Beryllium Toxicity and Chronic Beryllium Disease (Berylliosis)
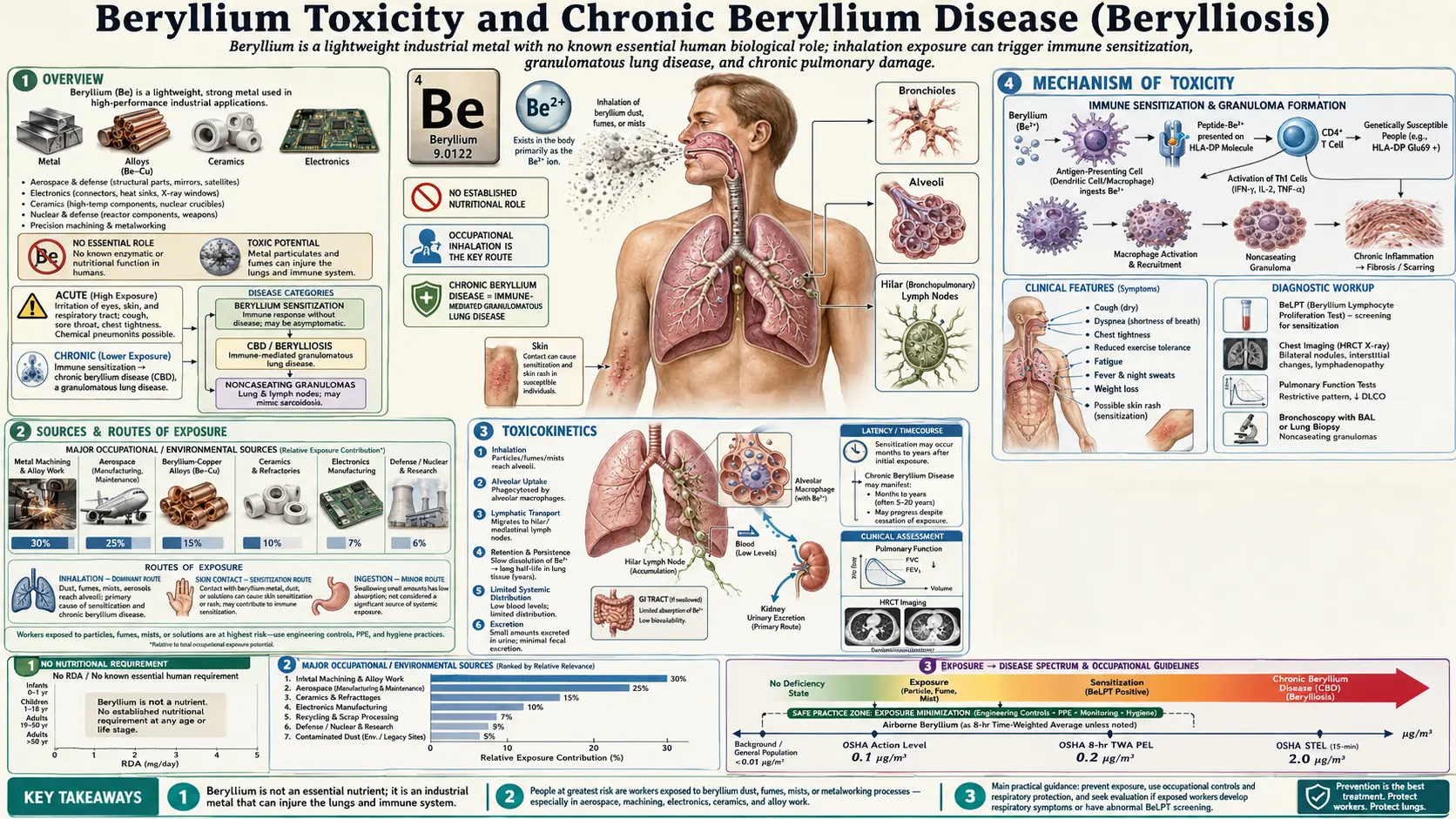
Table of Contents
- Overview
- Sources & Routes of Exposure
- Toxicokinetics
- Mechanism of Toxicity
- Symptoms & Health Effects
- Diagnosis & Laboratory Testing
- Treatment & Management
- Prevention & Risk Reduction
- Related Topics
- Key Research Papers
- Connections
- Featured Videos
1. Overview
Beryllium is a lightweight, exceptionally stiff steel-gray metal (symbol Be, atomic number 4). Pound for pound it is stronger than steel, conducts heat well, is transparent to X-rays, and does not spark when struck — properties that make it valuable in aerospace, nuclear weapons, electronics, and precision instruments. Those same uses are why beryllium is also one of the most important occupational lung toxicants known. Unlike lead, mercury, or cadmium, beryllium does not poison the body as a general metabolic toxin. Instead, in susceptible people it provokes a misdirected immune response against the metal itself, and that immune reaction — not the metal’s chemistry alone — is what damages the lungs.
