemical fact: Cr(VI) crosses cell membranes easily, while Cr(III) does not. That single asymmetry explains why the two forms differ so dramatically in toxicity.
Absorption
Cr(VI) is absorbed far more efficiently than Cr(III) by every route. In the gut, only a small percentage of ingested Cr(III) is taken up, whereas Cr(VI) is absorbed more readily — though much of swallowed Cr(VI) is chemically reduced to Cr(III) by saliva, stomach acid, and gut contents before it can be absorbed, a built-in detoxifying step. In the lungs, inhaled Cr(VI) particles deposit in the airways and are absorbed into the blood; some chromate also lodges in lung tissue for long periods, which is relevant to its role in lung cancer. Through intact skin, absorption is normally low, but it rises when the skin is damaged or when exposure is heavy and prolonged.
Distribution and the critical reduction step
Once Cr(VI) enters the bloodstream, it is taken up by red blood cells and tissues and is steadily reduced to Cr(III) by biological reducing agents such as ascorbate (vitamin C) and glutathione. This reduction is protective when it happens outside cells, because Cr(III) cannot easily get back in. But the danger arises when reduction happens inside the cell, after the chromate ion has already slipped through the membrane — the reactive intermediates generated along the way are what damage DNA (see the mechanism section). Chromium that ends up bound inside red cells reflects past Cr(VI) exposure, which is one reason whole-blood chromium can lag behind a recent exposure.
Elimination
Absorbed chromium is excreted mainly by the kidneys in the urine, with a smaller amount leaving through bile and feces. Urinary excretion is relatively prompt for recent exposure, which is exactly why urine chromium is the workhorse biomarker of recent uptake (see Diagnosis). However, chromium that has become tightly bound in tissues such as lung can persist for months to years, so a single urine measurement reflects recent exposure rather than the whole accumulated burden.
4. Mechanism of Toxicity
Why is one oxidation state of an element a nutrient and the other a carcinogen? The answer is a small, elegant piece of chemistry that has been worked out in detail over the past few decades and is captured well in mechanistic reviews of chromium genotoxicity.
The "Trojan horse" entry
Inside cells and in water, Cr(VI) exists as the chromate ion (and at higher concentrations as dichromate). This ion is shaped and charged much like the everyday biological anions sulfate and phosphate. Cells have dedicated transporters that pull sulfate and phosphate inside, and these transporters cannot tell the difference — so they usher chromate in as well. In effect, Cr(VI) is a Trojan horse: it disguises itself as a nutrient anion and rides the cell's own machinery across the membrane. Trivalent chromium, by contrast, has no such disguise and is largely shut out, which is the fundamental reason Cr(VI) is far more toxic than Cr(III).
Intracellular reduction: the damage happens on the way down
Once inside, chromate is chemically unstable and is reduced step by step — from Cr(VI) through short-lived Cr(V) and Cr(IV) intermediates — until it reaches stable Cr(III). The reducing agents are the same molecules that protect us elsewhere: ascorbate, glutathione, and various enzymes. The catch is that this intracellular reduction is precisely what makes Cr(VI) dangerous. Each step generates reactive intermediates and reactive oxygen species (ROS), and the reaction produces Cr(III) right next to the DNA, where it forms chromium-DNA adducts and DNA-protein and DNA-DNA crosslinks. The combination of oxidative damage and bulky chromium adducts leads to mutations, chromosome breakage, and genomic instability — the molecular hallmarks of a carcinogen.
From DNA damage to cancer, and to cell death
At lower, chronic exposures, the surviving damaged cells can carry forward mutations that, over years, drive cancer — this is the pathway behind occupational lung cancer. At higher, acute exposures, the oxidative onslaught and crosslinking overwhelm the cell, triggering cell-cycle arrest and programmed cell death (apoptosis) on a large scale, which manifests clinically as the corrosive tissue injury and organ failure of acute poisoning. The same chemistry, then, produces slow cancer at low dose and rapid corrosive injury at high dose.
