Nickel Toxicity: Contact Dermatitis, Occupational Exposure, and Carcinogenicity
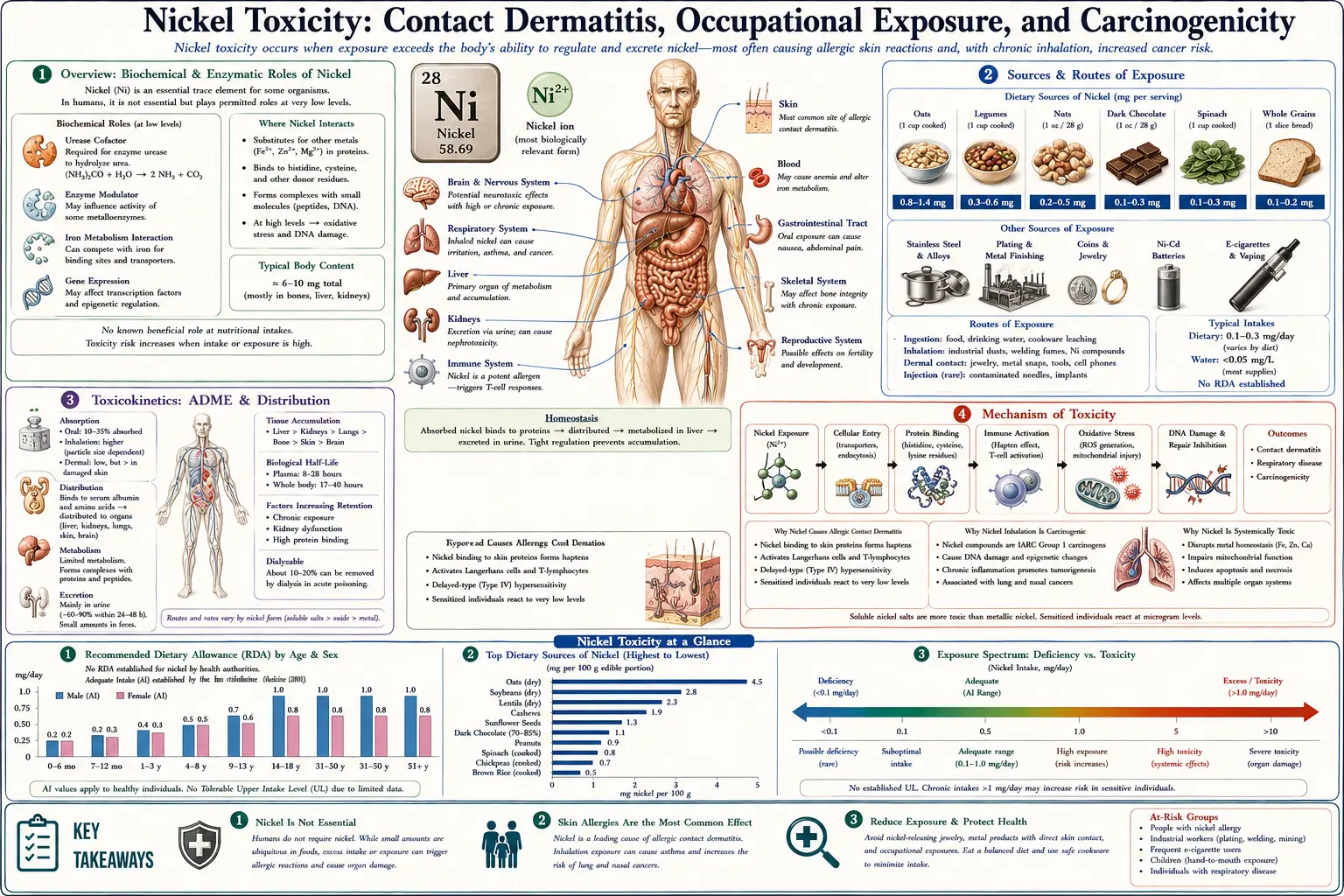
Table of Contents
- Overview
- Sources & Routes of Exposure
- Toxicokinetics
- Mechanism of Toxicity
- Symptoms & Health Effects
- Diagnosis & Laboratory Testing
- Treatment & Management
- Prevention & Risk Reduction
- Related Topics
- Key Research Papers
- Connections
- Featured Videos
1. Overview
Nickel (Ni) is a hard, silvery-white transition metal that is everywhere in modern life — in stainless steel, coins, jewelry, eyeglass frames, zippers, belt buckles, smartphones, orthodontic braces, and surgical implants. It is the workhorse of the alloy industry. Yet this same ubiquity makes nickel the single most important cause of allergic skin disease worldwide: nickel is the world's most common cause of allergic contact dermatitis, sensitizing an estimated 8–19% of the general population in surveyed countries. For most people, the harm from nickel is not poisoning in the classical sense but an immune reaction — an itchy, blistering rash that appears wherever metal touches skin.