Two distinct diseases
It is essential to understand that "beryllium disease" actually refers to two very different conditions that share a name but little else:
- Acute beryllium disease (ABD). A chemical pneumonitis — a direct, dose-related chemical burn of the airways and lung tissue — caused by inhaling high concentrations of soluble beryllium compounds. It behaves like an industrial inhalation injury, comes on within hours to weeks, and can be severe or fatal. It has become rare in modern industry because the airborne concentrations required to cause it are now controlled by exposure limits.
- Chronic beryllium disease (CBD), also called berylliosis. A delayed, immune-mediated granulomatous disease of the lungs that can appear months, years, or even decades after exposure — and after exposures far too low to ever cause acute disease. CBD is the dominant clinical problem today and is the central focus of this page.
Why CBD matters and why it is so often missed
CBD is a textbook example of how a tiny amount of a substance can cause serious chronic illness in a susceptible minority. Crucially, CBD is frequently mistaken for sarcoidosis, a more common granulomatous lung disease of unknown cause; the two can be indistinguishable on a chest scan and under the microscope. The decisive difference is a specialized blood (or lung-fluid) immune test, the beryllium lymphocyte proliferation test (BeLPT), combined with a careful history of beryllium exposure. Because exposure histories are easy to overlook and the test is not routine, an unknown number of people carrying a diagnosis of "sarcoidosis" almost certainly have undiagnosed CBD. Beryllium is also classified by the International Agency for Research on Cancer (IARC) as a Group 1 human carcinogen for lung cancer, adding a second long-term concern beyond CBD.
2. Sources & Routes of Exposure
Who is exposed
Beryllium exposure is overwhelmingly occupational. The metal and its alloys are used wherever stiffness, light weight, thermal stability, or non-sparking behavior is needed. The major exposed groups include:
- Aerospace and defense: structural components, gyroscopes, satellite and aircraft parts, and guidance systems.
- Nuclear weapons and reactors: beryllium is a neutron reflector and moderator; legacy U.S. Department of Energy weapons sites are among the most studied sources of disease.
- Electronics and semiconductors: heat sinks, connectors, and high-reliability springs, very often made of beryllium-copper alloy (typically about 2% beryllium).
- Telecommunications and precision instruments: relays, switches, and connectors that must flex millions of times without fatigue.
- Dental laboratories: some older nickel- and cobalt-chromium casting alloys contained beryllium; grinding and polishing dental appliances can generate fine dust.
- Metal machining, foundry work, and recycling/scrap: any cutting, grinding, sanding, welding, or melting of beryllium-containing materials can release respirable particles. Recycling of electronics and alloys is an increasingly recognized exposure.
The route that matters: inhalation
The hazard is almost entirely about breathing beryllium in. The dangerous forms are fine respirable particles and fumes — particles small enough (roughly a few micrometers and below) to bypass the upper airway defenses and deposit deep in the gas-exchange regions of the lung. A solid block of beryllium on a workbench is essentially harmless; the same metal turned into airborne dust by a grinder is the threat. Particle size and surface area appear to matter as much as the total mass, which is part of why even very low average air concentrations have caused sensitization. Skin contact can also induce sensitization in some workers, particularly through breaks in the skin, and is one reason modern programs address both air and surface (and skin) contamination.
Take-home and bystander exposure
Beryllium dust carried home on work clothes, shoes, skin, and in vehicles has caused disease in family members and in workers whose jobs were near — but not directly involving — beryllium operations. Studies at construction trades on nuclear sites, and clusters traced to unexpected sources such as beryllium-contaminated concrete dust, show that "non-beryllium workers" sharing a workplace can be sensitized. There is no meaningful dietary source of toxic beryllium exposure; trace amounts in food and water are poorly absorbed and are not the public-health issue.