Why context (extracellular vs. intracellular reduction) decides the outcome
It is worth restating the paradox at the heart of chromium toxicology: reduction of Cr(VI) is both the body's main defense and the source of its harm. When reduction is completed in the blood and extracellular fluid — for example by abundant vitamin C — the resulting Cr(III) is locked out of cells and the threat is largely neutralized. When reduction instead occurs inside the cell, the same reaction becomes a genotoxic event. This is why the body's reducing capacity, and therapeutic reductants, are central to both prevention and treatment.
5. Symptoms & Health Effects
The health effects of chromium-6 sort cleanly by route of exposure and by acute versus chronic timing. Skin contact causes skin disease; inhalation causes airway and lung disease; high-dose ingestion causes corrosive, multi-organ poisoning. Below, the effects are grouped the way a clinician would think about them.
Skin (dermal) effects
- Allergic contact dermatitis ("chrome dermatitis," "cement eczema"). Chromium is one of the most common causes of allergic contact dermatitis worldwide. Once a person is sensitized, even small re-exposures — from cement, leather, or metal — trigger an itchy, red, scaling, sometimes blistering rash, typically on the hands. Construction workers handling wet cement are a classic example.
- Chrome ulcers ("chrome holes"). Direct contact with concentrated Cr(VI), especially on broken skin or in skin creases and over knuckles, produces painless, punched-out ulcers with a hard rim that heal slowly and can leave scars. They are a marker of heavy industrial exposure.
- Irritant burns. Chromic acid is corrosive; splashes can cause chemical burns.
Respiratory effects (acute and chronic)
- Nasal injury. A hallmark of chronic chrome exposure is damage to the nasal lining: irritation, crusting, nosebleeds, ulceration of the nasal septum, and in significant exposures, perforation of the nasal septum — an actual hole through the cartilage wall between the nostrils. This finding in a worker is a strong clue to chromate exposure.
- Acute airway irritation and asthma. Breathing Cr(VI) mist can cause cough, wheeze, shortness of breath, and chest tightness; chromium is a recognized cause of occupational asthma, and high acute inhalation can inflame the lower airways.
- Lung cancer (chronic, the headline hazard). Long-term occupational inhalation of Cr(VI) causes lung cancer; this is the basis for IARC's Group 1 classification of Cr(VI) compounds. The risk has been documented for decades among chromate-production workers, chrome platers, and pigment makers, and rises with cumulative exposure. Some evidence also links Cr(VI) inhalation to cancers of the nasal cavity and sinuses.
Gastrointestinal and systemic effects of ingestion
Swallowing a large dose of a Cr(VI) compound (for example chromic acid or a dichromate salt, whether accidental or deliberate) is a medical emergency. Because Cr(VI) is corrosive, it produces:
- Hemorrhagic gastroenteritis — severe abdominal pain, vomiting (sometimes bloody), and bloody diarrhea from corrosive injury to the stomach and intestine.
- Hemolysis — destruction of red blood cells, which can darken the urine and cause anemia.
- Acute kidney injury (renal failure) — the kidneys, which excrete chromium, can be directly damaged, sometimes leading to the need for dialysis.
- Liver injury (hepatic failure) — elevated liver enzymes and, in severe cases, liver failure.
- Cardiovascular collapse and shock in the most severe poisonings.
Lower-dose, longer-term ingestion of Cr(VI) in drinking water is the contested arena. In two-year studies, the U.S. National Toxicology Program (NTP) gave rodents Cr(VI) in their water and found tumors of the gastrointestinal tract (oral cavity and small intestine), establishing that ingested Cr(VI) can be carcinogenic in animals. Whether typical environmental drinking-water levels cause cancer in humans is genuinely under study and debated. Ecological studies of communities exposed through water — including the Greek industrial-area study and a Chinese population study — have reported associations with stomach and other cancers, and a meta-analysis found a modest increase in stomach cancer among occupationally exposed workers. Critics note the limitations of ecological data, the protective reduction of Cr(VI) in the stomach, and uncertainties in dose. The honest summary: inhaled Cr(VI) is a proven human lung carcinogen; ingested Cr(VI) is a proven animal carcinogen and a biologically plausible but not fully settled human one, which is why agencies treat it cautiously and continue to research it.
