Antimony Toxicity: Stibine Gas, Industrial Exposure, and Health Effects
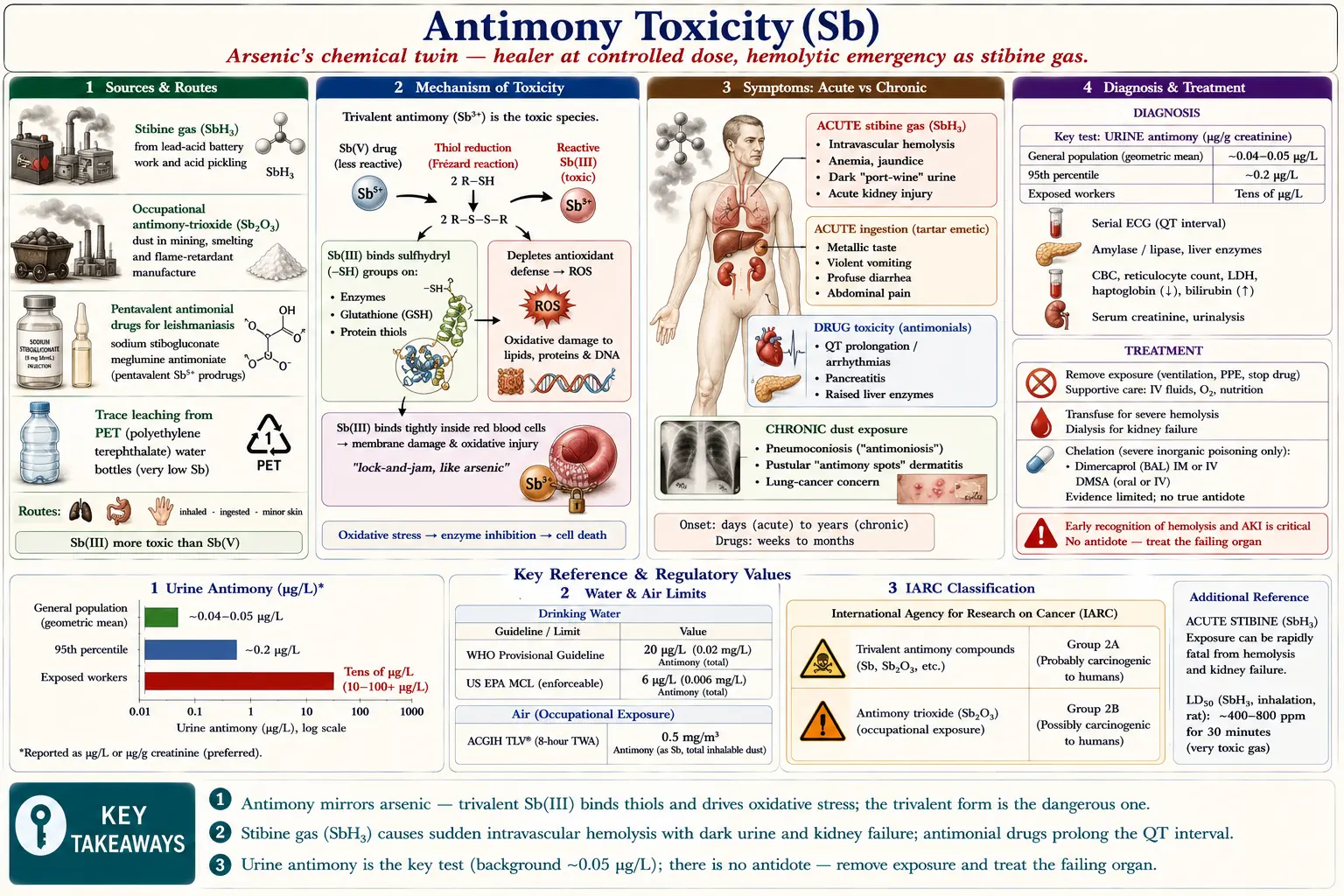
Table of Contents
- Overview
- Sources & Routes of Exposure
- Toxicokinetics
- Mechanism of Toxicity
- Symptoms & Health Effects
- Diagnosis & Laboratory Testing
- Treatment & Management
- Prevention & Risk Reduction
- Related Topics
- Key Research Papers
- Connections
- Featured Videos
1. Overview
Antimony (chemical symbol Sb, from the Latin stibium; atomic number 51) is a silvery-grey metalloid — an element on the borderline between metals and non-metals. It sits in group 15 of the periodic table, the same column as nitrogen, phosphorus, and, most importantly here, arsenic. Because antimony is arsenic's immediate neighbor in that group, the two share much of their chemistry and a striking amount of their toxicology. If you understand how arsenic harms the body, you are most of the way to understanding antimony.