3. Toxicokinetics
Absorption and distribution
How beryllium behaves in the body depends heavily on its chemical form and on the route of entry. Inhaled particles deposit in the airways and alveoli, where the lung’s scavenging cells (alveolar macrophages) engulf them. Soluble beryllium compounds are cleared faster; insoluble or poorly soluble forms (such as beryllium oxide and beryllium metal) persist for long periods, sometimes years, acting as a continuous local stimulus to the immune system. Absorption from the gut is very low — only a small percentage of an ingested dose crosses the intestinal wall — which is why swallowing beryllium is far less concerning than breathing it.
Retention, storage, and elimination
Beryllium that does enter the circulation distributes to the skeleton, liver, and other tissues, with bone serving as the principal long-term reservoir. Elimination is slow and occurs mainly through the urine. Because the metal that drives chronic disease tends to be sequestered in the lung and lymph nodes rather than freely circulating, blood and urine beryllium levels are not reliable indicators of an individual’s body burden or of CBD. This is a critical and often misunderstood point: for most heavy metals, a blood or urine level estimates exposure and risk, but for chronic beryllium disease the relevant "dose" is immunological, not the milligrams measured in a body fluid.
Why dose and disease do not line up
A consistent and humbling finding across many cohorts is the weak relationship between measured cumulative exposure and who actually develops sensitization or CBD. Some heavily exposed workers never sensitize; some lightly exposed ones do. This breakdown of a simple dose-response is the signature of an immunologic (hypersensitivity) disease rather than a classic toxicologic one, and it shifts the explanation from the metal’s kinetics to the individual’s immune genetics, discussed next.
4. Mechanism of Toxicity
A type IV (delayed) hypersensitivity
Chronic beryllium disease is a cell-mediated, delayed-type (type IV) hypersensitivity reaction — the same broad immune category as poison-ivy dermatitis or the tuberculin skin test, but directed at a metal and located in the lung. The damage is done not by the metal’s chemical aggressiveness but by a sustained, antigen-specific attack mounted by the body’s own T-lymphocytes.
Beryllium as a hapten and the CD4+ T-cell response
Beryllium is far too small a molecule for the immune system to "see" on its own. It acts as a hapten: a beryllium ion lodges within the antigen-binding groove of certain HLA class II molecules (specifically HLA-DP variants) displayed on antigen-presenting cells. By altering the shape and chemistry of the peptides held in that groove, beryllium effectively creates a neoantigen — a "new" target the immune system has never tolerated. Beryllium-specific CD4+ helper T cells recognize this complex, become activated, proliferate, and release inflammatory signaling molecules (cytokines such as interferon-gamma and tumor necrosis factor). These signals recruit and corral macrophages into tight, organized clusters.
Granuloma formation
The hallmark lesion of CBD is the noncaseating granuloma — a compact ball of immune cells (macrophages, multinucleated giant cells, and surrounding lymphocytes) walling off the persistent beryllium. "Noncaseating" means there is no cheese-like dead tissue at the center, which is exactly what is also seen in sarcoidosis — hence the diagnostic confusion. Over time, accumulating granulomas and the scarring (fibrosis) they leave behind stiffen the lung, thicken the gas-exchange membrane, and progressively impair the transfer of oxygen into the blood.
Genetic susceptibility: HLA-DPB1 Glu69
Why do only some exposed people develop disease? A major part of the answer is inherited. A landmark 1993 study identified a specific molecular feature — a glutamic-acid residue at position 69 of the HLA-DPβ1 chain (the "Glu69" marker) — that is strongly over-represented in people with chronic beryllium disease. This negatively charged amino acid sits in the part of the HLA molecule that grips the antigen, and it appears to favor the binding of beryllium and the formation of the neoantigen. Carrying a Glu69-positive HLA-DPB1 allele substantially increases the risk of sensitization and CBD, although it is neither necessary nor sufficient on its own — exposure, particle characteristics, and other genetic and immune factors all contribute. Research using HLA-DP2 transgenic mouse models and human T-cell studies has since mapped the beryllium-specific response in fine detail and is exploring regulatory T cells as a brake on the granulomatous inflammation.
5. Symptoms & Health Effects
Acute beryllium disease (chemical pneumonitis)
Acute disease follows intense, short-term inhalation of (usually soluble) beryllium. It is essentially a chemical injury to the respiratory tract and may include:
- Irritation of the nose, throat, and airways; cough; and a burning or raw sensation in the chest.
- Shortness of breath, sometimes severe, developing over hours to a few weeks.
- Tracheobronchitis and, in the most severe cases, chemical pneumonitis with widespread inflammation of the lung tissue and dangerously low blood oxygen.
- Skin and eye irritation, and (with skin contact) contact dermatitis or, if metal enters a wound, persistent skin granulomas and slow-healing ulcers.
