Tin and Organotin Toxicity: From Food Cans to Neurotoxic Compounds
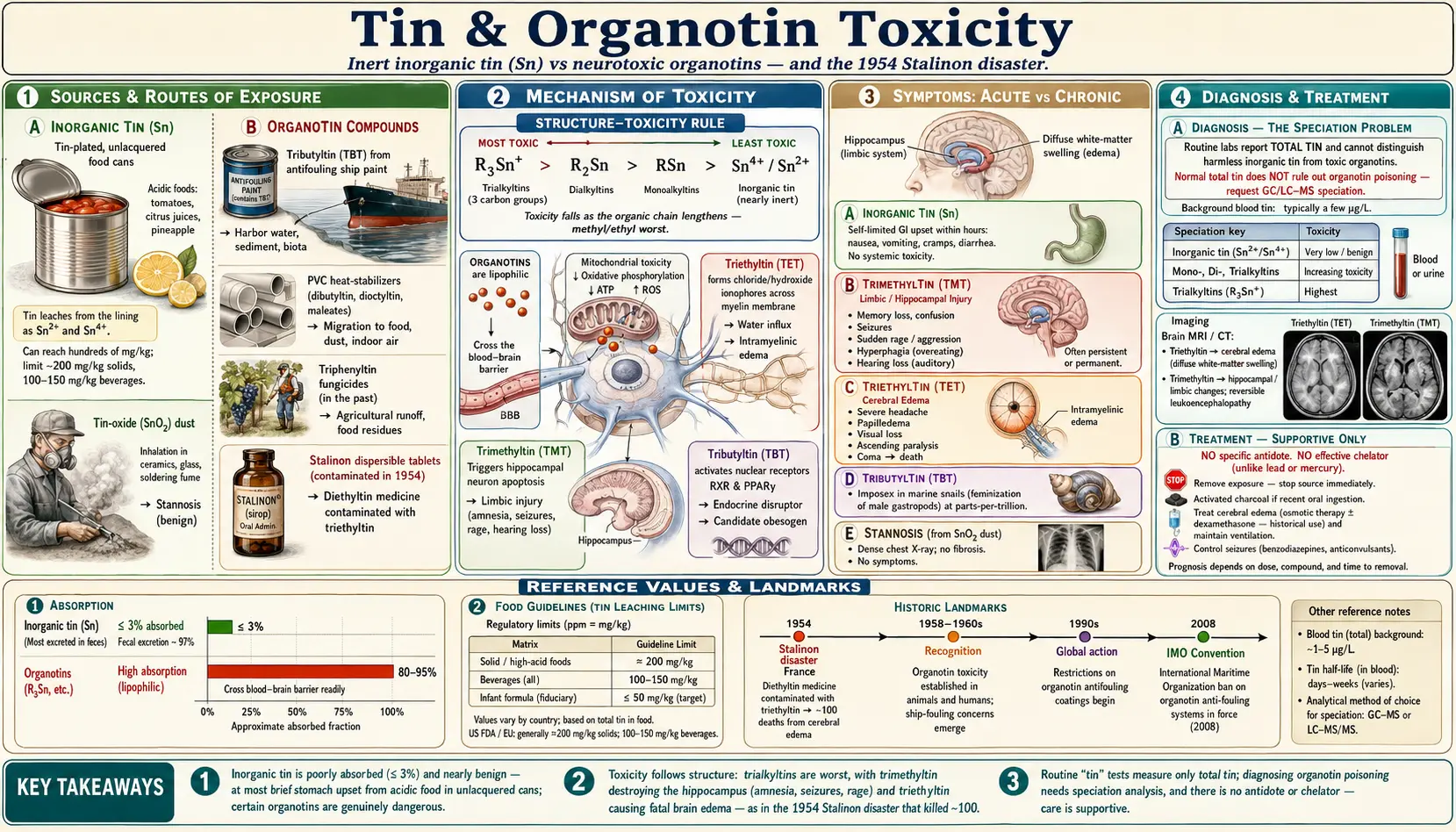
Table of Contents
- Overview
- Sources & Routes of Exposure
- Toxicokinetics
- Mechanism of Toxicity
- Symptoms & Health Effects
- Diagnosis & Laboratory Testing
- Treatment & Management
- Prevention & Risk Reduction
- Related Topics
- Key Research Papers
- Connections
- Featured Videos
1. Overview
Tin (chemical symbol Sn, from the Latin stannum) is a soft, silvery metal humans have used for thousands of years — in bronze, in solder, and as the shiny inner coating of the "tin can." For most people this everyday tin is remarkably safe. The story of tin's toxicity is really a story of two completely different chemistries that happen to share the same element and could hardly differ more in how dangerous they are.