Like arsenic, antimony exists in two oxidation states that behave very differently. Trivalent antimony, Sb(III), is the more toxic form: it binds avidly to sulfur-containing groups on proteins and is more reactive inside cells. Pentavalent antimony, Sb(V), is less acutely toxic and is the form used in medicine. For both arsenic and antimony, the lower (trivalent) oxidation state is the dangerous one. The body and some chemical environments can also reduce Sb(V) back to Sb(III), which matters both for the medicines below and for how the element behaves in tissue.
The therapeutic paradox
Antimony is one of those rare poisons that is also a deliberately administered drug. Pentavalent antimonial medications — sodium stibogluconate (Pentostam) and meglumine antimoniate (Glucantime) — have been first-line treatments for leishmaniasis, a parasitic disease spread by sandfly bites, for the better part of a century, and remain in heavy use across South Asia, the Middle East, East Africa, and Latin America. They work, but even at controlled doses they carry real risks of heart rhythm disturbances, pancreatitis, and liver injury (detailed in the symptoms section). This dual identity, healer and toxin, is the central theme of antimony's story.
Three faces of antimony exposure
For practical purposes, harmful antimony exposure comes in three distinct forms, each with its own clinical picture: stibine gas (SbH3), a rare but dramatic industrial emergency that destroys red blood cells (closely paralleling arsine gas poisoning); inorganic antimony salts and dusts, the slow chronic exposures of miners, smelter workers, and battery and flame-retardant manufacturers (plus rare ingestion of antimony compounds); and trace consumer exposure, chiefly the small amounts that leach from PET plastic bottles into water and juice, generally far below health guidance values but worth understanding honestly.
Antimony is not an essential nutrient — the body has no known requirement for it and no useful biological role has been identified. Everything it does is, at best, neutral and, at higher doses, harmful.
2. Sources & Routes of Exposure
People encounter antimony through three doorways into the body: inhalation (breathing in dust, fumes, or stibine gas), ingestion (swallowing it in water, food, or as a compound), and, to a much lesser degree, skin contact. Which doorway is involved largely determines what kind of illness results — inhaled stibine attacks the blood, swallowed antimony salts attack the gut, and chronic inhaled dust attacks the lungs and skin.
Stibine gas (SbH3)
Stibine, or antimony hydride, is a colorless, foul-smelling gas that is generated accidentally rather than used on purpose. It forms whenever fresh, reactive antimony metal — or antimony-contaminated metal — meets acid or nascent hydrogen. The classic settings are lead-acid battery manufacture and charging (battery plate alloys contain antimony to harden them), metal etching and pickling with acids, and any industrial process that produces hydrogen near antimony-bearing material. It is the direct chemical cousin of arsine (AsH3), the analogous arsenic gas, and the two produce nearly identical emergencies. Because stibine is so much rarer than arsine, many clinicians have never seen a case, which can delay recognition.
Occupational dusts and fumes
The workhorse of chronic antimony exposure is inhaled inorganic dust, dominated by antimony trioxide (Sb2O3). Industries with documented exposure include:
- Mining and smelting of antimony ore (stibnite, antimony sulfide) and of other metals where antimony is a co-contaminant of copper, lead, and gold ores.
- Lead-acid battery production, where antimony-lead alloys are cast and machined.
- Flame-retardant manufacturing. Antimony trioxide is added to plastics, textiles, and electronics as a flame-retardant synergist (it boosts the performance of halogenated retardants). This is the single largest industrial use of antimony today.
- Glass, ceramics, pigments, and solder, where antimony compounds serve as fining agents, opacifiers, and alloy components.
