Manganese Toxicity (Manganism): A Parkinson-Like Neurological Disorder
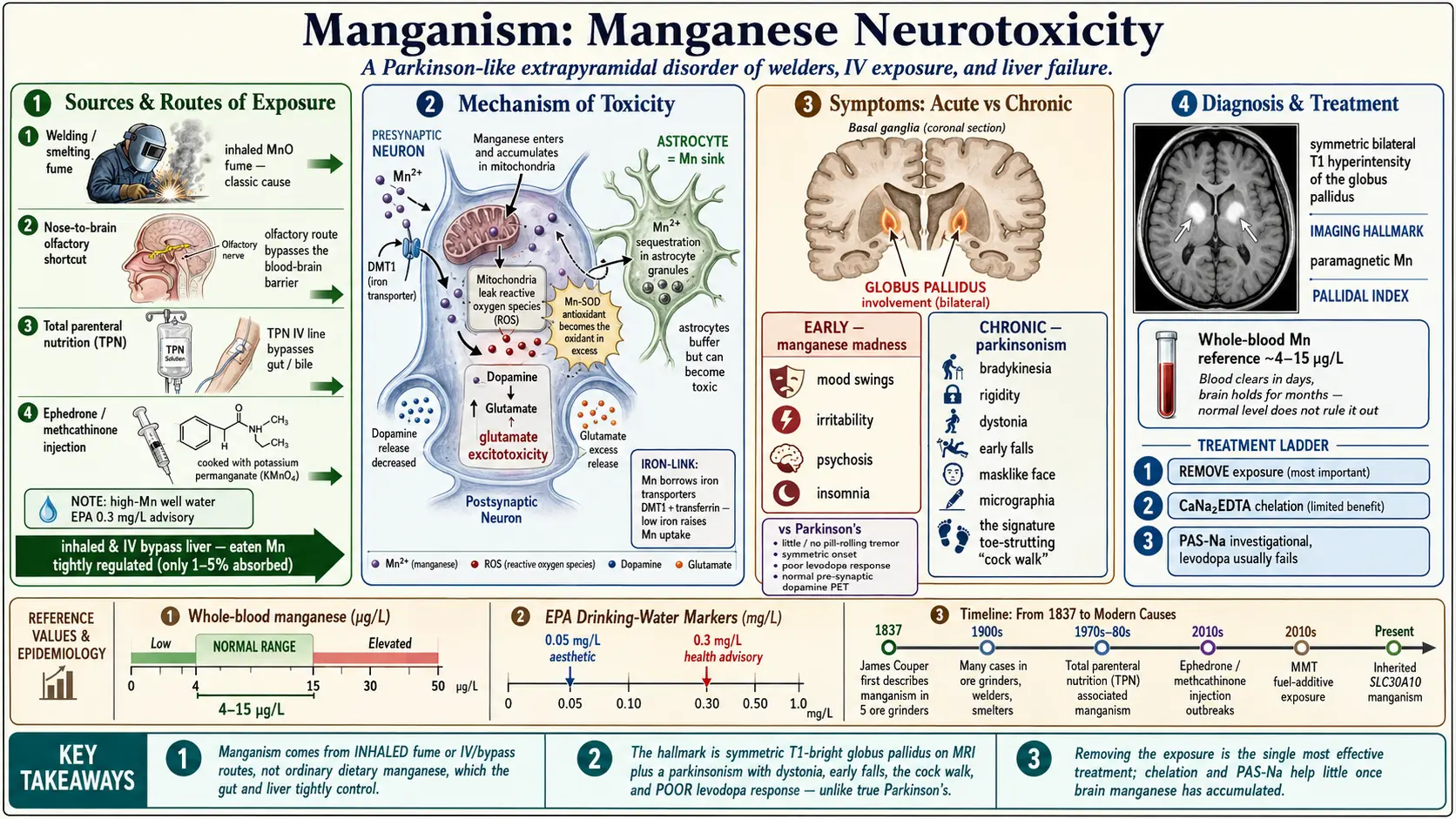
Table of Contents
- Overview
- Sources & Routes of Exposure
- Toxicokinetics
- Mechanism of Toxicity
- Symptoms & Health Effects
- Diagnosis & Laboratory Testing
- Treatment & Management
- Prevention & Risk Reduction
- Related Topics
- Key Research Papers
- Connections
- Featured Videos
1. Overview
Manganese is one of nature's contradictions: a metal your body cannot live without, yet one that can poison the brain when it accumulates. In trace amounts manganese (chemical symbol Mn) is an essential nutrient. It activates enzymes that build bone and cartilage, that switch on the body's own antioxidant defenses (manganese superoxide dismutase, the chief antioxidant inside your mitochondria), and that help process carbohydrates and clear ammonia from the blood. A typical adult carries only about 10–20 milligrams of manganese in the whole body and needs perhaps 2–3 milligrams a day from food. For the chemistry of the essential nutrient, see the companion page on manganese as an essential trace mineral.