The first form is inorganic tin — the metal itself and simple tin salts (such as stannous chloride). It is poorly absorbed by the body and has low systemic toxicity; when it causes trouble at all, the trouble is usually a self-limited bout of stomach upset after someone eats highly acidic food that has sat in an unlacquered tin-plated can.
The second form is organotin compounds — molecules in which tin is bonded directly to carbon (for example trimethyltin, triethyltin, and tributyltin). These synthetic compounds are an entirely different hazard class. Some are among the more potent neurotoxins known to industrial medicine, capable of injuring specific regions of the brain, causing fatal brain swelling, disrupting hormones at vanishingly small concentrations, and harming the immune system. The single most important idea on this page is this distinction: inorganic tin is generally benign; certain organotins are genuinely dangerous.
This difference is not academic. A landmark tragedy — the Stalinon disaster in France in 1954 — killed roughly one hundred people because an oral medicine made with an organotin was contaminated with a far more toxic organotin. Both forms are "tin," but only one is lethal.
2. Sources & Routes of Exposure
Because inorganic and organotin compounds are used so differently, the people exposed to each, and the way they are exposed, are also different. Understanding the source usually tells you which chemistry — and therefore which risk — is in play.
Inorganic Tin from Food Cans
The classic inorganic-tin exposure is dietary. Steel cans are often plated with a thin layer of tin to resist corrosion. When the can is unlacquered (no protective interior coating) and the food inside is acidic — tomatoes and tomato products, citrus and other fruit, fruit juices, pineapple — the acid slowly dissolves tin into the food, especially after the can is opened and oxygen reaches the contents. Concentrations can climb into the hundreds of milligrams of tin per kilogram of food. International food-safety bodies generally set a guideline limit around 200 mg/kg for solid canned foods and roughly 100–150 mg/kg for canned beverages, levels chosen specifically to prevent the acute stomach upset described later. Modern lacquered (enamel-lined) cans have made high-tin exposures uncommon.
Tributyltin (TBT) in Marine Paint
From the 1960s onward, tributyltin (TBT) was added to ship-hull "antifouling" paints to kill barnacles, algae, and other organisms that slow vessels and increase fuel use. TBT worked extremely well — and leached steadily into harbors and coastal waters worldwide. It proved so toxic to marine life that it became one of the most regulated marine pollutants in history (see Mechanism and Symptoms). Human exposure to TBT comes mainly through seafood and through occupational contact during paint manufacturing and ship maintenance.
Other Organotins: PVC, Agriculture, Wood, and Catalysts
- PVC heat stabilizers: Mono- and di-organotins (dibutyltin, dioctyltin) keep polyvinyl chloride plastic from degrading when heated. These mono- and di-substituted compounds are considerably less toxic than the tri-substituted organotins, and dioctyltins are approved in some food-contact plastics.
- Agricultural fungicides: Triphenyltin (fentin) and relatives have been used as fungicides on crops such as potatoes and sugar beets, and as molluscicides.
- Wood preservatives, biocides, and catalysts: Tributyltin oxide and similar compounds protected timber and textiles from rot, and organotins catalyze the production of silicones and polyurethane foams.