Historically, severe occupational exposure produced a recognized lung disease, sometimes called antimoniosis — a form of pneumoconiosis (dust-deposit lung disease) described in antimony process workers, with chest X-ray changes and respiratory symptoms.
Medicinal antimony
For patients treated for leishmaniasis, the medicine itself is the exposure source. A full therapeutic course of sodium stibogluconate or meglumine antimoniate delivers a substantial, deliberate dose of pentavalent antimony intravenously or intramuscularly over two to four weeks — far more antimony than any environmental source. This is why the toxic effects of antimonials are seen most clearly in the leishmaniasis literature.
Consumer exposure: antimony in PET plastic
This is the source most people will actually encounter, and it deserves honest, non-alarmist treatment. Antimony trioxide is used as a catalyst to manufacture polyethylene terephthalate (PET), the clear plastic of most disposable water and soft-drink bottles. A trace of that catalyst remains in the finished plastic and slowly migrates (leaches) into the liquid inside.
The research findings are consistent: antimony levels in freshly bottled water are very low, but they rise with storage time and rise sharply with heat. Shotyk and Krachler documented that antimony climbs measurably the longer water sits in the bottle. Welle and Franz modeled the migration and showed it is strongly temperature-dependent — a bottle left in a hot car releases far more antimony than one kept cool. Westerhoff and colleagues confirmed leaching from PET used for bottled water.
The reassuring context: even when elevated, the measured concentrations are generally far below the WHO drinking-water guideline of 20 µg/L and the U.S. EPA limit of 6 µg/L (see Diagnosis). The sensible reading is not “PET water is dangerous,” but rather: don't store bottled water for long periods, and don't let it get hot. Glass and stainless steel sidestep the issue entirely.
3. Toxicokinetics
Toxicokinetics is the study of what the body does to a substance — how it gets in (absorption), where it goes (distribution), and how it gets out (excretion). For antimony these steps differ between the trivalent and pentavalent forms, which helps explain both the disease patterns and the choice of diagnostic test.
Absorption
Antimony is absorbed through both the gastrointestinal tract (when swallowed) and the lungs (when inhaled). GI absorption of inorganic antimony is incomplete and erratic, one reason acute oral poisonings vary so much in severity. Inhaled antimony trioxide dust is the dominant occupational route; fine particles deposit deep in the lung and are absorbed slowly, while larger particles are cleared upward and swallowed. Skin absorption through intact skin is minor.
Distribution and binding to red blood cells
Once absorbed, the two oxidation states part ways. Trivalent Sb(III) binds tightly to red blood cells (erythrocytes), concentrating inside them and in sulfhydryl-rich tissues such as the liver, thyroid, and spleen. Pentavalent Sb(V) stays more in the plasma and distributes more diffusely. This is why Sb(III) lingers longer and is more toxic, and why the antimonial drugs (given as Sb(V)) are partly reduced to Sb(III) at their site of action, where the trivalent form is thought to be the active anti-parasitic species.
Excretion: the urine-versus-bile split
The route the body uses to eliminate antimony depends on its oxidation state, and this is the single most practically important fact in the whole section because it dictates the best diagnostic test:
- Pentavalent Sb(V) is cleared mainly in the urine, and relatively quickly. This is why urine antimony is the preferred biomonitoring sample — most relevant exposures, including the medicines and many occupational settings, are excreted renally.
- Trivalent Sb(III) is eliminated more slowly and to a greater extent through the bile and feces, with a longer biological half-life. Because it clings to red cells and tissues, it accumulates more before it leaves.
Across both forms, antimony clears from the body relatively fast compared with metals like lead or cadmium, which is why blood antimony reflects only recent exposure and why elevated levels fall once exposure stops. There is no large long-term skeletal reservoir comparable to lead in bone.
4. Mechanism of Toxicity
Antimony harms cells through the same core chemistry that makes arsenic dangerous. Understanding the mechanism makes the symptoms predictable: the heart, liver, pancreas, and red blood cells suffer because of how antimony interferes with the molecular machinery they depend on.