Dietary deficiency of manganese in humans is extraordinarily rare; the danger that brings people to a neurologist is almost always the opposite problem — chronic excess. When too much manganese reaches the brain over months or years, it concentrates in a cluster of deep movement-control structures called the basal ganglia, especially a region named the globus pallidus. The result is a slowly progressive neurological disease called manganism.
Manganism is an extrapyramidal disorder, meaning it disrupts the brain circuits that fine-tune posture, balance, and automatic movement. Clinically it looks a great deal like Parkinson's disease — slowness, stiffness, a shuffling walk — which is why it is often called a "Parkinson-like" or "parkinsonian" syndrome. But it is a distinct illness with its own fingerprint, its own causes, and a very different response to treatment. Recognizing those differences matters, because the standard Parkinson's drug, levodopa, usually does little for manganism, and because the most effective "treatment" is something no pill can do: getting the person away from the manganese.
Who first described it
Manganism is not a new disease. In 1837 the Scottish physician James Couper described five men who ground manganese dioxide in a chemical works and developed a strange weakness of the legs, a masklike face, and slurred speech. For most of the next two centuries the condition was an occupational illness of miners and ore processors. The twenty-first century has added newer, sometimes self-inflicted, sources — from intravenous drug use to long-term hospital nutrition — that are described below.
2. Sources & Routes of Exposure
Manganism is almost always a disease of inhalation or of bypassing the gut. This is the single most important idea for understanding who is at risk. When manganese is eaten in food or water, the intestine and the liver tightly regulate how much enters the body and rapidly dump the excess into bile. When manganese is breathed in as fume or dust, or delivered straight into a vein, those control points are skipped, and the metal reaches the brain far more readily.
Occupational inhalation — the classic cause
The historical and still the most common cause is breathing manganese-containing fume or dust on the job. High-risk occupations include:
- Welders, especially those working in confined or poorly ventilated spaces, who inhale fine manganese oxide fume generated as the electrode and steel vaporize.
- Miners of manganese ore and workers who crush or grind the ore.
- Smelter, ferroalloy, and steel workers who produce or handle manganese alloys at high temperature.
- Dry-cell battery manufacturing workers, where manganese dioxide is a key material.
- Producers of fungicides, ceramics, glass, and certain pigments.
In these settings the dose that matters is cumulative — total exposure built up over years — and studies of welders have shown a measurable, dose-dependent worsening of parkinsonian signs as cumulative exposure rises.
Air pollution from fuel additives
A combustion additive called MMT (methylcyclopentadienyl manganese tricarbonyl) is used in some countries as an anti-knock agent in gasoline, in place of the lead that was phased out for the same purpose. Burning MMT releases fine manganese particles into the air. Whether ordinary roadside exposure to MMT causes neurological harm in the general public is still debated, but it is a recognized way that manganese enters the outdoor air people breathe.
Contaminated drinking water
Manganese occurs naturally in groundwater, and some private wells contain high levels. Although the gut regulates swallowed manganese, several studies — particularly in children — have linked high-manganese well water to subtle problems with attention, memory, and school performance, suggesting that the intestinal "gatekeeper" can be overwhelmed when concentrations are very high and exposure is lifelong. The U.S. EPA sets a secondary (aesthetic) standard of 0.05 milligrams per liter and a health-based advisory level of 0.3 milligrams per liter for drinking water.