Pharmaceutical Contamination and Inhaled Dust
Historically, the most lethal human organotin exposure came not from industry but from medicine: the Stalinon preparation (discussed below) was taken by mouth for skin infections and was contaminated with triethyltin. That route is essentially closed today, but it remains the defining example of how an organotin can reach — and kill — people directly. Separately, workers who grind, smelt, or polish tin and tin oxide can inhale fine tin oxide dust over many years, causing a distinct (and notably benign) lung condition called stannosis, covered under Symptoms.
3. Toxicokinetics
"Toxicokinetics" describes what the body does to a substance — how much gets in, where it goes, and how it leaves. Here again, inorganic tin and organotins behave very differently, and that difference explains the gap in their toxicity.
Inorganic Tin: Poorly Absorbed, Quickly Gone
Inorganic tin is poorly absorbed from the gut — most studies estimate only a few percent of an ingested dose (often cited as roughly 3% or less) crosses into the bloodstream, while the large remainder passes through and is eliminated in the feces. The small absorbed fraction does not accumulate dangerously; some deposits in bone and a portion leaves in urine. Because so little is absorbed and what is absorbed clears efficiently, ordinary dietary tin rarely causes systemic poisoning — the gut is essentially a barrier.
Organotins: Lipophilic Compounds That Cross Membranes
Organotin compounds are lipophilic (fat-loving) because of their carbon–tin bonds, which lets them dissolve into and pass through the fatty membranes around cells. This changes everything: organotins are absorbed far more readily than inorganic tin, distribute widely, and — critically — the smaller trialkyltins can cross the blood–brain barrier, the filter that normally keeps many toxins out of the brain. Once inside, they reach the very tissues (brain, immune organs, endocrine glands) that make them harmful.
Metabolism by Dealkylation
The body slowly breaks organotins down by dealkylation — stripping off carbon groups one at a time (triethyltin → diethyltin → monoethyltin), heading toward inorganic tin. Because toxicity falls sharply as carbon groups are removed, this metabolism is partly a detoxification pathway, but it is slow for the most toxic trialkyltins — one reason their effects build up and persist. Triethyltin in particular is excreted slowly, via both bile and urine.
4. Mechanism of Toxicity
Why are certain organotins so damaging while inorganic tin is nearly harmless, and why does the danger depend so precisely on the molecule's structure? Several overlapping mechanisms are responsible, and they help explain the very specific syndromes seen in poisoned people.
The Structure–Toxicity Rule
A consistent finding across organotin toxicology is that toxicity is governed by how many carbon groups are attached to the tin and how long those chains are. Trialkyltins (three carbon groups, as in trimethyltin and triethyltin) are the most toxic to mammals; di- and mono-substituted compounds are far less so. Among the trialkyltins, toxicity decreases as the chain lengthens — the small methyl and ethyl compounds are the most dangerous. This is the reason trimethyltin and triethyltin cause devastating brain injury while the bulkier tributyltin acts more as a hormone disruptor than an acute neurotoxin.
Mitochondrial Poisoning, Ion Disruption, and Calcium
Organotins interfere with mitochondria, the structures that generate cellular energy, disrupting oxidative phosphorylation (the production of ATP, the cell's energy currency), partly by acting as ionophores. Cells with high energy demands, such as neurons, are especially vulnerable when their power supply fails. Triethyltin and related compounds act specifically as chloride/hydroxide ionophores — ferrying chloride (Cl−) and hydroxide (OH−) ions across membranes that should control those flows tightly. The result is a breakdown of ion and water balance: chloride and water are pulled into the layers of myelin (the insulation around nerve fibers), producing the intramyelinic edema — fluid-filled swelling within the brain's white matter — that is the hallmark of triethyltin injury. Organotins also disturb calcium homeostasis, and abnormal intracellular calcium is a well-known trigger for cell death.