Binding to sulfhydryl (thiol) groups
The central event is antimony's affinity for sulfhydryl groups — the “–SH” (thiol) chemical handles found on the amino acid cysteine and on small molecules like glutathione, the cell's main internal antioxidant. Trivalent Sb(III), like trivalent arsenic, latches onto these thiol groups. Many enzymes need free, correctly shaped cysteine residues to work; when antimony occupies those sites, the enzymes are inhibited. By tying up glutathione and thiol-bearing enzymes, antimony both disables key metabolic reactions and strips the cell of its antioxidant defenses — the same lock-and-jam mechanism that underlies arsenic toxicity, which is why the two produce overlapping injuries.
Oxidative stress
With glutathione depleted and antioxidant enzymes inhibited, cells are exposed to reactive oxygen species (ROS) — unstable, oxygen-derived molecules that damage lipids, proteins, and DNA. This oxidative stress is a major route to cell injury and death in antimony toxicity, and it helps explain the carcinogenicity concerns surrounding antimony trioxide (oxidative DNA damage is a recognized step toward cancer).
The pentavalent-to-trivalent reduction
A mechanistic detail ties the medicine and the poison together. Pentavalent Sb(V), the form given as a drug, is comparatively inert on its own — but inside cells, thiol-rich molecules reduce Sb(V) to the more reactive Sb(III). Frézard and colleagues showed that biological thiols such as glutathione (and trypanothione, a glutathione relative unique to the leishmania parasite) drive this Sb(V)→Sb(III) conversion. In the parasite this activation is what kills it; in the patient the same reduction contributes to toxicity. The lower oxidation state is, again, the business end of the molecule.
Why these particular organs?
Tissues with high metabolic rates and abundant sulfhydryl chemistry are hit hardest. Red blood cells bind Sb(III) directly and, when overwhelmed (as in stibine exposure), rupture. The heart's conduction system is sensitive to the metabolic and ionic disturbances antimony causes, producing the QT prolongation seen with antimonial drugs. The metabolically intense liver and pancreas show injury (raised enzymes, pancreatitis). Recognizing this pattern is the key to anticipating and monitoring antimony's clinical effects.
5. Symptoms & Health Effects
Antimony's effects depend almost entirely on the form, the dose, and the speed of exposure. The clinical pictures fall into clean categories: acute stibine gas poisoning, acute ingestion of antimony salts, the predictable drug toxicities of antimonial medicines, and chronic occupational exposure. The sections below are organized by organ system within each scenario.
Acute stibine (SbH3) gas poisoning — a hematologic emergency
This is the most dramatic and immediately life-threatening antimony exposure, and it mirrors arsine gas poisoning almost exactly. After an often symptom-free latent period of a few hours, the hallmark is sudden, massive intravascular hemolysis — red blood cells burst inside the bloodstream.
- Blood and constitutional: headache, nausea, weakness, and abdominal or back/flank pain, followed by the signs of hemolysis — anemia (see Anemia), jaundice (yellowing from the breakdown of hemoglobin), and a distinctive picture of free hemoglobin in the blood and urine.
- Kidneys: the flood of free hemoglobin and red-cell debris clogs and poisons the kidney tubules, causing acute kidney injury that can progress to renal failure requiring dialysis (see Kidney Disease). The urine turns dark — red to brown or “port-wine” colored — from hemoglobin, a key clue.
- Whole body: in severe cases the combination of profound anemia and renal failure is fatal without prompt supportive care.
The practical teaching point is that any worker who develops dark urine, jaundice, and anemia after acid work near antimony-containing metal should be treated as a stibine (or arsine) emergency until proven otherwise.
Acute ingestion of antimony salts — a gastrointestinal emergency
Swallowed soluble antimony compounds (historically including tartar emetic, antimony potassium tartrate) act much like arsenic on the gut and were in fact once used deliberately as emetics. The dominant features are violent gastrointestinal:
- Gastrointestinal: a metallic taste, profuse vomiting, and severe watery, sometimes bloody, diarrhea — clinically reminiscent of acute arsenic ingestion. The fluid loss can be dangerous in its own right.
- Cardiovascular and whole-body: dehydration, low blood pressure, collapse, and, with large doses, heart rhythm disturbances. Liver and kidney injury can follow.