6. Diagnosis & Laboratory Testing
There is no single test that proves "chromium-6 poisoning," because once chromium is inside the body it is reduced to Cr(III) and a urine or blood test cannot easily distinguish which form a person was exposed to. Diagnosis therefore combines exposure history (occupation, water source, the Hinkley-type scenario), physical findings (chrome ulcers, nasal septum changes, dermatitis), and laboratory biomarkers, interpreted together.
Urine chromium — the primary biomarker
The workhorse test for recent exposure is the urinary chromium concentration, because absorbed chromium is excreted mainly by the kidneys. It reflects recent uptake (the past day or two) rather than long-term body burden. Units matter and are a common source of confusion:
- Results are reported either as a concentration in micrograms per liter (µg/L) of urine, or — to correct for how dilute the urine is — as micrograms per gram of creatinine (µg/g creatinine). Occupational reference values are usually expressed per gram of creatinine.
- In people without occupational exposure, urinary chromium is typically very low — on the order of a fraction of a microgram up to a few µg/L; many unexposed individuals fall well below 1 µg/L.
- For workers, exposure is judged against an occupational Biological Exposure Index (BEI). The American Conference of Governmental Industrial Hygienists (ACGIH) sets a BEI for total chromium in urine measured at the end of a shift at the end of the workweek, with a smaller allowable increase across a single shift. The post-shift, end-of-week timing exists because chromium accumulates over the workweek; comparing a value to the right reference therefore depends on exactly when the sample was taken.
Because urine chromium captures total chromium (Cr(III) plus the chromium derived from Cr(VI)), a high value signals exposure and prompts a hunt for the source; it does not by itself prove the hexavalent form was responsible. Trends over time and comparison with co-workers are often more informative than a single number.
Occupational biomonitoring programs
In regulated workplaces, urine chromium is collected as part of a structured medical surveillance program: baseline and periodic samples, standardized collection timing, and a designated occupational physician who interprets results against the BEI and looks for the early clinical signs (nasal exam, skin exam, respiratory symptoms). Rising group urine levels can flag a failing ventilation system before any worker becomes ill — biomonitoring as an early-warning system, not just a diagnosis after the fact.
Other tests, by clinical scenario
- Blood (whole-blood or red-cell) chromium can be used; chromium bound inside red cells can reflect earlier Cr(VI) exposure, but blood is less convenient than urine for routine monitoring.
- Nasal examination (anterior rhinoscopy) documents septal ulceration or perforation in chronically exposed workers.
- Chest imaging (chest X-ray, CT) is used when lung cancer or other respiratory disease is suspected on the basis of symptoms and exposure history; chromium has no specific imaging signature, so imaging is for finding disease, not for measuring the metal.
- Upper GI endoscopy is indicated after a corrosive Cr(VI) ingestion to grade the extent of esophageal and gastric injury.
- Supportive labs in acute poisoning — complete blood count and a blood film (for hemolysis), kidney function (creatinine), liver enzymes, and electrolytes — track the multi-organ effects rather than the chromium level itself.
7. Treatment & Management
There is no single "antidote" that neutralizes chromium throughout the body the way a chelator might be used for lead. Instead, treatment follows three logical lines: stop and remove the exposure (decontamination), chemically convert Cr(VI) to the far less toxic Cr(III) using reducing agents, and support the organs that are injured. The right mix depends entirely on the route and severity. This section is educational, not a treatment manual; any real exposure needs professional and often emergency medical care, ideally with input from a poison control center.
Decontamination
- Skin and eyes: remove contaminated clothing and irrigate the skin or eyes copiously with water; chromic-acid burns are treated as chemical burns. Prompt, thorough rinsing limits absorption and tissue damage.
- Inhalation: move the person to fresh air; give oxygen and treat bronchospasm as needed.