Nickel toxicity therefore wears two very different faces. The first is immunological: a delayed (type IV) hypersensitivity allergy that affects the public at large and turns an everyday metal into a source of chronic, recurring dermatitis. The second is occupational and chemical: among workers in nickel refining, plating, welding, and battery manufacture, inhaled nickel compounds raise the risk of lung and nasal cancers, and one specific compound — nickel carbonyl — is among the most acutely lethal industrial gases known. Understanding nickel means keeping both stories in view at once.
A point that surprises many readers: nickel is sometimes described as an ultratrace element. Trace amounts are present in human tissue and nickel is essential for certain bacteria and plants (it sits at the active site of the enzyme urease). But no firmly established human requirement for nickel exists, no recommended dietary allowance has been set, and no deficiency disease has ever been demonstrated in people. In practical terms, nickel is best regarded as a contaminant and an allergen rather than a nutrient. The U.S. Institute of Medicine set only a tolerable upper intake level (1 mg/day for adults as soluble nickel salts), not a recommended intake.
This page focuses on what nickel does to the human body: how a metal that rarely poisons through the gut becomes the leading trigger of skin allergy, how sensitized people can react to nickel in their food (systemic nickel allergy syndrome), how refinery workers face cancer risk and the rare catastrophe of nickel carbonyl exposure, and how clinicians diagnose and manage each of these problems.
2. Sources & Routes of Exposure
Nickel reaches the body by three routes — through the skin (the dominant route for allergy), by inhalation (the dominant route for cancer risk and acute poisoning), and by ingestion (the route relevant to systemic reactions in already-sensitized people). The source that matters most depends on which route you are considering.
Consumer Items That Touch the Skin
Skin contact with nickel-releasing objects is what sensitizes the population and what triggers flares afterward. The classic offenders include:
- Jewelry and piercings — earrings, necklaces, rings, and especially body and ear piercings placed through broken skin, which is the most efficient way to become sensitized. Cheap costume jewelry and white-gold alloys are frequent culprits.
- Fasteners and clothing hardware — belt buckles, jeans studs and buttons, bra hooks, zippers, and snap fasteners produce the recognizable rashes at the navel, waistline, and beneath bra straps.
- Eyeglass frames — metal frames and nose pads cause dermatitis on the bridge of the nose and behind the ears.
- Coins, keys, and tools — handled occupationally (cashiers, locksmiths) or recreationally; many coins are nickel-bearing alloys.
- Mobile phones and electronics — nickel in phone casings, buttons, and connectors can cause facial and hand dermatitis. The European Union explicitly extended its Nickel Directive to mobile phones after cases were documented.
- Orthodontic and medical devices — braces, dental crowns, orthopedic and cardiovascular implants, and surgical clips can release nickel internally, occasionally provoking reactions discussed below.
Occupational Inhalation
Workplace exposure to airborne nickel is the source that drives the serious systemic risks. High-exposure jobs include nickel mining and refining, electroplating, stainless-steel and alloy production, welding and grinding of nickel-bearing metals, nickel-cadmium battery manufacture, and catalyst and pigment production. The hazard depends heavily on the chemical form: soluble nickel salts (sulfate, chloride), less-soluble sulfidic and oxidic nickel (subsulfide, nickel oxide), and metallic nickel each behave differently in the lung. The U.S. National Institute for Occupational Safety and Health (NIOSH) and OSHA set permissible airborne limits, and the IARC classifications hinge on these occupational cohorts.
Nickel Carbonyl — A Special Industrial Hazard
Nickel carbonyl, Ni(CO)4, deserves separate mention because it is unlike any consumer exposure. It is a colorless, volatile liquid (boiling at about 43 °C) that readily forms a heavy, intensely toxic gas, used historically in the Mond process for refining ultra-pure nickel and in some catalytic and vapor-deposition chemistry. It is one of the most acutely poisonous nickel forms known and has caused refinery deaths. Its toxicology is covered under Mechanism and Symptoms below.