Medical and bypass routes
Some of the most severe modern cases come from manganese that never passes through the digestive tract:
- Total parenteral nutrition (TPN) — intravenous feeding for people who cannot eat. Manganese is added to the feeding solution as a trace element, but because it is infused directly into the bloodstream it bypasses the intestinal and biliary controls and can build up in the brain. Infants on long-term TPN, and adults with liver disease that blocks biliary excretion, are especially vulnerable.
- Intravenous drug use — people who inject a home-made stimulant called ephedrone or methcathinone are at high risk. These drugs are cooked from pseudoephedrine using potassium permanganate, leaving large amounts of manganese in the injected product. The result is a severe, distinctive, and largely irreversible manganese-induced parkinsonism that has been reported across Eastern Europe and the former Soviet states.
3. Toxicokinetics
"Toxicokinetics" simply means what the body does with a toxin — how it gets in, where it goes, and how it leaves. Manganese has an unusual story on every count, and these quirks explain who gets sick.
Absorption and the body's gatekeepers
From food, only a small fraction of manganese — roughly 1 to 5 percent — is actually absorbed, and the body adjusts that fraction up or down to keep itself in balance. The main exit door is the liver, which packages excess manganese into bile and sends it out through the intestine in the stool. This biliary route is the master regulator of how much manganese the body holds. Anything that opens a back door around the gut and liver — an intravenous line, or a failing liver — defeats this system and lets manganese accumulate.
The nose-to-brain shortcut
Inhaled manganese is dangerous for a second reason beyond skipping the liver. Tiny manganese particles deposited high in the nose can travel directly along the olfactory nerve into the brain, the so-called olfactory route, completely bypassing the bloodstream and the protective blood–brain barrier. This nose-to-brain pathway helps explain why airborne exposure is so much more neurotoxic, dose for dose, than swallowed manganese.
The iron connection
Manganese does not have its own dedicated transport system; it borrows the machinery the body uses for iron. It rides on the same intestinal importer (DMT1) and the same blood carrier (transferrin) that move iron. This shared plumbing has a critical consequence: when the body is iron-deficient, it ramps up these transporters to scavenge more iron — and inadvertently pulls in more manganese as well. People with low iron stores, including many menstruating women and young children, therefore absorb and retain more manganese from the same exposure. For the iron side of this relationship, see the pages on iron and iron overload.
Where it lands
Once inside the brain, manganese concentrates in the basal ganglia and especially the globus pallidus, the structure most consistently damaged in manganism. Manganese is paramagnetic, which (as Section 6 explains) is why these deposits light up brightly on a particular type of MRI scan. Crucially, the brain has no efficient way to actively pump manganese back out, so once it accumulates it tends to linger for months even after exposure stops.
4. Mechanism of Toxicity
Why does a metal the brain needs in trace amounts become a poison in excess? Manganism is not the work of a single broken switch but of several overlapping forms of damage that converge on the same vulnerable circuits.
Mitochondrial poisoning and oxidative stress
Manganese is preferentially taken up by mitochondria, the energy factories inside every cell. There it interferes with the electron-transport chain that makes cellular fuel, which causes the mitochondria to leak reactive oxygen species — unstable molecules that corrode proteins, membranes, and DNA. This is a bitter irony: in trace amounts manganese is the metal at the heart of manganese superoxide dismutase, an enzyme that defends mitochondria against exactly these reactive molecules; in excess, manganese becomes the source of the very oxidative stress that enzyme evolved to neutralize.
Disruption of brain chemical messengers
The basal ganglia run on a careful balance of neurotransmitters — chiefly dopamine, but also glutamate and GABA. Manganese disturbs this balance. Early in the disease it appears to interfere with how dopamine is handled and released in the globus pallidus, while leaving the dopamine-producing cells of the substantia nigra relatively intact — a key difference from Parkinson's disease that is explored in the next two sections. Manganese also promotes the build-up of glutamate, an excitatory messenger that, in excess, is toxic to neurons (a process called excitotoxicity).
