Leishmaniasis
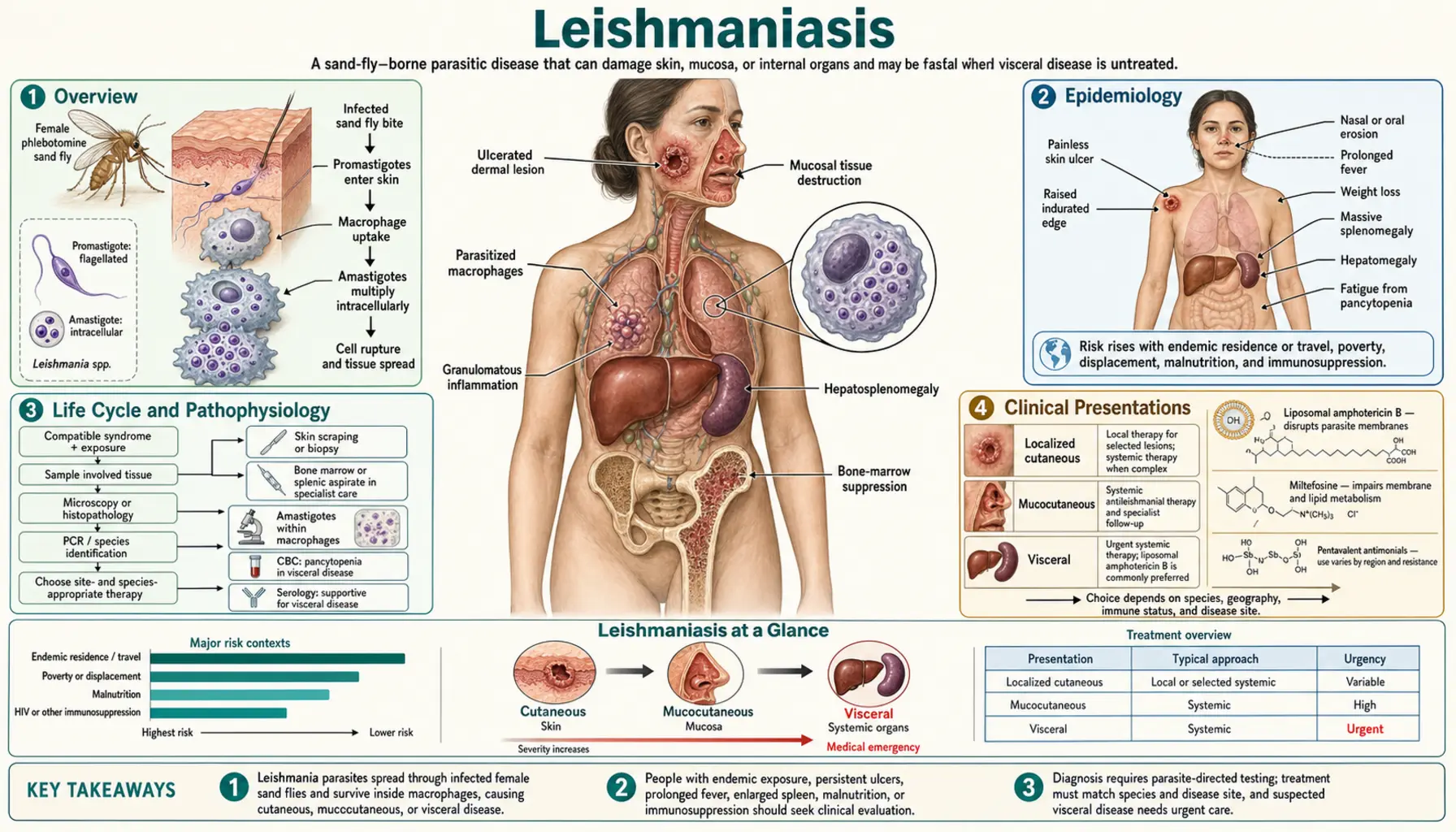
Table of Contents
- Overview
- Epidemiology
- Life Cycle and Pathophysiology
- Clinical Presentations
- Diagnosis
- Treatment
- Complications
- Prevention
- Research and Advances
- References
- PubMed Searches
- Connections
- Featured Videos
Overview
Leishmaniasis is a vector-borne parasitic disease caused by more than 20 species of the protozoan genus Leishmania. It is transmitted to humans through the bite of infected female sandflies — Phlebotomus species in the Old World (Europe, Africa, Asia) and Lutzomyia species in the New World (the Americas). The disease presents in three major clinical forms: cutaneous leishmaniasis (CL), mucocutaneous leishmaniasis (MCL), and visceral leishmaniasis (VL), also known as kala-azar.