Dietary Nickel
Food is a minor route for the general population but is central to systemic nickel allergy syndrome. Average dietary intake is roughly 100–300 µg of nickel per day. Foods particularly rich in nickel include legumes (beans, lentils, peas, soybeans), nuts, cocoa and chocolate, oats and whole grains, and many canned foods (acidic foods can leach nickel from cans and from stainless-steel cookware). Drinking water and the first run of water from nickel-plated taps can also contribute. For most people this dietary nickel is harmless; for the nickel-sensitized minority it can sustain a stubborn dermatitis.
3. Toxicokinetics
Toxicokinetics describes what the body does to a substance — how it is absorbed, distributed, and eliminated. Nickel's kinetics explain why oral nickel rarely poisons, why the skin and lungs are the vulnerable interfaces, and why blood and urine nickel are used to gauge recent exposure.
Absorption
Gastrointestinal absorption of nickel is limited and variable — roughly 1–10% of an ingested dose, and lower still when nickel is taken with food because it binds to dietary components. Absorption rises sharply when soluble nickel is taken on an empty stomach with water, which is why human experimental studies of systemic reactions use fasting nickel challenges. By contrast, inhaled nickel can be deposited and partly retained in the respiratory tract, and the fraction reaching the bloodstream depends on particle size and solubility: soluble salts are absorbed more readily, while insoluble particles can lodge in lung tissue for long periods. Dermal absorption of intact skin is low, but nickel ions penetrate enough to engage the immune system, and penetration increases through damaged, sweaty, or occluded skin.
Distribution
Once in blood, nickel travels bound largely to albumin, with smaller amounts on the nickel-transport protein and free ion. It distributes to kidney, lung, liver, and other tissues; the kidney typically shows the highest concentrations among soft tissues because it is the main excretory organ. Nickel can cross the placenta, and small amounts appear in breast milk.
Elimination
Absorbed nickel is cleared predominantly by the kidneys into urine, with a biological half-life on the order of a day or two for the soluble fraction — so blood and urine nickel reflect relatively recent exposure, not lifetime body burden. Unabsorbed nickel simply passes in the feces. Sweat is a minor but real route; sweat nickel concentrations can actually exceed those in urine, which matters for skin exposure because perspiration helps liberate nickel ions from metal objects. Because nickel does not bioaccumulate over decades the way cadmium does, removing the source generally allows nickel levels to fall.
4. Mechanism of Toxicity
Nickel injures the body through three largely separate mechanisms — an immune mechanism behind contact allergy, a respiratory-poison mechanism behind nickel carbonyl, and a genotoxic/epigenetic mechanism behind cancer. They share a metal but little else.
Type IV (Delayed) Hypersensitivity — the Allergy Mechanism
Allergic contact dermatitis to nickel is a T-cell-mediated, delayed-type (type IV) hypersensitivity reaction, not an antibody (IgE) allergy like hay fever. It unfolds in two phases. In the sensitization phase, nickel ions (Ni2+) released from an object penetrate the skin, bind to the body's own proteins, and are taken up by skin immune cells (Langerhans and dendritic cells) that present the nickel-altered proteins to T lymphocytes in the lymph nodes. This generates a population of nickel-specific memory T cells over one to three weeks. In the elicitation phase, any subsequent skin contact with nickel recruits these memory T cells back to the site, where they release inflammatory cytokines that produce the characteristic eczematous rash 12–72 hours later. Nickel is an unusually potent sensitizer in part because Ni2+ can also directly trigger an innate immune receptor (Toll-like receptor 4) on human cells, amplifying inflammation.
Nickel Carbonyl — Pulmonary Toxin and Oxidative Injury
Nickel carbonyl is dangerous because of how it behaves once inhaled. As a lipid-soluble, uncharged molecule it readily crosses cell membranes and reaches deep lung tissue, where it decomposes to release nickel and carbon monoxide. The liberated nickel damages alveolar (lung air-sac) cells, generates reactive oxygen species and oxidative stress, disrupts cellular enzymes, and provokes intense inflammation and leakage of fluid into the lungs. The result is a chemical pneumonitis and non-cardiogenic pulmonary edema that can develop hours to days after exposure. This delayed, fluid-filled lung injury is what makes nickel carbonyl lethal even when the initial symptoms seem mild.