Astrocytes as a manganese sink
Within the brain, manganese is taken up heavily by astrocytes, the support cells that nourish neurons and regulate their chemical environment. Overloaded astrocytes mishandle glutamate and lose their ability to buffer the neurons around them, so a chemical insult that begins in the support cells spreads to the movement-control neurons they are supposed to protect. In the special case of liver failure (Section 5), the same astrocyte injury also drives the confusion of hepatic encephalopathy.
Why the damage is hard to reverse
Because manganism injures structures downstream of the brain's dopamine factory rather than the factory itself, and because the brain cannot readily flush manganese back out, the damage tends to lock in. Some patients continue to worsen for months or even years after exposure ends — a feature that distinguishes manganism from many other poisonings, in which removal from exposure brings prompt recovery.
5. Symptoms & Health Effects
Manganism typically unfolds in stages over months to years. Understanding both the early warning signs and how the full syndrome differs from ordinary Parkinson's disease is the most clinically important part of this topic.
The early "manganese madness" phase
Before the movement problems become obvious, heavy early exposure can produce a striking psychiatric and behavioral phase, historically called "manganese madness" (or, in French mining literature, locura manganica). Workers may develop emotional instability and mood swings, irritability and aggression, compulsive or inappropriate behavior such as uncontrollable laughing or crying, nervousness, insomnia, and — in severe high-dose cases — vivid hallucinations and psychosis. These changes are often mistaken for a primary mental-health problem, which can delay recognition of the true cause. As the disease advances, the psychiatric symptoms tend to fade and are replaced by the slow, stiff "burned-out" parkinsonian phase.
The movement disorder
The motor stage of manganism resembles Parkinson's disease and includes:
- Bradykinesia — slowness and poverty of movement, the most consistent feature.
- Rigidity — stiff, resistant muscles.
- Gait and balance disturbance early — a tendency to fall and a clumsy, unsteady walk that often appears sooner and more prominently than in Parkinson's disease.
- Dystonia — sustained, twisting muscle contractions and abnormal postures of the face, hands, and feet, which are more characteristic of manganism than of typical Parkinson's.
- Soft, monotone speech and a masklike, expressionless face.
- Micrographia — small, cramped handwriting.
The "cock walk" — a near-signature finding
A particularly distinctive sign of advanced manganism is the "cock walk" (also called the coq gait): the person walks high on the toes and the balls of the feet, with elbows flexed and the spine held erect, strutting like a rooster. This characteristic dystonic, toe-walking gait is rarely seen in idiopathic Parkinson's disease and, when present, strongly points toward manganese as the culprit.
How manganism differs from idiopathic Parkinson's disease
Although the two diseases overlap, several features help tell them apart — a distinction with real consequences for treatment:
- Tremor: the classic "pill-rolling" resting tremor that is the hallmark of Parkinson's disease is often mild or absent in manganism; when tremor occurs it is more likely to be an action or postural tremor.
- Dystonia and the cock walk: prominent dystonia and the toe-strutting gait favor manganism.
- Early falls and gait failure: balance problems and falls tend to appear earlier in manganism.
- Psychiatric onset: an early phase of emotional lability, hallucinations, or psychosis favors manganism.
- Symmetry: manganism usually affects both sides of the body roughly equally from the start, whereas Parkinson's disease characteristically begins on one side.
- Levodopa response: Parkinson's disease responds robustly to levodopa; manganism characteristically responds poorly or not at all (see Section 7).
- Brain imaging of dopamine: specialized dopamine PET and DAT-SPECT scans differ. In Parkinson's disease the pre-synaptic dopamine system (the nigrostriatal nerve terminals) is degenerated and these scans are abnormal; in manganism the injury is mainly downstream in the globus pallidus, so pre-synaptic dopamine imaging is often relatively normal. This contrast is one of the more reliable ways to separate the two.
Beyond the brain, very high inhalation exposure can also irritate the lungs (so-called "metal fume" respiratory effects), and there is concern about subtler cognitive and motor effects at exposures below those that cause full-blown manganism.