Leishmaniasis ranks as the second most deadly parasitic disease worldwide after malaria. Approximately one billion people live in areas at risk for infection across 98 endemic countries. The World Health Organization (WHO) estimates 700,000 to one million new cases occur each year, with up to 30,000 deaths annually from visceral disease. The WHO classifies leishmaniasis as a neglected tropical disease (NTD), reflecting its disproportionate burden on the world's poorest populations.
Despite its global burden, leishmaniasis remains underfunded and underreported. Many cases go undiagnosed in resource-limited settings, and treatment options — while effective — carry significant toxicity risks. No licensed human vaccine currently exists, making vector control and early diagnosis central to disease management.
Epidemiology
The epidemiology of leishmaniasis varies sharply by clinical form and geographic region.
Visceral leishmaniasis (kala-azar) accounts for approximately 50,000–90,000 new cases per year globally, with about 90% concentrated in just six countries: India, Bangladesh, Nepal, Sudan, Ethiopia, and Brazil. The Indian subcontinent carries the highest burden, where L. donovani is the predominant species. In East Africa, L. donovani is also responsible, while in South America L. chagasi (now considered synonymous with L. infantum) is the primary species, with domestic dogs serving as a major reservoir.
Cutaneous leishmaniasis is far more common, with 600,000 to one million new cases per year. It occurs across three broad geographic zones: the Americas (primarily L. braziliensis and L. amazonensis), the Middle East and Central Asia (L. major in arid zones), and the Mediterranean basin and Western Asia (L. tropica in urban settings). Afghanistan, Algeria, Colombia, and Brazil together account for a large proportion of cases.
Mucocutaneous leishmaniasis occurs almost exclusively in South America and is caused primarily by L. braziliensis. It affects roughly 1–10% of CL cases caused by this species.
Key risk factors include poverty, malnutrition (which suppresses the immune response needed to control infection), deforestation and urbanization (which bring humans closer to sandfly habitats), and displacement due to conflict. HIV coinfection dramatically worsens outcomes — visceral leishmaniasis becomes an AIDS-defining illness and greatly increases mortality and relapse rates. Travelers to endemic regions — military personnel, ecotourists, and aid workers — are at increasing risk.
Life Cycle and Pathophysiology
The Leishmania parasite alternates between two hosts and two morphological forms during its life cycle.
In the sandfly vector: When a female sandfly takes a blood meal from an infected mammal, it ingests amastigotes (the intracellular, non-flagellated form found in host tissue). Inside the sandfly midgut, amastigotes transform into promastigotes — elongated, flagellated, and highly motile forms. These promastigotes multiply and migrate to the sandfly's proboscis. When the sandfly feeds again, it injects promastigotes along with its saliva into the host's dermis.
In the mammalian host: Promastigotes are quickly recognized and engulfed by host macrophages and dendritic cells at the bite site. Inside the macrophage phagolysosome — an acidic, enzyme-rich compartment designed to destroy pathogens — Leishmania promastigotes transform into amastigotes. Rather than being destroyed, amastigotes have evolved mechanisms to neutralize lysosomal enzymes, inhibit phagolysosome acidification, and evade the respiratory burst. They replicate within the phagolysosome until the macrophage ruptures, releasing amastigotes to infect neighboring macrophages, dendritic cells, and monocytes.