Carcinogenesis — Genotoxic and Epigenetic Mechanisms
Nickel compounds are carcinogenic largely through indirect genetic and epigenetic damage rather than by directly mutating DNA in the way classic chemical mutagens do. Inside the cell, nickel ions generate reactive oxygen species and interfere with DNA-repair enzymes, allowing oxidative DNA damage to persist. Nickel also silences tumor-suppressor genes by epigenetic means — it alters DNA methylation and histone modifications, switching off protective genes without changing the DNA sequence. A further key mechanism is that nickel mimics low-oxygen conditions: it stabilizes hypoxia-inducible factor (HIF) and activates hypoxia-response pathways that favor abnormal cell survival and proliferation. Because insoluble nickel particles can be engulfed by cells and slowly release nickel ions next to the nucleus, they deliver a sustained intracellular dose, which helps explain why less-soluble nickel compounds are strongly linked to respiratory cancers.
5. Symptoms & Health Effects
Because nickel acts through several mechanisms, its symptoms span the skin, the airways, the gut, and (over years of occupational exposure) the development of cancer. It is useful to separate acute effects (appearing within minutes to days) from chronic effects (developing over months to decades), and to organize them by organ system.
Skin (Allergic Contact Dermatitis)
The most common health effect of nickel is dermatitis. The acute rash is red, intensely itchy, and often blistering or weeping, appearing precisely where nickel touched the skin — earlobes from earrings, the navel and waist from jeans studs and belt buckles, wrists from watch backs and bracelets, the nose bridge from eyeglass frames. With repeated or continuous exposure the skin becomes chronically thickened, scaly, cracked, and darkened (lichenified). Some people develop secondary eruptions at sites distant from the original contact (an "id" reaction) and a pattern of recurring hand eczema, which can be occupationally disabling for hairdressers, caterers, metalworkers, and healthcare staff who handle nickel-bearing tools.
Systemic Nickel Allergy Syndrome (SNAS)
In a subset of already nickel-sensitized people, swallowed dietary nickel can trigger reactions far from the gut. This systemic contact dermatitis can take the form of widespread eczema, a symmetric rash of the flexures and buttocks (the so-called "baboon syndrome"), flare-ups of previous patch-test sites, and dyshidrotic (pompholyx) blistering of the hands and feet. Many patients also report gastrointestinal symptoms — bloating, abdominal pain, nausea, and altered bowel habit — and nonspecific systemic complaints such as headache and fatigue, a cluster increasingly labeled systemic nickel allergy syndrome. Controlled oral-challenge studies confirm that a sufficiently large dose of soluble nickel can provoke these reactions in sensitized individuals, and that a low-nickel diet can reduce them.
Implant-Related Reactions
Nickel released from orthopedic, dental, or cardiovascular implants occasionally causes localized eczema over the device, persistent dermatitis, or — debated and far less common — local tissue reactions around metal-on-metal joint replacements. Most people with nickel allergy tolerate stainless-steel implants well, but documented sensitivity is a reason clinicians may choose nickel-free or titanium hardware.
Acute Nickel Carbonyl Poisoning — a Biphasic Illness
Acute inhalation of nickel carbonyl produces a classic two-stage (biphasic) illness, and recognizing the pattern is lifesaving. The immediate phase, within minutes to hours, brings headache, dizziness, nausea, vomiting, and chest tightness; these symptoms often ease if the person leaves the contaminated area, creating a dangerous false reassurance. A delayed phase then develops roughly 12 hours to 5 days later, dominated by severe chemical pneumonitis and pulmonary edema — worsening cough, breathlessness, fever, and chest pain that can progress to respiratory failure and death. The large clinical series of nickel carbonyl poisoning describe exactly this delayed pulmonary catastrophe, with severity graded by symptoms and chest findings. Survivors may have prolonged respiratory and neurological complaints.
Respiratory Tract (Chronic Occupational Effects)
Chronic inhalation of nickel dust and fumes is associated with a range of non-malignant airway effects, including chronic rhinitis, sinusitis, nasal septal damage (including perforation), and occupational asthma ("nickel asthma"), the latter being a sensitizer-induced asthma in susceptible workers. These conditions overlap with, but are distinct from, the cancer risk.