6. Diagnosis & Laboratory Testing
There is no single test that proves manganism. The diagnosis is built from three pillars: a careful exposure history, a neurological examination showing the pattern above, and supportive laboratory and imaging findings. For an overview of how toxic-metal testing fits into broader workups, see the laboratory tests section.
Whole-blood manganese
The usual blood test is whole-blood manganese (not serum or plasma), because most manganese in blood is carried inside red blood cells. A common reference range for whole-blood manganese in adults is roughly 4–15 micrograms per liter (µg/L), equivalent to about 73–273 nanomoles per liter, though exact ranges vary by laboratory and method. A recent or ongoing exposure often raises this value.
There is, however, a crucial caveat that clinicians and patients must understand: blood manganese correlates poorly with the amount of manganese in the brain. Manganese clears from the blood within hours to days, while it can persist in the brain for months. A normal blood level therefore does not rule out manganism, and a modestly elevated level does not, by itself, prove that the brain is affected. Blood manganese is most useful for confirming that exposure is occurring and for monitoring whether removal from exposure is working — not for measuring brain burden. Twenty-four-hour urinary manganese is sometimes measured, particularly during chelation challenge, but it shares similar limitations.
Brain MRI — the imaging hallmark
The most informative test for manganese deposition is a brain MRI. Because manganese is paramagnetic, it shortens the T1 relaxation time of nearby tissue, which makes manganese-laden regions appear abnormally bright (hyperintense) on T1-weighted images. The signature finding of manganism is symmetric, bilateral T1 hyperintensity of the globus pallidus — the deep basal-ganglia structure glowing white on a T1 scan — sometimes extending to neighboring areas. Radiologists may quantify this with a "pallidal index," comparing the brightness of the globus pallidus to nearby white matter.
This MRI sign is a marker of deposition, not necessarily of permanent damage: it reflects manganese physically present in the tissue, and it characteristically fades over months once exposure stops as the metal slowly clears. It is also not perfectly specific — the very same symmetric T1 pallidal hyperintensity appears in people with chronic liver failure, because their impaired biliary excretion lets manganese accumulate even without occupational exposure (see below). The MRI must therefore always be read alongside the clinical history.
Putting it together
A confident diagnosis of manganism generally requires a plausible source of excess manganese, a compatible parkinsonian or dystonic syndrome (ideally with manganism-favoring features such as early gait failure, dystonia, the cock walk, or a poor levodopa response), and supporting evidence such as elevated whole-blood manganese and/or T1 pallidal hyperintensity on MRI. In younger patients with no obvious exposure — especially with a family history — an inherited manganese-transport disorder (Section 7) should be considered and can be confirmed by genetic testing.
7. Treatment & Management
Treatment of manganism is humbling: there is no reliable cure, and the cornerstone is prevention of further injury rather than reversal of damage already done. Several approaches are used, with honest limits.
Remove the exposure — the single most important step
The first and most effective intervention is to identify and eliminate the source of manganese. For a welder or miner that means leaving the exposure, improving ventilation, or changing jobs; for someone on intravenous feeding it means adjusting or removing the manganese in the solution; for an ephedrone user it means stopping the drug. Because the brain clears manganese slowly, improvement after removal is gradual and incomplete, and some patients keep worsening for a time before stabilizing — but stopping the exposure halts the ongoing insult and is the foundation of every treatment plan.
Chelation
Chelation uses a drug that binds the metal so it can be flushed out in the urine. The agent best studied for manganese is CaNa2EDTA (calcium disodium edetate). It does measurably increase the amount of manganese excreted in the urine, but its clinical benefit is limited — symptoms often change little even when urinary manganese rises — probably because EDTA cannot easily reach the manganese already locked inside brain tissue. Chelation is therefore not a dependable rescue, though it may be tried, especially when ongoing exposure has produced a high body burden.
PAS-Na (para-aminosalicylic acid)
An older anti-tuberculosis drug, sodium para-aminosalicylic acid (PAS-Na), has drawn renewed interest. Reports from China — beginning with two chronic-manganese-poisoning cases treated successfully in the early 1990s — and more recent reviews describe meaningful, sometimes lasting, clinical improvement, possibly because PAS penetrates the brain better than EDTA and may also calm inflammation. PAS-Na remains investigational for manganism rather than a standard, widely approved therapy, but it is among the more promising specific treatments.