Toxicity of antimonial medicines (the leishmaniasis drugs)
Because patients receive a known, sustained dose, the side-effect profile of sodium stibogluconate and meglumine antimoniate is well characterized. These are expected, monitored toxicities, not freak events:
- Cardiotoxicity (the most feared): antimonials prolong the QT interval on the electrocardiogram (ECG) — a measure of the heart's electrical recovery time. Excessive QT prolongation can trigger dangerous ventricular arrhythmias, including torsades de pointes and sudden cardiac death. Chulay and colleagues documented dose-related ECG changes — T-wave flattening/inversion and QT prolongation — during sodium stibogluconate therapy; Ribeiro and colleagues found similar QT and repolarization changes even with low-dose meglumine antimoniate. ECG monitoring during therapy is standard for this reason.
- Pancreatitis: inflammation of the pancreas, with abdominal pain and elevated blood amylase and lipase, is a recognized and sometimes severe complication. Gasser and colleagues described antimonial-induced pancreatitis during leishmaniasis treatment, and pancreatic enzymes are routinely tracked during therapy.
- Hepatotoxicity: reversible elevations in liver enzymes (transaminases) are common; serious liver injury is less common but possible, so liver tests are monitored.
- Other: muscle and joint aches (myalgia, arthralgia), headache, nausea, injection-site pain, and reductions in blood counts can also occur.
Chronic occupational exposure
Long-term, lower-level exposure — mostly from inhaled antimony trioxide dust — produces a slower, more insidious set of problems:
- Respiratory: chronic irritation of the airways with cough, and, with heavy long-term dust exposure, pneumoconiosis (“antimoniosis”) — dust deposits in the lung visible on chest X-ray, described by Potkonjak and Pavlovich in antimony process workers.
- Skin: a characteristic pustular dermatitis historically called “antimony spots” — itchy pustules clustered around sweat and sebaceous glands, seen in workers exposed to antimony dust and heat.
- Cardiac and gastrointestinal: reports of ECG changes and digestive complaints in exposed workers, consistent with antimony's general toxic profile.
- Cancer concern: antimony trioxide is treated as a potential occupational carcinogen on the basis of inhalation studies (discussed in Diagnosis & classification). Newton and colleagues reported lung tumors in rats chronically inhaling antimony trioxide, which underpins the agency classifications.
6. Diagnosis & Laboratory Testing
Diagnosing antimony exposure rests on a good exposure history (occupation, recent leishmaniasis treatment, an industrial accident) combined with laboratory biomonitoring — measuring antimony in body fluids. The key practical message is that urine antimony is the single most useful test for most exposures, because the relevant forms are cleared renally and antimony does not persist long in blood.
Urine antimony — the key test
Urine is the preferred specimen for assessing both occupational and recent environmental antimony exposure. Results are reported either per liter of urine (µg/L) or, better, corrected for urine concentration as µg per gram of creatinine (µg/g creatinine), which adjusts for how dilute or concentrated the sample is.
- General (unexposed) population — normal: very low. U.S. NHANES biomonitoring data (CDC) put the population geometric mean at roughly 0.04–0.05 µg/L (about 0.05 µg/g creatinine), with the 95th percentile near 0.2 µg/L. In plain terms, ordinary people carry only trace amounts. Germany's environmental health reference value (HBM RV95) for children is 0.3 µg/L, in the same low range.
- Elevated / occupational: there is no single official cutoff line, but exposed workers (smelting, antimony trioxide production) typically run one to two orders of magnitude higher — from several µg/L into the tens of µg/L. A result well above the ~0.2 µg/L general-population ceiling, in the right clinical context, signals meaningful exposure. Bailly and colleagues, and Iavicoli and colleagues, established the use of urine antimony for monitoring inorganic-antimony workers.
- Note that the ACGIH has not set a Biological Exposure Index (BEI) for antimony — the data were judged insufficient — so interpretation is comparative (against background levels) rather than against a fixed biological limit.
Blood antimony
Blood (or serum) antimony reflects only recent exposure because the element clears quickly. General-population whole-blood antimony is generally below about 1 µg/L (often well under that), and no formal agency reference value is published for blood. Blood levels are most useful in acute poisoning — for example, confirming exposure during the workup of acute hemolysis — rather than for assessing chronic exposure, where urine is superior.