Cancer (Lung and Nasal/Sinus)
The most serious chronic effect is cancer. Long-term occupational inhalation of certain nickel compounds increases the risk of cancers of the lung and of the nasal cavity and paranasal sinuses, as documented in refinery and smelter cohorts since the mid-20th century. On this evidence, the International Agency for Research on Cancer classifies nickel compounds as Group 1 (carcinogenic to humans), while metallic nickel is classified as Group 2B (possibly carcinogenic to humans). The risk is an occupational, inhalation-driven phenomenon; wearing nickel jewelry or eating nickel-containing food does not carry this cancer risk.
6. Diagnosis & Laboratory Testing
There is no single "nickel test." Diagnosis is matched to the problem: skin patch testing identifies the allergy, a chemical spot test identifies which objects release nickel, and blood and urine nickel measure systemic exposure. Each answers a different question.
Patch Testing — Confirming Nickel Allergy
The gold standard for diagnosing nickel contact allergy is the epicutaneous patch test. Standardized test chambers loaded with nickel sulfate (typically 5% in petrolatum) are taped to the upper back. The patches are removed after 48 hours and the skin is read by a clinician at 48 hours and again at 72–96 hours (a delayed reading is important because nickel reactions can develop late). A positive reaction shows graded redness, papules, or vesicles confined to the test site, reflecting the underlying delayed-type hypersensitivity. Patch testing distinguishes true allergy from irritation and from other eczemas, and nickel is the most frequently positive allergen in baseline patch-test series around the world.
Dimethylglyoxime (DMG) Spot Test — Testing the Object, Not the Patient
A simple, inexpensive chemical test lets patients and clinicians find out whether a specific object releases enough nickel to cause trouble. A cotton swab is moistened with the dimethylglyoxime (DMG) reagent (with ammonia) and rubbed on the metal surface; if free nickel is being released, the swab turns a characteristic pink/strawberry-red color. The DMG test is widely used to screen jewelry, watches, fasteners, tools, and phones, and it underpins regulatory enforcement of nickel-release limits. It is a screening test — a negative result does not absolutely exclude very low nickel release, and the test is for identifying problematic items, not for diagnosing the allergy itself.
Blood and Urine Nickel — Measuring Systemic Exposure
When the question is recent systemic exposure (occupational monitoring, suspected acute poisoning), nickel is measured in blood/serum and urine, usually by inductively coupled plasma mass spectrometry. Reference (background) concentrations in unexposed people are low — generally on the order of a few micrograms per liter (µg/L) or less in both serum and urine, with urine often reported as nickel per gram of creatinine to correct for dilution. Because nickel clears within days, these values track recent exposure rather than long-term burden, and markedly elevated levels support occupational over-exposure or acute nickel carbonyl poisoning. Laboratory reference ranges vary, so results must be interpreted against the testing laboratory's own values. Blood and urine nickel are not useful for diagnosing contact allergy — that is what patch testing is for.
Putting the Tests Together
In practice, a person with an itchy rash under jewelry is evaluated with a patch test to confirm nickel allergy and may use a DMG swab to identify the offending items; a refinery worker is followed with periodic urine nickel as a biomarker of exposure; and a collapsed worker after a refinery accident has blood and urine nickel drawn urgently to confirm and grade nickel carbonyl poisoning while treatment begins.
7. Treatment & Management
Treatment depends entirely on which form of nickel toxicity is present. For the common problem — contact dermatitis — the cornerstone is avoidance. For the rare emergency — nickel carbonyl poisoning — the priorities are decontamination, oxygen, intensive supportive care, and chelation.
Allergic Contact Dermatitis: Avoidance Is the Cornerstone
The single most effective treatment for nickel dermatitis is removing the source. Practical measures include switching to nickel-free or hypoallergenic jewelry (surgical-grade stainless steel, titanium, niobium, plastic, or coated metals), choosing nickel-free eyeglass frames and watch backs, and creating a barrier between skin and metal — clear nail polish or a coating on the backs of buckles and studs, plastic covers on snaps, fabric guards. The DMG spot test helps patients pre-screen new purchases. Sweat increases nickel release, so keeping skin dry and limiting prolonged metal contact in hot conditions helps.
For active rash, the medical mainstays are topical corticosteroids to calm the inflammation, with topical calcineurin inhibitors as steroid-sparing options for sensitive areas (face, eyelids), emollients to repair the skin barrier, and short courses of systemic steroids reserved for severe, widespread flares. Antihistamines may relieve itch. Secondary bacterial infection of excoriated skin is treated as needed.