Levodopa usually does not work
It is natural to reach for levodopa, the mainstay of Parkinson's disease, and a trial is reasonable to confirm the diagnosis. But because manganism damages targets downstream of the brain's dopamine-producing cells rather than the cells themselves, levodopa is generally ineffective in manganism. A poor response, in fact, is one of the clues that the parkinsonism is due to manganese rather than ordinary Parkinson's disease. Other symptom-directed measures — physical and occupational therapy, treatment of dystonia, and management of mood and psychiatric symptoms — remain valuable for quality of life.
Special situations: liver disease and inherited transport defects
When manganese accumulates because the liver cannot excrete it — in cirrhosis, chronic liver failure, or a portosystemic shunt — managing the underlying liver disease is central. In these patients, brain manganese deposition contributes to cirrhosis-related hepatic encephalopathy and to a condition called acquired hepatocerebral degeneration; the T1-bright globus pallidus on MRI is a familiar sight in advanced liver disease, and it can improve after liver transplantation. A rare inherited cause deserves mention: mutations in the manganese-transport gene SLC30A10 (and the related gene SLC39A14) cause a hereditary syndrome of hypermanganesemia with dystonia, liver disease, and high red-cell counts (polycythemia). These genetic forms are treated quite differently — with chelation plus iron supplementation, which competes manganese out of the shared transport machinery.
8. Prevention & Risk Reduction
Because established manganism is so difficult to reverse, nearly all of the meaningful action lies in preventing excess exposure in the first place. The good news is that, unlike idiopathic Parkinson's disease, manganism has identifiable and largely controllable causes.
In the workplace
- Ventilation and fume extraction. Local exhaust ventilation at the welding arc or grinding point removes manganese fume at its source. Confined-space welding deserves special caution.
- Respiratory protection. Properly fitted respirators reduce inhaled dose when engineering controls are not enough.
- Exposure limits and monitoring. Occupational agencies set airborne manganese limits, and periodic air sampling helps confirm controls are working.
- Health surveillance. Watching for early neurological or psychiatric changes in exposed workers allows removal from exposure before disease becomes fixed. Because cumulative dose drives risk, reducing exposure even partway through a career still matters.
In drinking water and the home
- Test private wells for manganese, particularly before giving the water to infants and young children. Treatment systems (oxidation-filtration, ion exchange, or reverse osmosis) can lower high levels.
- Be mindful that iron deficiency increases manganese uptake: correcting low iron stores is a reasonable, health-promoting step that also reduces how much manganese the body absorbs from any source.
In medical care
- Review manganese in intravenous nutrition. Patients on long-term TPN — especially infants and anyone with cholestasis or liver disease — should have manganese content reviewed and blood levels and, if indicated, brain MRI monitored, because the intravenous route bypasses the body's natural controls.
- Watch the liver. In people with cirrhosis or portosystemic shunting, clinicians should remember that impaired biliary excretion alone can raise brain manganese and contribute to encephalopathy.
A note on dietary manganese
For the general public eating an ordinary diet, manganese from food is not a meaningful poisoning risk — the gut and liver handle it well, and manganese is a needed nutrient. There is no reason to fear manganese in whole foods such as grains, nuts, legumes, leafy greens, and tea. The concern in this article is reserved for inhaled manganese, very high well-water levels, the intravenous routes, and liver failure — the situations in which the body's safeguards are bypassed or broken.
9. Related Topics
- Manganese (essential trace mineral) — the nutrient side of this same metal: why the body needs it and how deficiency (rare) differs from the excess described here.
- Toxic Minerals — overview hub for minerals and metals that harm health in excess.
- Heavy Metals — the broader family of neurotoxic and systemic metal poisonings.
- Lead — another classic occupational and environmental neurotoxic metal.
- Iron Overload — relevant because manganese shares iron's transporters.
- Iron — iron status directly affects how much manganese the body absorbs.
- Copper — another essential trace metal that is neurotoxic in excess.
- Parkinson's Disease — the idiopathic disorder manganism mimics, and the key clinical comparison.