Triggering Neuronal Apoptosis
Trimethyltin, in particular, drives vulnerable neurons into apoptosis (programmed cell death). It shows a striking preference for the limbic system, especially the hippocampus — the brain's memory hub — where it destroys specific populations of neurons. This selective, region-specific killing is what produces the distinctive memory loss, behavioral changes, and seizures of trimethyltin poisoning, and it is the focus of much of the modern research described below.
Endocrine Disruption (TBT)
Tributyltin has a separate and now-famous mechanism: it binds and activates two nuclear hormone receptors, the retinoid X receptor (RXR) and peroxisome proliferator-activated receptor gamma (PPARγ). These receptors act as master switches for fat-cell development and hormone signaling. By switching them on inappropriately, TBT behaves as an endocrine disruptor — and it is one of the most-studied candidate "obesogens," chemicals hypothesized to promote fat accumulation. The same receptor activity, at extraordinarily low concentrations, masculinizes female marine snails (see Symptoms).
5. Symptoms & Health Effects
The symptoms of tin exposure depend almost entirely on which form is involved, and on whether exposure is sudden (acute) or sustained (chronic). The most important and distinctive effects are the organotin neurological syndromes, so they receive the most attention here.
Inorganic Tin: Mostly Gastrointestinal Upset
Eating food high in inorganic tin (typically acidic food from unlacquered cans) usually produces a self-limited bout of gastrointestinal irritation within half an hour to a few hours: nausea, vomiting, abdominal cramps, bloating, and diarrhea, sometimes with headache. Such outbreaks have been linked to canned fruit and juices when tin rose well above the ~200 mg/kg guideline. The episode is unpleasant but short-lived, resolving once the food clears; serious systemic poisoning from dietary inorganic tin is not a typical concern because so little is absorbed.
Trimethyltin Syndrome (Limbic / Hippocampal Injury)
Trimethyltin (TMT) produces one of the most striking toxic syndromes in clinical toxicology, reflecting its destruction of limbic and hippocampal neurons. Reported features — documented in both accidental human poisonings and animal models — include:
- Memory loss and confusion (consistent with hippocampal damage);
- Disorientation and impaired concentration;
- Seizures;
- Rage, irritability, and aggression — sudden, sometimes violent behavioral change is a notably characteristic feature;
- Hyperphagia (markedly increased appetite/overeating);
- Hearing loss (the auditory system is a target);
- Headache, disturbed sleep, depression, and in severe cases a depressed level of consciousness.
Symptoms can be delayed after exposure and may persist long after the exposure ends, mirroring the permanent loss of neurons. The constellation of amnesia, seizures, and abrupt aggression in someone with a possible organotin exposure should raise suspicion of trimethyltin specifically.
Triethyltin Syndrome (Cerebral Edema)
Triethyltin (TET) causes a different picture — not selective neuron killing but diffuse swelling of the brain. By driving fluid into the myelin and white matter (intramyelinic edema), it raises pressure inside the skull (increased intracranial pressure). The clinical result is dominated by the consequences of that pressure and swelling:
- Severe headache;
- Papilledema (swelling of the optic disc at the back of the eye, a physical sign of raised intracranial pressure);
- Visual disturbances;
- Weakness or paralysis, often ascending;
- Nausea and vomiting, and in severe cases progression to coma.
This is the syndrome that killed and disabled the victims of the Stalinon disaster.
The Stalinon Disaster (France, 1954)
"Stalinon" was a French oral medication marketed for boils, acne, and other skin infections. Its active ingredient was an organotin (diethyltin diiodide), but the manufactured product was contaminated with triethyltin, the far more toxic relative. The consequence was a mass poisoning: roughly 100 people died, and many more were seriously injured, from cerebral edema and raised intracranial pressure — severe headaches, visual loss, and paralysis. The Stalinon catastrophe became a landmark in toxicology and pharmaceutical regulation, a permanent illustration both of organotin neurotoxicity and of the dangers of contaminated medicines.