Supporting laboratory tests by scenario
- Suspected stibine hemolysis: complete blood count (showing anemia), markers of hemolysis (elevated LDH and indirect bilirubin, low haptoglobin, free plasma and urine hemoglobin), a blood film, and kidney function tests (creatinine, urea) and urinalysis to detect acute kidney injury.
- Patients on antimonial drugs: serial ECGs watching the QT interval, plus amylase/lipase (pancreatitis) and liver enzymes (transaminases), monitored throughout the treatment course.
- Chronic occupational surveillance: periodic urine antimony as the biomonitoring backbone, with chest imaging and respiratory assessment where pneumoconiosis is a concern.
Environmental and regulatory benchmarks
Several authoritative numbers anchor what counts as a safe environmental level:
- WHO drinking-water guideline: 0.020 mg/L (20 µg/L) for antimony — noting the WHO labels this value provisional.
- U.S. EPA drinking-water limit (MCL): 0.006 mg/L (6 µg/L), with the health goal (MCLG) set at the same value.
- ACGIH occupational air limit (TLV): 0.5 mg/m3 as antimony, 8-hour time-weighted average.
Carcinogenicity classification
The International Agency for Research on Cancer (IARC) has evaluated antimony compounds more than once. In Monograph Volume 47 (1989), antimony trioxide was classified Group 2B (“possibly carcinogenic to humans”), based largely on the rat inhalation evidence. In a more recent re-evaluation (Volume 131, 2023), IARC classified antimony by oxidation state: trivalent antimony as Group 2A (“probably carcinogenic to humans”) and pentavalent antimony as Group 3 (not classifiable). Because antimony trioxide is a trivalent compound, both classifications are relevant context for occupational risk.
7. Treatment & Management
There is no antidote that simply “neutralizes” antimony. Treatment rests on three pillars: stopping the exposure, supportive care for whatever organ is failing, and, in selected severe inorganic poisonings, chelation to help the body bind and remove the metal. The right combination depends entirely on which of the exposure scenarios is in play.
First and most important: remove the exposure
Nothing else works if exposure continues. For stibine gas, move the person to fresh air immediately while rescuers protect themselves. For occupational dust, remove the worker from the contaminated environment. For antimonial drug toxicity, the clinician weighs reducing the dose or stopping the drug against the need to cure a potentially fatal leishmaniasis — sometimes switching to an alternative such as liposomal amphotericin B or miltefosine.
Supportive care — treat the failing organ
- Hemolysis and kidney failure (stibine): this is largely a supportive-care problem. Management centers on generous intravenous fluids to protect the kidneys, careful attention to electrolytes, blood transfusion for severe anemia, and dialysis if acute kidney injury is severe. Maintaining urine flow helps clear the hemoglobin pigment.
- Acute ingestion: aggressive rehydration and electrolyte replacement to counter the massive vomiting and diarrhea, with cardiac monitoring.
- Drug-induced cardiotoxicity: ECG monitoring, correcting electrolyte abnormalities (especially potassium and magnesium, which worsen QT prolongation), and holding or stopping the drug if the QT interval becomes dangerously long.
- Pancreatitis and hepatotoxicity: standard supportive management plus dose adjustment or discontinuation of the antimonial.
Chelation therapy — useful but evidence-limited
Chelation uses a drug that grabs the metal and carries it out of the body, usually in the urine. For severe inorganic antimony poisoning, the agents borrowed from arsenic and heavy-metal poisoning are:
- Dimercaprol (British Anti-Lewisite, BAL): an older, oil-based injectable chelator with thiol groups that compete with the body's own sulfhydryls for the antimony. It is the traditional choice for acute severe inorganic metalloid poisoning.
- DMSA (succimer) and the related DMPS: newer, water-soluble, oral thiol chelators that are better tolerated than dimercaprol and are used for arsenic and related metalloids.
An honest caveat: the evidence for chelating antimony specifically is limited — much of the rationale is extrapolated from arsenic, where these agents are better studied. Chelation is reserved for genuinely severe inorganic poisonings and is not routine for the antimonial medicines (where dose adjustment is the answer) or for trace consumer exposure (which needs no treatment at all). Chelation decisions should be guided by a poison-control center or medical toxicologist.