- Cirrhosis — impaired biliary manganese excretion contributes to brain deposition and encephalopathy.
- Liver Disease — chronic liver failure is a major non-occupational cause of manganese accumulation.
- Lab Tests — how whole-blood manganese and related metal testing fit into a diagnostic workup.
- All Minerals — the full minerals section.
10. Key Research Papers
- Guilarte TR. Manganese neurotoxicity: new perspectives from behavioral, neuroimaging, and neuropathological studies in humans and non-human primates. Front Aging Neurosci. 2013;5:23.
- Stepens A, Logina I, Liguts V, et al. A parkinsonian syndrome in methcathinone users and the role of manganese. N Engl J Med. 2008;358(10):1009–1017.
- Racette BA, Searles Nielsen S, Criswell SR, et al. Dose-dependent progression of parkinsonism in manganese-exposed welders. Neurology. 2017;88(4):344–351.
- Sikk K, Haldre S, Aquilonius SM, Taba P. Manganese-induced parkinsonism due to ephedrone abuse. Parkinsons Dis. 2011;2011:865319.
- Avelino MA, Fusão EF, Pedroso JL, et al. Inherited manganism: the "cock-walk" gait and typical neuroimaging features. J Neurol Sci. 2014;341(1–2):150–152.
- Ky SQ, Deng HS, Xie PY, Hu W. A report of two cases of chronic serious manganese poisoning treated with sodium para-aminosalicylic acid. Br J Ind Med (Occup Environ Med). 1992;49(1):66–69.
- Xie X, Song W, Peng C, et al. Treatment of manganese and lead poisoning with sodium para-aminosalicylic acid: a contemporary update. Toxicol Lett. 2024;398:69–81.
- Alves G, Thiebot J, Tracqui A, et al. Neurologic disorders due to brain manganese deposition in a jaundiced patient receiving long-term parenteral nutrition. JPEN J Parenter Enteral Nutr. 1997;21(1):41–45.
- Iwase K, Higaki J, Mikata S, et al. Manganese deposition in basal ganglia due to perioperative parenteral nutrition following gastrointestinal surgeries. Dig Surg. 2002;19(3):174–183.
- Tuschl K, Clayton PT, Gospe SM, et al. Syndrome of hepatic cirrhosis, dystonia, polycythemia, and hypermanganesemia caused by mutations in SLC30A10, a manganese transporter in man. Am J Hum Genet. 2012;90(3):457–466.
- Quadri M, Federico A, Zhao T, et al. Mutations in SLC30A10 cause parkinsonism and dystonia with hypermanganesemia, polycythemia, and chronic liver disease. Am J Hum Genet. 2012;90(3):467–477.
- Aschner M, Guilarte TR, Schneider JS, Zheng W. The transport of manganese across the blood–brain barrier. Neurotoxicology. 2006;27(3):311–314.
- Spahr L, Butterworth RF, Fontaine S, et al. Increased blood manganese in cirrhotic patients: relationship to pallidal magnetic resonance signal hyperintensity and neurological symptoms. Hepatology. 1996;24(5):1116–1120.
- Bowler RM, Roels HA, Nakagawa S, et al. Dose–effect relationships between manganese exposure and neurological, neuropsychological and pulmonary function in confined space bridge welders. Occup Environ Med. 2007;64(3):167–177.
- Agency for Toxic Substances and Disease Registry (ATSDR). Toxicological Profile for Manganese. U.S. Department of Health and Human Services. 2012.
- World Health Organization. Manganese in Drinking-Water: Background Document for Development of WHO Guidelines for Drinking-Water Quality. 2021.
- National Institutes of Health, Office of Dietary Supplements. Manganese — Health Professional Fact Sheet. Updated 2021.
- U.S. Environmental Protection Agency. Drinking Water Health Advisory for Manganese. EPA. 2004.
Connections
- Manganese (essential trace mineral)
- Toxic Minerals
- Heavy Metals
- Lead
- Iron Overload
- Iron
- Copper
- Parkinson's Disease
- Cirrhosis
- Liver Disease
- Lab Tests
- All Minerals