Acute disease can be life-threatening but, with removal from exposure and supportive care, may resolve — though some survivors later go on to develop chronic beryllium disease.
Beryllium sensitization versus disease
A pivotal concept in chronic beryllium illness is the distinction between sensitization and disease:
- Beryllium sensitization (BeS) means the immune system has developed beryllium-specific T cells — an abnormal immune response detectable by laboratory testing — but there is no granulomatous lung disease yet. A sensitized person typically feels well and has normal imaging and lung function. Sensitization is, in effect, the immunologic foothold that can precede disease.
- Chronic beryllium disease (CBD) means sensitization plus demonstrable granulomatous inflammation in the lung. CBD is the actual illness.
Sensitization is not harmless background noise: longitudinal follow-up shows that a meaningful fraction of sensitized workers progress to CBD over time, on the order of several percent per year in some cohorts. That is why finding sensitization triggers ongoing medical surveillance rather than reassurance.
Chronic beryllium disease (berylliosis)
CBD is typically insidious. Many people have no symptoms for years while granulomas quietly accumulate, and disease may first surface as an abnormal finding on screening. When symptoms appear, they reflect progressive lung impairment and commonly include:
- Breathlessness on exertion (dyspnea) — usually the earliest and most prominent complaint, gradually worsening over months to years.
- A persistent dry cough and reduced exercise tolerance.
- Fatigue, low-grade fevers, night sweats, and unintended weight loss — constitutional symptoms that, again, overlap heavily with sarcoidosis.
- Chest discomfort and, as disease advances, low blood oxygen and finger clubbing.
In advanced CBD, accumulating fibrosis can lead to respiratory failure, pulmonary hypertension, and strain on the right side of the heart (cor pulmonale). Although the lungs dominate the clinical picture, granulomas can occasionally involve lymph nodes, skin, liver, and other organs. Separately, and over the long term, occupational beryllium exposure carries an increased risk of lung cancer (IARC Group 1), a concern that is independent of whether a person develops CBD.
6. Diagnosis & Laboratory Testing
Diagnosing chronic beryllium disease is fundamentally about answering two questions: Is this person immunologically sensitized to beryllium? and Do they have granulomatous lung disease? Establishing both — in someone with a credible history of beryllium exposure — is what separates CBD from sarcoidosis and other granulomatous diseases. The American Thoracic Society has published an official statement on the diagnosis and management of beryllium sensitivity and CBD that frames the modern approach.
The key test: the beryllium lymphocyte proliferation test (BeLPT)
The cornerstone of diagnosis is the beryllium lymphocyte proliferation test (BeLPT), an immune (not a metal-level) assay. White blood cells (lymphocytes) are isolated from a blood sample, cultured in the laboratory, and exposed to beryllium salts. If the person has beryllium-specific T cells, those cells proliferate in response — a measurable surge in cell division that a beryllium-naive immune system does not show. A clearly increased proliferation indicates sensitization.
Practical points clinicians weigh when interpreting the BeLPT:
- It detects sensitization, not disease. An abnormal blood BeLPT tells you the immune response exists; it does not by itself prove granulomas are present in the lung.
- Confirmation and repetition matter. Because any single run has a meaningful chance of a borderline or discordant result, programs typically require two abnormal tests (often run at independent laboratories, or repeated over time) before calling someone sensitized, which improves reliability.
- Blood versus lung fluid. The test can be run on blood or, more sensitively, on cells recovered from the lung itself by bronchoalveolar lavage (BAL) — washing a segment of lung with saline during bronchoscopy and analyzing the retrieved cells. A BAL BeLPT is often more sensitive than the blood test and is especially useful when blood results are equivocal.
Confirming granulomas: biopsy
To establish disease rather than mere sensitization, tissue is usually obtained by transbronchial lung biopsy during the same bronchoscopy. Finding noncaseating granulomas (and/or mononuclear-cell infiltration) in the lung of a beryllium-sensitized, beryllium-exposed person confirms CBD. Special stains and cultures are performed to exclude infections (such as tuberculosis and fungi) that can also produce granulomas. The combination — positive BeLPT plus granulomas plus exposure — is what distinguishes CBD from sarcoidosis, which is otherwise histologically identical.