Systemic Nickel Allergy Syndrome: The Low-Nickel Diet
For patients whose dermatitis or systemic symptoms are driven by dietary nickel, a low-nickel diet can reduce flares. This means limiting the high-nickel foods named earlier — legumes, nuts, cocoa and chocolate, oats and whole grains, soy, and canned and acidic foods stored in metal — and avoiding the first draw of water from the tap and prolonged cooking of acidic foods in stainless steel. Structured low-nickel diet scoring systems have been developed and tested to make the approach practical and measurable. The diet is restrictive and best undertaken with dietitian guidance to avoid nutritional gaps; it is used selectively, in confirmed nickel-sensitized patients whose symptoms correlate with intake, rather than broadly.
Acute Nickel Carbonyl Poisoning: A Medical Emergency
Nickel carbonyl poisoning is managed in an intensive-care setting. Immediate steps are removal from the contaminated atmosphere and decontamination, followed by high-flow oxygen and close observation, because the dangerous pulmonary edema can be delayed by one to five days. Care is largely supportive — supplemental oxygen, mechanical ventilation if respiratory failure develops, and treatment of pulmonary edema. Chelation is used to bind and accelerate elimination of nickel, with sodium diethyldithiocarbamate being the historical agent of choice; disulfiram (which is metabolized to diethyldithiocarbamate) has also been used. Because nickel carbonyl also releases carbon monoxide, carboxyhemoglobin is checked and treated. Urine nickel measurement helps gauge severity and guide the intensity and duration of chelation. Prompt recognition of the biphasic pattern, and not being lulled by the temporary improvement of the early phase, is the most important determinant of survival.
8. Prevention & Risk Reduction
Most nickel disease is preventable. Public-health regulation has measurably reduced allergy in the population, and occupational controls protect workers from cancer and acute poisoning.
Regulating Nickel Release from Consumer Products
The most important population-level intervention has been limiting how much nickel everyday objects may release onto the skin. The European Union Nickel Directive set limits on nickel release from items in prolonged skin contact (such as jewelry, watches, and fasteners) and on items inserted into pierced skin. Surveillance studies credit such regulation with falling rates of nickel sensitization in younger people in regulated countries, and the rules were later interpreted to cover newer items such as mobile phones. For individuals, the lesson is concrete: get piercings done with documented nickel-free posts, and favor regulated or certified nickel-free products.
Personal Strategies for the Nickel-Allergic
- Carry and use a DMG test kit to screen jewelry, belt buckles, tools, and electronics before buying or wearing them.
- Choose titanium, surgical stainless steel, niobium, sterling silver, platinum, or solid high-karat gold for items worn against the skin, and plastic or coated alternatives for fasteners.
- Coat the inside of buckles, jeans studs, and snap fasteners with clear lacquer or barrier products, and reapply as the coating wears.
- Keep skin dry where it contacts metal, since sweat liberates nickel; remove metal jewelry during heavy exercise.
- Inform surgeons, orthodontists, and dentists of a known nickel allergy so nickel-free hardware can be selected when appropriate.
Occupational Controls
In nickel-using industries, prevention follows the standard hierarchy of controls: substitution and process enclosure, local exhaust ventilation to capture dust and fumes at the source, respiratory protection where airborne nickel cannot be otherwise controlled, and biological monitoring with periodic urine nickel to detect over-exposure. Strict engineering controls, leak detection, and emergency procedures are essential wherever nickel carbonyl is generated, given its lethality and delayed effects. Workers handling nickel-bearing metals should also be alert to occupational hand dermatitis and asthma and report early symptoms. Agencies such as NIOSH, OSHA, and ATSDR publish exposure limits and guidance underpinning these programs.
9. Related Topics
- Toxic Minerals — the parent overview of toxic and heavy-metal exposures, where nickel sits alongside the other elements covered here.
- Heavy Metals — general principles of metal toxicity, biomonitoring, and chelation that frame nickel's behavior.
- Cadmium — a Group 1 carcinogen and the metal historically paired with nickel in NiCd batteries; useful contrast in toxicokinetics.
- Hexavalent Chromium — another occupational respiratory carcinogen and a frequent co-allergen with nickel in metal-contact dermatitis.
- Beryllium — a metal whose immune-mediated lung disease parallels nickel's hypersensitivity biology.
- Copper Toxicity — a related transition-metal toxicity for comparison of mechanisms and clinical effects.
- Zinc — the essential metal nickel can compete with and a key cofactor displaced in some nickel mechanisms.