Tributyltin: "Imposex" and Endocrine Effects
Tributyltin's signature effect appears in marine snails. At concentrations as low as a few parts per trillion in seawater, TBT causes imposex — literally "imposed sex" — in which female snails develop male sex organs (a penis and vas deferens), often blocking the release of eggs and causing local populations to collapse. Imposex in species such as the dog whelk became a sensitive global biomarker of TBT pollution. The discovery that a marine paint could sterilize shellfish at trace levels drove the worldwide ban of organotin antifouling paints under the International Maritime Organization's Anti-fouling Systems Convention, which entered into force in 2008. In mammals, TBT is studied as an endocrine disruptor, an immunotoxicant (it can suppress immune function), and a candidate obesogen; experimental exposures have been linked to increased fat accumulation, including effects that may carry across generations.
Stannosis: A Benign Lung Condition
Years of inhaling fine tin oxide dust can cause stannosis, a form of pneumoconiosis (dust-related lung disease). Importantly, stannosis is considered benign: it produces dramatic, dense shadows on chest X-rays (because tin is very efficient at absorbing X-rays), yet it generally does not scar the lung or impair breathing the way silica or asbestos exposure does. It is mainly a radiological curiosity that must be distinguished from more serious dust diseases.
6. Diagnosis & Laboratory Testing
Diagnosing tin-related illness rests on two pillars: a careful exposure history and, where appropriate, laboratory measurement of tin — with one crucial caveat about what the lab is actually measuring.
The Speciation Problem: Total Tin vs. Organotin
This is the single most important laboratory concept on this page. A routine "tin level" measured in blood or urine reports total tin — it does not distinguish harmless inorganic tin from a dangerous organotin. Because dietary inorganic tin is poorly absorbed, blood and urine tin are not reliable markers of inorganic exposure and a normal value cannot rule out a serious organotin poisoning. To identify and quantify the actual toxic species, the laboratory must perform speciation analysis — specialized techniques (such as gas or liquid chromatography coupled to mass spectrometry or atomic-emission/absorption detection) that separate and measure the specific organotin compounds (trimethyltin, triethyltin, tributyltin, and so on). Speciation is a specialized test, not part of routine bloodwork, and clinicians must request it deliberately when an organotin exposure is suspected.
Units and Interpretation
Tin concentrations in biological samples are typically reported in micrograms per liter (µg/L) of blood or urine, or as micrograms per gram of tissue; environmental and food levels are given as milligrams per kilogram (mg/kg) or micrograms per liter for water and beverages. Background blood tin in unexposed people is generally low (on the order of a few µg/L or less). Reference ranges vary between laboratories and methods, so results should always be interpreted against the specific lab's stated range and, ideally, alongside speciation data rather than a single total-tin number.
Neuroimaging in Organotin CNS Poisoning
When the nervous system is involved, brain imaging is central to diagnosis and monitoring. In triethyltin-type poisoning, MRI or CT may show diffuse cerebral/white-matter edema and signs of raised intracranial pressure. In trimethyltin-type injury, imaging may reveal abnormalities in the limbic system and hippocampus consistent with selective neuronal damage, and modern case reports describe a reversible leukoencephalopathy (white-matter change that can partly recover) after organotin exposure. Imaging findings, combined with the clinical syndrome and exposure history, often establish the diagnosis even before speciation results return.
Putting It Together
In practice the workup proceeds by pattern recognition: acidic canned food plus brief vomiting points to benign inorganic tin and needs little testing; occupational organotin handling plus headache, papilledema, and paralysis — or amnesia, seizures, and aggression — points to an organotin and demands neuroimaging and speciation analysis. Recognizing the syndrome is often faster, and more decisive, than waiting for a tin number.
7. Treatment & Management
An honest and important point comes first: for organotin poisoning there is no proven specific antidote and no effective chelator. Unlike lead or mercury — where chelating drugs can bind and remove the metal — chelation has not been shown to help in organotin intoxication, and treatment is therefore supportive: keeping the patient alive and stable while the body slowly clears and metabolizes the compound, and treating each complication as it arises.