Imaging and lung-function testing
Imaging and physiology gauge how much the lungs are affected and help track disease over time:
- High-resolution computed tomography (HRCT) of the chest is far more sensitive than a plain chest X-ray and may show small nodules, thickening along the bronchovascular bundles and interlobular septa, enlarged hilar and mediastinal lymph nodes, ground-glass opacity, and, in advanced cases, fibrosis. A normal or near-normal scan, however, does not rule out early CBD.
- Pulmonary function tests (PFTs) may be normal early and later reveal a restrictive pattern (reduced lung volumes), an obstructive pattern, or a mixed pattern, frequently with a reduced diffusing capacity (DLCO) — a measure of how well oxygen crosses from air into blood — which is often the earliest functional abnormality.
- Cardiopulmonary exercise testing can uncover gas-exchange abnormalities that appear only under the stress of exertion, when resting tests still look normal.
Putting it together, and what the metal levels do (and do not) tell you
A confident CBD diagnosis rests on a triad: a documented beryllium exposure, immunologic sensitization (abnormal BeLPT on blood or BAL), and granulomatous pathology on lung biopsy, with infection and other causes excluded. Notably, measuring beryllium in blood or urine is not used to diagnose CBD — those levels reflect recent exposure at best and are usually unrevealing because the disease-driving metal is sequestered in tissue. The diagnosis is immunologic and histologic, not a question of how many micrograms show up in a body fluid.
7. Treatment & Management
First and most important: remove the exposure
There is no chelation therapy for beryllium — the binding agents used to pull lead or mercury out of the body do not help in beryllium disease, because the problem is an ongoing immune reaction rather than a circulating metal burden. The single most important intervention is to end further exposure. For a sensitized worker or someone with early CBD, removal from beryllium work (or rigorous protection) can slow or halt progression and is the foundation on which everything else is built.
Anti-inflammatory and immunosuppressive treatment
Because CBD is driven by immune-mediated inflammation, treatment for symptomatic or progressive disease relies on dampening that inflammation:
- Corticosteroids (such as oral prednisone) are the mainstay. They suppress the granulomatous inflammation and can improve symptoms, lung function, and imaging in many patients. Treatment is often prolonged, and the well-known side effects of long-term steroids (bone loss, elevated blood sugar, weight gain, infection risk, and others) must be monitored and managed.
- Steroid-sparing immunosuppressants (for example methotrexate, azathioprine, or similar agents) are added or substituted when steroids alone are insufficient, when side effects are limiting, or to reduce the cumulative steroid dose over time.
- Watchful waiting is appropriate for people who are sensitized only, or who have mild, stable, asymptomatic CBD; not every patient needs immediate drug therapy, but all need regular surveillance (symptoms, PFTs/DLCO, and imaging) to catch progression early.
Supportive and advanced care
As disease advances, management mirrors that of other progressive interstitial lung diseases: supplemental oxygen for low blood oxygen, pulmonary rehabilitation to maintain function and quality of life, vaccination and prompt treatment of respiratory infections, and management of complications such as pulmonary hypertension. In end-stage, treatment-refractory CBD with respiratory failure, lung transplantation may be considered. Because of the elevated lung-cancer risk, exposed patients also warrant attention to smoking cessation and appropriate lung-health follow-up.
8. Prevention & Risk Reduction
Controlling exposure at the source
Because there is no cure and no chelator, prevention is the real treatment for beryllium disease. The classic occupational-hygiene hierarchy applies, with engineering controls preferred over reliance on protective equipment:
- Engineering controls: enclosed processes, local exhaust ventilation at grinding, machining, and welding stations, wet methods to suppress dust, and HEPA filtration. The aim is to keep respirable beryllium out of the air in the first place.
- Work practices and housekeeping: HEPA vacuuming rather than dry sweeping or compressed-air blow-down (which re-suspends dust), prompt cleanup of surface contamination, and strict separation of "clean" and "dirty" areas.
- Skin and respiratory protection: properly fitted respirators where airborne control is incomplete, plus gloves and protective clothing, given that skin contact can also drive sensitization.
- Preventing take-home exposure: dedicated work clothing laundered on-site, change rooms and showers, and keeping street clothes and personal items away from contaminated zones — measures specifically intended to protect workers’ families.
Regulation and exposure limits
U.S. occupational regulation tightened substantially with a 2017 Occupational Safety and Health Administration (OSHA) rule that lowered the permissible exposure limit (PEL) for beryllium and added a short-term exposure limit, plus requirements for exposure assessment, control, training, and medical surveillance. The lowering of the limit reflected mounting evidence that disease — especially sensitization — was occurring at the older, higher "safe" level. Agencies including the National Institute for Occupational Safety and Health (NIOSH) and the Agency for Toxic Substances and Disease Registry (ATSDR) provide complementary guidance, and beryllium’s IARC Group 1 carcinogen classification underpins the strict regulatory stance.