- Ingestion: this is managed as a corrosive ingestion. Inducing vomiting is generally avoided because re-exposing the esophagus to a corrosive is harmful; decisions about gastric decontamination, dilution, and endoscopy are made by clinicians based on what and how much was swallowed.
Reducing agents: turning Cr(VI) into Cr(III)
The most chromium-specific therapeutic idea is to supply reducing agents that convert Cr(VI) to Cr(III), because Cr(III) is poorly absorbed and far less able to enter cells. Ascorbic acid (vitamin C) is the best-known example and has been used in several ways:
- Topically, on chromic-acid skin burns and chrome ulcers, to reduce surface Cr(VI) and limit further injury.
- Orally or intravenously in poisoning, on the rationale of reducing Cr(VI) before and after absorption; high-dose intravenous vitamin C has been reported in serious ingestions.
- Other reductants and supportive agents (for example N-acetylcysteine, which restores glutathione, the body's own Cr(VI)-reducing molecule) have also been used or proposed.
It is important to be candid that the evidence base for these reductant therapies is largely mechanistic and based on case reports and animal data rather than large clinical trials; they are biologically rational and used in practice, but they are adjuncts to — not replacements for — decontamination and organ support.
Supportive and organ-directed care
- Kidneys: aggressive intravenous fluids to maintain urine output; hemodialysis if acute kidney injury is severe (dialysis also removes some circulating chromium).
- Blood: transfusion for significant hemolysis or blood loss.
- Liver: supportive care and monitoring for hepatic failure.
- GI tract: management of corrosive injury, pain control, and later surveillance for strictures.
- Cancer surveillance: for chronically exposed workers, the long-term "management" is really screening and prompt evaluation of respiratory symptoms, since the chief delayed risk is lung cancer.
8. Prevention & Risk Reduction
Because Cr(VI) is almost entirely a man-made exposure, it is also one of the more preventable carcinogens — the controls are well understood, and the main challenge is applying them consistently. Prevention operates at two levels: the workplace and the water supply.
Workplace controls (the regulatory backbone)
In the United States, the Occupational Safety and Health Administration (OSHA) regulates Cr(VI) under a dedicated hexavalent chromium standard, which sets a legally enforceable permissible exposure limit (PEL) for airborne Cr(VI) and an "action level" that triggers monitoring. The standard codifies the classic industrial-hygiene hierarchy of controls:
- Substitution — replacing Cr(VI) processes with safer alternatives where possible (for example trivalent-chromium or non-chromium plating and coatings).
- Engineering controls — chiefly local exhaust ventilation to capture mist and fume at the source, plus enclosure of processes; this is the single most effective protection for platers and welders.
- Work practices — wet methods, good housekeeping to avoid resuspending dust, and no eating or smoking in work areas.
- Personal protective equipment — appropriate respirators, gloves, and protective clothing, used as a last layer rather than the first.
- Medical surveillance and biomonitoring — periodic urine chromium and clinical exams (see Diagnosis) to verify the controls are working.
Drinking-water controls
For the public, prevention means keeping Cr(VI) out of water and removing it when present. The U.S. Environmental Protection Agency (EPA) sets a federal drinking-water limit for total chromium (currently 0.1 mg/L, i.e. 100 µg/L), and California has gone further by adopting a separate, stricter standard specifically for hexavalent chromium. Where contamination exists, water can be treated to remove Cr(VI) — for example by reducing it to Cr(III) and filtering, or by ion exchange and reverse osmosis. Communities with affected wells (the enduring lesson of Hinkley) rely on source control, regular testing, and treatment.
Practical takeaways for individuals
- If you work with chrome plating, stainless-steel welding, chromate pigments, tanning, or cement, treat ventilation, gloves, and respirators as essential and participate in any biomonitoring program offered.
- If you are concerned about your water, find out whether your supplier reports chromium-6 specifically; private wells can be tested by a certified laboratory.