Remove the Person from Exposure and Decontaminate
The first step in every case is to stop further exposure — remove the patient from the contaminated environment, discontinue any implicated product or medication, and protect rescuers from secondary contamination. If an organotin (or a large amount of inorganic tin) has been swallowed recently, standard gastrointestinal decontamination (for example timely activated charcoal) may be considered under the guidance of a poison-control center or toxicologist; skin or eye contact is managed with thorough irrigation.
Managing the Neurological Emergencies
- Cerebral edema (triethyltin type): Raised intracranial pressure is a medical emergency managed with the standard tools of neurocritical care — close monitoring, head positioning, osmotic therapy, and airway and ventilation support as needed. (Notably, corticosteroids such as dexamethasone have an experimental history in triethyltin edema, reflected in the older literature.)
- Seizures (trimethyltin type): Seizures are controlled with standard anticonvulsant medications.
- Airway and breathing: Patients with depressed consciousness or progressive weakness/paralysis may require airway protection and ventilatory support.
Supportive Care and Recovery
Beyond the acute emergencies, management is general intensive and supportive care: fluids and electrolytes, monitoring of vital organs, and rehabilitation. Because trimethyltin destroys neurons outright, some deficits — memory problems, behavioral change, hearing loss — can be permanent. Triethyltin's edema may improve as fluid balance is restored, but severe cases can be fatal or leave lasting injury. For inorganic tin, treatment is rarely more than rehydration and symptom relief for the brief gastrointestinal upset, which resolves on its own.
8. Prevention & Risk Reduction
Because the hazards of inorganic and organotin compounds are so different, so are the strategies for avoiding them. Encouragingly, the most dangerous exposures have already been sharply reduced by regulation, and the everyday ones are easy to manage.
For Inorganic Tin (Food)
- Use lacquered/enamel-lined cans, now standard, which largely prevent tin from leaching into food.
- Do not store opened canned food in the can, especially acidic foods like tomatoes, citrus, and fruit juice — transfer leftovers to glass or plastic and refrigerate, since tin dissolves fastest once the can is opened and exposed to air. Discard severely dented, bulging, or rusted cans.
- Food-safety limits (around 200 mg/kg for solid foods, lower for beverages) exist specifically to keep dietary tin below the level that causes stomach upset.
For Organotins (the Real Hazard)
- The TBT marine-paint ban: The IMO Anti-fouling Systems Convention (in force 2008) prohibits organotin antifouling paints worldwide, the central preventive measure against TBT pollution. Tin-free antifouling coatings have replaced them.
- Occupational protection: Workers who manufacture or handle organotins (PVC stabilizers, catalysts, fungicides, legacy paints) need engineering controls, respiratory and skin protection, and exposure monitoring, because organotins are absorbed through skin and lungs as well as the gut.
- Pharmaceutical and product safety: The Stalinon disaster permanently reshaped expectations for purity testing of medicines; preventing organotin contamination of consumer and medical products remains a regulatory priority.
- Agricultural and dietary limits: Restrictions on triphenyltin fungicides and monitoring of organotins in seafood help limit residual human exposure.
9. Related Topics
- Toxic Minerals — overview of the toxic metals and metalloids on this site
- Heavy Metals — shared ideas of absorption, body burden, and chelation
- Lead — a neurotoxic metal where chelation, unlike for organotins, works
- Mercury — whose organic (methylmercury) form is far more neurotoxic than the inorganic, a close parallel to tin
- Arsenic — a metalloid with strongly species-dependent toxicity
- Cadmium — a toxic metal with a long biological half-life
- Aluminum — a low-toxicity but ubiquitous metal
- Manganism — a metal-induced movement disorder
- Parkinson's Disease — a movement disorder with toxic risk factors
- Selenium — an essential mineral that is also toxic in excess
- Zinc — an essential mineral and target of metal toxicity
- Iron — an essential metal central to oxygen transport
- Lab Tests — metal testing and the importance of speciation
- All Minerals — the full mineral library
10. Key Research Papers
- Fait A, Ferioli A, Barbieri F. Organotin compounds. Toxicology. 1994;91(1):77–82. (Concise review of organotin toxicology and the structure–toxicity relationship.)