Medical surveillance with the BeLPT
For workers with potential exposure, periodic medical surveillance built around the blood BeLPT is the key secondary-prevention tool. Screening identifies sensitized workers before they have symptoms or established disease, allowing exposure reduction and closer monitoring that can intercept CBD early — when removal from exposure does the most good. Surveillance programs typically pair the BeLPT with symptom review, lung-function testing, and, when sensitization is found, evaluation for disease and a plan for ongoing follow-up. The combination of strict exposure control plus BeLPT-based surveillance is the most effective strategy currently available against a disease for which there is no cure.
9. Related Topics
- Heavy Metals — overview of toxic metals, exposure routes, and shared principles of metal toxicity.
- Cadmium — another occupational metal toxicant with prominent lung and kidney effects.
- Arsenic — classic toxic metalloid and recognized human carcinogen.
- Lead — the archetypal heavy-metal poison, in contrast to beryllium’s immune mechanism.
- Mercury — another well-studied toxic metal with distinct organ targets.
- Pulmonology — lung diseases, including granulomatous and interstitial conditions that overlap with CBD.
- Lab Tests — background on diagnostic testing, including specialized immune assays.
- All Minerals — the full minerals section, essential and toxic.
10. Key Research Papers
- Balmes JR, Abraham JL, Dweik RA, et al. An official American Thoracic Society statement: diagnosis and management of beryllium sensitivity and chronic beryllium disease. American Journal of Respiratory and Critical Care Medicine. 2014;190(10):e34–e59.
- Newman LS, Mroz MM, Balkissoon R, Maier LA. Beryllium sensitization progresses to chronic beryllium disease: a longitudinal study of disease risk. American Journal of Respiratory and Critical Care Medicine. 2005;171(1):54–60.
- Richeldi L, Sorrentino R, Saltini C. HLA-DPB1 glutamate 69: a genetic marker of beryllium disease. Science. 1993;262(5131):242–244.
- Fontenot AP, Falta MT, Kappler JW, Dai S, McKee AS. Beryllium-induced hypersensitivity: genetic susceptibility and neoantigen generation. The Journal of Immunology. 2016;196(1):22–27.
- Fontenot AP. Immunologic effects of beryllium exposure. Annals of the American Thoracic Society. 2018;15(Suppl 2):S81–S85.
- Falta MT, Pinilla C, Mack DG, et al. Metal-specific CD4+ T-cell responses induced by beryllium exposure in HLA-DP2 transgenic mice. Mucosal Immunology. 2016;9(1):218–228.
- Van Dyke MV, Martyny JW, Mroz MM, et al. Exposure and genetics increase risk of beryllium sensitisation and chronic beryllium disease. Occupational and Environmental Medicine. 2011;68(11):842–848.
- Martin AK, Mack DG, Falta MT, et al. Beryllium-specific CD4+ T cells in blood as a biomarker of disease progression. Journal of Allergy and Clinical Immunology. 2011;128(5):1100–1106.
- Cherry N, Beach J, Burstyn I, et al. Genetic susceptibility to beryllium: a case-referent study of men and women of working age with sarcoidosis or other chronic lung disease. Occupational and Environmental Medicine. 2015;72(1):21–27.
- Schubauer-Berigan MK, Deddens JA, Couch JR, Petersen MR. Risk of lung cancer associated with quantitative beryllium exposure metrics within an occupational cohort. Occupational and Environmental Medicine. 2011;68(5):354–360.
- Mack DG, Falta MT, McKee AS, et al. Regulatory T cells modulate granulomatous inflammation in an HLA-DP2 transgenic murine model of beryllium-induced disease. Proceedings of the National Academy of Sciences USA. 2014;111(22):8147–8152.
- Cloeren M, Chen R, Ringen K, et al. Beryllium disease among construction trade workers at Department of Energy nuclear sites: a follow-up. American Journal of Industrial Medicine. 2022;65(8):634–644.
- Agency for Toxic Substances and Disease Registry (ATSDR). Toxicological Profile for Beryllium. U.S. Department of Health and Human Services. Available via ATSDR ToxProfiles.
- Occupational Safety and Health Administration (OSHA). Beryllium — Occupational Exposure to Beryllium (Final Rule, 2017); Safety and Health Topics. U.S. Department of Labor. osha.gov/beryllium.