What does not need treatment
Plainly: the trace antimony that leaches from a PET water bottle does not call for chelation, “detox” products, or any medical intervention. The appropriate response is preventive — storage and temperature habits — not therapeutic.
8. Prevention & Risk Reduction
Because antimony has no antidote and its worst effects (hemolysis, lung scarring, cancer risk) are hard to reverse, prevention is decisively more valuable than treatment. The strategies differ for workers, patients, and ordinary consumers.
Workplace controls
Occupational antimony disease is largely preventable with standard industrial-hygiene practice, applied in roughly this order of effectiveness:
- Engineering controls first: enclosed processes and local exhaust ventilation to capture dust and fumes at the source — especially critical where stibine can form (battery work, acid pickling of antimony-bearing metal). Suppressing airborne antimony trioxide is the single highest-impact measure.
- Respiratory and skin protection: appropriate respirators where dust cannot be fully controlled, and protective clothing to prevent “antimony spots” dermatitis and skin contact.
- Hygiene practices: no eating, drinking, or smoking in work areas; washing before breaks; and keeping work clothes out of the home to avoid take-home contamination.
- Medical surveillance: periodic urine antimony biomonitoring to confirm controls are working, plus respiratory monitoring where pneumoconiosis is a risk, staying within the ACGIH TLV of 0.5 mg/m3.
Safer prescribing of antimonial medicines
For leishmaniasis patients, prevention of drug toxicity means baseline and serial ECGs to catch QT prolongation early, monitoring of pancreatic and liver enzymes, correcting electrolytes before and during treatment, weight-based dosing, and a low threshold to pause or switch to alternative therapies (liposomal amphotericin B, miltefosine, paromomycin) when toxicity appears. In regions where antimonial resistance has risen — documented especially in parts of South Asia — alternative drugs may also be preferred on efficacy grounds.
Reducing consumer exposure from PET plastic
The practical, evidence-aligned steps for the general public are simple and low-effort:
- Don't let bottled water get hot. Heat is the strongest driver of antimony migration, so avoid leaving plastic bottles in hot cars, in direct sun, or near heat sources.
- Don't store bottled water for long periods. Antimony rises with storage time; drink it reasonably fresh rather than stockpiling cases for months or years.
- Prefer glass or stainless steel for water you carry or store routinely — these contain no antimony catalyst to leach.
- Keep perspective. For most people drinking cool, reasonably fresh bottled water, antimony intake stays well below WHO and EPA guidance values. This is a habit worth optimizing, not a crisis.
Household and general environmental awareness
Antimony trioxide is a common flame retardant in upholstered furniture, mattresses, and electronics, and is present in some older glassware and pigments. Ordinary use poses little risk, but avoid burning treated materials or sanding antimony-containing items without protection. As with arsenic and other toxic metals, a varied diet, good general nutrition, and avoiding unnecessary exposures form a sensible baseline defense.
9. Related Topics
- Arsenic — antimony's periodic-table neighbor and closest toxicological analogue; nearly identical thiol-binding and oxidative mechanisms, and the source of most antimony treatment strategies.
- Lead — alloyed with antimony in lead-acid batteries, a shared occupational exposure setting and a stibine-generation hazard.
- Mercury — another sulfhydryl-binding toxic metal managed with overlapping chelation approaches.
- Cadmium — an industrial toxic metal with chronic occupational lung and kidney effects paralleling antimony's.
- Heavy Metals — overview of the toxic-metal family, biomonitoring, and chelation principles.
- Anemia — the central consequence of stibine-induced intravascular hemolysis.
- Kidney Disease — acute kidney injury from hemoglobin released during antimony-driven hemolysis.
- Selenium — an essential antioxidant trace mineral; antioxidant status is part of the body's defense against metal-induced oxidative stress.
- Zinc — an essential metal whose binding sites and homeostasis can be perturbed by toxic-metal exposure.
- Lab Tests — how blood and urine biomonitoring tests (including urine antimony) are ordered and interpreted.
- All Minerals — the full minerals section, essential and toxic.