- Do not confuse this with your supplement: chromium picolinate and the chromium in food are Cr(III), not chromium-6. See the essential Chromium page for that separate discussion.
9. Related Topics
- Chromium (essential) — the trivalent, dietary form: food sources, the glucose-tolerance debate, and supplement safety. Read this to keep Cr(III) and Cr(VI) straight.
- Toxic Minerals — the hub page for the toxic and heavy-metal cluster.
- Heavy Metals — overview of the broader heavy-metal toxicity family.
- Nickel — another metal that causes allergic contact dermatitis and shares carcinogenic mechanisms.
- Cadmium — a Group 1 metal carcinogen with prominent lung and kidney effects.
- Arsenic — a drinking-water contaminant whose carcinogenicity, like chromium's, hinges on redox chemistry.
- Vitamin C (ascorbic acid) — the reducing agent central to both detoxifying Cr(VI) and treating exposure.
- Pulmonology — lung disease and lung cancer, the chief chronic hazard of inhaled chromium-6.
- Kidney Disease — the kidney injury seen in acute Cr(VI) poisoning.
- Lab Tests — how biomarkers like urine chromium are measured and interpreted.
10. Key Research Papers
- Nickens KP, Patierno SR, Ceryak S. Chromium genotoxicity: a double-edged sword. Chemico-Biological Interactions 2010;188(2):276–288.
- DesMarias TL, Costa M. Mechanisms of chromium-induced toxicity. Current Opinion in Toxicology 2019;14:1–7.
- Wise SS, Wise JP Sr. Chromium and genomic stability. Mutation Research / Fundamental and Molecular Mechanisms of Mutagenesis 2012;733(1–2):78–82.
- Sun H, Brocato J, Costa M. Oral chromium exposure and toxicity. Current Environmental Health Reports 2015;2(3):295–303.
- Welling R, Beaumont JJ, Petersen SJ, Alexeeff GV, Steinmaus C. Chromium VI and stomach cancer: a meta-analysis of the current epidemiological evidence. Occupational and Environmental Medicine 2015;72(2):151–159.
- Linos A, Petralias A, Christophi CA, et al. Oral ingestion of hexavalent chromium through drinking water and cancer mortality in an industrial area of Greece — an ecological study. Environmental Health 2011;10:50.
- Salnikow K, Zhitkovich A. Genetic and epigenetic mechanisms in metal carcinogenesis and cocarcinogenesis: nickel, arsenic, and chromium. Chemical Research in Toxicology 2008;21(1):28–44. [PubMed]
- Beaumont JJ, Sedman RM, Reynolds SD, et al. Cancer mortality in a Chinese population exposed to hexavalent chromium in drinking water. Epidemiology 2008;19(1):12–23. [PubMed]
- Pavesi T, Moreira JC. Mechanisms and individuality in chromium toxicity in humans. Journal of Applied Toxicology 2020;40(9):1183–1197. [PubMed]
- Chiu A, Shi XL, Lee WKP, et al. Review of chromium(VI) apoptosis, cell-cycle-arrest, and carcinogenesis. Journal of Environmental Science and Health, Part C 2010;28(3):188–230. [PubMed]
- Agency for Toxic Substances and Disease Registry (ATSDR). Toxicological Profile for Chromium. U.S. Department of Health and Human Services. atsdr.cdc.gov
- International Agency for Research on Cancer (IARC). Chromium (VI) compounds. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, Volume 100C (Arsenic, Metals, Fibres and Dusts). publications.iarc.fr
- U.S. Environmental Protection Agency (EPA). Chromium(VI), CASRN 18540-29-9. Integrated Risk Information System (IRIS). iris.epa.gov
- Occupational Safety and Health Administration (OSHA). Hexavalent Chromium standard, 29 CFR 1910.1026. U.S. Department of Labor. osha.gov
Connections
- Chromium (essential / trivalent)
- Toxic Minerals
- Heavy Metals
- Nickel
- Cadmium
- Arsenic
- All Minerals
- Vitamin C
- Pulmonology
- Kidney Disease
- Lab Tests