- Copper — an essential trace metal that contrasts with nickel's lack of an established human requirement.
- Iron — shares divalent-metal transport pathways relevant to how the gut handles trace metals.
- Pulmonology — lung disease overview covering occupational pneumonitis, asthma, and the respiratory cancers linked to inhaled nickel.
- Lab Tests — background on the blood, urine, and patch testing used to diagnose nickel exposure and allergy.
- All Minerals — the full minerals section, essential and toxic.
10. Key Research Papers
- Ahlström MG, Thyssen JP, Wennervaldt M, Menné T, Johansen JD. Nickel allergy and allergic contact dermatitis: A clinical review of immunology, epidemiology, exposure, and treatment. Contact Dermatitis. 2019;81(4):227–241. doi:10.1111/cod.13327
- Thyssen JP, Linneberg A, Menné T, Johansen JD. The epidemiology of contact allergy in the general population — prevalence and main findings. Contact Dermatitis. 2007;57(5):287–299. doi:10.1111/j.1600-0536.2007.01220.x
- Fors R, Persson M, Bergström E, Stenlund H, Stymne B, Stenberg B. Nickel allergy in relation to piercing and orthodontic appliances — a population study. Contact Dermatitis. 2012;67(6):342–350. doi:10.1111/j.1600-0536.2012.02097.x
- Jensen CS, Menné T, Johansen JD. Nickel-elicited systemic contact dermatitis. Contact Dermatitis. 2003;49(3):124–132. doi:10.1034/j.1600-0536.2003.00017.x
- Veien NK, Hattel T, Laurberg G. Low nickel diet: an open, prospective trial. Contact Dermatitis. 1990;22(5):282–285. doi:10.1111/j.1600-0536.1990.tb01617.x
- Mislankar M, Zirwas MJ. Low-nickel diet scoring system for systemic nickel allergy. Dermatitis. 2013;24(4):190–195. doi:10.1097/der.0b013e3182937e81
- Thyssen JP, Gawkrodger DJ, White IR, Julander A, Menné T, Lidén C. Coin exposure may cause allergic nickel dermatitis; mobile phones are now covered by the European Union Nickel Directive. Contact Dermatitis. 2009;61(1):56–58. doi:10.1111/j.1600-0536.2009.01551.x
- Hallab N, Merritt K, Jacobs JJ. Metal allergy and second-generation metal-on-metal arthroplasties. Contact Dermatitis. 2012;66(6):373–383. doi:10.1111/j.1600-0536.2011.01970.x
- Shi ZC. Acute nickel carbonyl poisoning: a report of 179 cases. British Journal of Industrial Medicine (Occupational and Environmental Medicine). 1986;43(6):422–424. doi:10.1136/oem.43.6.422
- Sunderman FW, Kincaid JF. Nickel poisoning. II. Studies on patients suffering from acute exposure to vapors of nickel carbonyl. Journal of the American Medical Association. 1954;155(10):889–894. doi:10.1001/jama.1954.03690280013003
- Cheng J, et al. Research on the cell and molecule mechanism of acute toxicity of nickel carbonyl in rats. Toxicology Letters. 2010;196(Suppl):S253. doi:10.1016/j.toxlet.2010.03.940
- Pedersen E, Høgetveit AC, Andersen A. Lung cancer in workers in a nickel refinery. British Journal of Industrial Medicine (Occupational and Environmental Medicine). 1978;35(2):109–116. doi:10.1136/oem.35.2.109
- Agency for Toxic Substances and Disease Registry (ATSDR). Toxicological Profile for Nickel. U.S. Department of Health and Human Services, Public Health Service. atsdr.cdc.gov/toxprofiles/tp15.pdf
- International Agency for Research on Cancer (IARC). Nickel and nickel compounds. In: IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, Vol. 100C. Lyon: IARC. IARC Monograph 100C
- National Institute for Occupational Safety and Health (NIOSH). Nickel — NIOSH Pocket Guide to Chemical Hazards. U.S. Centers for Disease Control and Prevention. cdc.gov/niosh/npg/npgd0452.html
Connections
- All Toxic Minerals
- Heavy Metals
- Cadmium
- Hexavalent Chromium
- Beryllium
- Copper Toxicity
- Zinc
- Copper
- Iron
- Pulmonology
- Lab Tests
- All Minerals
- Contact Dermatitis — the skin disease nickel causes more often than any other allergen.