10. Key Research Papers
- Sundar S, Chakravarty J. Antimony toxicity. International Journal of Environmental Research and Public Health. 2010;7(12):4267–4277.
- Cooper RG, Harrison AP. The exposure to and health effects of antimony. Indian Journal of Occupational and Environmental Medicine. 2009;13(1):3–10.
- Sundar S. Drug resistance in Indian visceral leishmaniasis. Tropical Medicine & International Health. 2001;6(11):849–854.
- Chulay JD, Spencer HC, Mugambi M. Electrocardiographic changes during treatment of leishmaniasis with pentavalent antimony (sodium stibogluconate). American Journal of Tropical Medicine and Hygiene. 1985;34(4):702–709.
- Ribeiro AL, Drummond JB, Volpini AC, Andrade AC, Passos VM. Electrocardiographic changes during low-dose, short-term therapy of cutaneous leishmaniasis with the pentavalent antimonial meglumine. Brazilian Journal of Medical and Biological Research. 1999;32(3):297–301.
- Gasser RA Jr, Magill AJ, Oster CN, Franke ED, Grögl M, Berman JD. Pancreatitis induced by pentavalent antimonial agents during treatment of leishmaniasis. Clinical Infectious Diseases. 1994;18(1):83–90.
- Westerhoff P, Prapaipong P, Shock E, Hillaireau A. Antimony leaching from polyethylene terephthalate (PET) plastic used for bottled drinking water. Water Research. 2008;42(3):551–556.
- Welle F, Franz R. Migration of antimony from PET bottles into beverages: determination of the activation energy of diffusion and migration modelling compared with literature data. Food Additives & Contaminants: Part A. 2010;28(1):115–126.
- Shotyk W, Krachler M. Contamination of bottled waters with antimony leaching from polyethylene terephthalate (PET) increases upon storage. Environmental Science & Technology. 2007;41(5):1560–1563.
- Bailly R, Lauwerys R, Buchet JP, Mahieu P, Konings J. Experimental and human studies on antimony metabolism: their relevance for the biological monitoring of workers exposed to inorganic antimony. British Journal of Industrial Medicine. 1991;48(2):93–97.
- Iavicoli I, Caroli S, Alimonti A, Petrucci F, Carelli G. Biomonitoring of a worker population exposed to low antimony trioxide levels. Journal of Trace Elements in Medicine and Biology. 2002;16(1):33–39.
- Frézard F, Demicheli C, dos Santos Ferreira C, Costa MAP. Glutathione-induced conversion of pentavalent antimony to trivalent antimony in meglumine antimoniate. Antimicrobial Agents and Chemotherapy. 2001;45(3):913–916.
- Potkonjak V, Pavlovich M. Antimoniosis: a particular form of pneumoconiosis. I. Etiology, clinical and X-ray findings. International Archives of Occupational and Environmental Health. 1983;51(3):199–207.
- Newton PE, Bolte HF, Daly IW, Pillsbury BD, Terrill JB, Drew RT, Ben-Dyke R, Sheldon AW, Rubin LF. Subchronic and chronic inhalation toxicity of antimony trioxide in the rat. Fundamental and Applied Toxicology. 1994;22(4):561–576.
- Agency for Toxic Substances and Disease Registry (ATSDR). Toxicological Profile for Antimony and Compounds. U.S. Department of Health and Human Services, Public Health Service; 2019. ATSDR Tox Profile (PDF).
- World Health Organization. Antimony in Drinking-water — Background document for development of WHO Guidelines for Drinking-water Quality. WHO; provisional guideline value 0.020 mg/L. WHO background document.
- International Agency for Research on Cancer (IARC). Antimony trioxide and antimony trisulfide. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, Volume 47; 1989 (antimony trioxide classified Group 2B). IARC Monograph Vol. 47.
- U.S. Environmental Protection Agency (EPA). National Primary Drinking Water Regulations — Antimony (MCL 0.006 mg/L). EPA NPDWR.
Connections
- Arsenic
- Lead
- Mercury
- Cadmium
- Heavy Metals
- Selenium
- Zinc
- Anemia
- Kidney Disease
- Lab Tests
- All Minerals
- Leishmaniasis — the sandfly-borne parasitic disease treated with pentavalent antimonial drugs.