- "Stalinon": a Therapeutic Disaster. British Medical Journal. 1958;1(5069):515. (Contemporary account of the landmark French organotin mass poisoning.)
- Studer RK, Siegel BA, Morgan J, Potchen EJ. Dexamethasone therapy of triethyltin-induced cerebral edema. Experimental Neurology. 1973;38(3):429–437. (Classic study of triethyltin cerebral edema and an attempted corticosteroid treatment.)
- Harry GJ, McPherson CA, Wine RN, Atkinson K, Lefebvre d'Hellencourt C. Trimethyltin-induced neurogenesis in the murine hippocampus. Neurotoxicity Research. 2003;5(8):623–627. (Demonstrates the hippocampal selectivity of trimethyltin injury.)
- Liu Z, Wang L, Wang Y, Wu S, et al. Quantitative proteomics reveals the neurotoxicity of trimethyltin chloride on mitochondria in the hippocampus of mice. NeuroToxicology. 2023;99:162–176. (Modern mechanistic work linking trimethyltin to mitochondrial injury in the hippocampus.)
- Antizar-Ladislao B. Environmental levels, toxicity and human exposure to tributyltin (TBT)-contaminated marine environment. A review. Environment International. 2008;34(2):292–308. (Comprehensive review of TBT in the marine environment and human exposure.)
- Grün F. The obesogen tributyltin. Vitamins and Hormones. 2014;94:277–325. (Reviews TBT's RXR/PPARγ endocrine mechanism and the obesogen hypothesis.)
- Robertson AJ, Whitaker PH. Radiological changes in pneumoconiosis due to tin oxide. Journal of the Faculty of Radiologists. 1955;6(4):224–233. (Early description of stannosis, the benign tin-dust pneumoconiosis.)
- Dang TT, Doan UV, Nguyen TH, et al. Reversible leukoencephalopathy associated with organotin poisoning. Clinical Toxicology. 2023;61(6):476–478. (Modern human organotin case — PubMed search; PMID 37358038.)
- Fent K. Ecotoxicology of organotin compounds. Critical Reviews in Toxicology. 1996;26(1):3–117. (The definitive organotin ecotoxicology review, including TBT imposex — PubMed search; PMID 8833456.)
- Hirano A, Zimmerman HM, Levine S. Intramyelinic and extracellular spaces in triethyltin intoxication. Journal of Neuropathology and Experimental Neurology. 1968;27(4):581–590. (Classic neuropathology of triethyltin intramyelinic edema — PubMed search; PMID 5687754.)
- Kirchner S, Kieu T, Chow C, Casey S, Blumberg B. Prenatal exposure to the environmental obesogen tributyltin predisposes multipotent stem cells to become adipocytes. Molecular Endocrinology. 2010;24(3):526–539. (Key experimental evidence for TBT as an obesogen — PubMed search.)
- Agency for Toxic Substances and Disease Registry (ATSDR). Toxicological Profile for Tin and Tin Compounds. U.S. Department of Health and Human Services. ATSDR ToxProfile (PDF).
- World Health Organization / International Programme on Chemical Safety (IPCS). Environmental Health Criteria 116: Tributyltin Compounds. WHO/IPCS INCHEM.
- International Maritime Organization (IMO). International Convention on the Control of Harmful Anti-fouling Systems on Ships (AFS Convention; in force 2008). IMO Anti-fouling Systems.
Connections
- All Toxic Minerals
- Heavy Metals
- Lead
- Mercury
- Arsenic
- Cadmium
- Aluminum
- Manganism
- Parkinson's Disease
- Selenium
- Zinc
- Iron
- Lab Tests
- All Minerals