Immune response and disease outcome: The balance between Th1 and Th2 immune responses largely determines whether infection is controlled or progresses to disease. A robust Th1 response — characterized by interferon-gamma (IFN-γ) and tumor necrosis factor-alpha (TNF-α) production — activates macrophages to kill intracellular parasites via nitric oxide and reactive oxygen species. This response is associated with healing and resistance. A Th2-dominant response — with interleukin-4 (IL-4), IL-10, and IL-13 — suppresses macrophage killing activity, promotes parasite survival, and permits dissemination. IL-10 in particular plays a central role in parasite persistence.
In visceral leishmaniasis, parasites disseminate through the reticuloendothelial system to the liver (Kupffer cells), spleen, and bone marrow. Massive immune activation leads to hypergammaglobulinemia (elevated IgG, IgM, IgA) and hypersplenism. Paradoxically, antigen-specific T-cell responses are suppressed even while non-specific B-cell activation is exuberant.
In mucocutaneous leishmaniasis, tissue destruction is driven not by unchecked parasite growth but by a dysregulated, excessive immune response — macrophages and T cells cause collateral damage to mucosal tissue while attempting to eliminate residual parasites.
Clinical Presentations
Cutaneous Leishmaniasis (CL)
Cutaneous leishmaniasis is the most common form and presents days to weeks after the sandfly bite. The initial lesion is a painless papule that enlarges into a nodule and then ulcerates. The classic ulcer has a well-defined, raised, indurated border surrounding a clean base with granulation tissue — often described as a "volcano crater" appearance. In Latin America, lesions on the ear or face caused by L. braziliensis are called "chiclero ulcer." Lesions may be single or multiple, depending on the number of infectious bites and species involved.
Regional lymphadenopathy is common. Without treatment, lesions caused by many species (such as L. major) heal spontaneously within 2 months to 2 years, leaving a depressed scar. However, L. braziliensis infections carry a risk of progressing to mucocutaneous disease and should always be treated systemically. L. tropica and L. donovani can cause chronic non-healing CL.
Mucocutaneous Leishmaniasis (MCL)
Mucocutaneous leishmaniasis, caused primarily by L. braziliensis, develops months to years after the original cutaneous lesion. Parasites spread hematogenously from the skin to the mucosal membranes. The nasal mucosa is typically affected first, with congestion, epistaxis (nosebleeds), and progressive destruction of the nasal septum. Without treatment, the infection spreads to the palate, pharynx, and larynx.
Advanced MCL produces the characteristic "tapir nose" — collapse and saddle deformity of the nasal bridge from septal destruction. Severe disease causes disfigurement and can compromise the airway, leading to aspiration pneumonia and death. Crucially, MCL is driven in part by an excessive immune response: patients often have high parasite-specific T-cell responses, yet tissue destruction continues. This makes MCL difficult to treat and prone to relapse.
Visceral Leishmaniasis (VL / Kala-Azar)
The term "kala-azar" derives from the Hindi for "black fever," a reference to the dark hyperpigmentation of the skin — particularly on the face, hands, and abdomen — seen in some patients. VL has an insidious onset, with symptoms developing over weeks to months after infection. The hallmark features are:
- Prolonged fever — characteristically undulating, often with two daily temperature spikes
- Progressive massive splenomegaly — the spleen can enlarge dramatically, sometimes reaching the pelvis
- Hepatomegaly — less dramatic than splenomegaly but consistently present
- Weight loss and wasting — severe cachexia in advanced disease
- Pancytopenia — anemia, leukopenia, and thrombocytopenia from hypersplenism and bone marrow suppression
- Hypoalbuminemia — contributes to edema and ascites in severe cases
- Hypergammaglobulinemia — non-specific B-cell activation produces elevated immunoglobulins
Left untreated, visceral leishmaniasis is almost uniformly fatal — mortality approaches 95–100% within 2 years. Death is typically caused by secondary infections such as pneumonia, tuberculosis, or dysentery, rather than by direct parasite damage. Profound immunosuppression leaves patients unable to mount an effective defense against these opportunistic pathogens.
Post-Kala-Azar Dermal Leishmaniasis (PKDL)
PKDL is a delayed complication that develops after apparently successful treatment of visceral leishmaniasis. It is most common in India, where up to 10–20% of treated VL patients develop it, and in Sudan. PKDL presents as hypopigmented (and sometimes hyperpigmented) macules that progress to nodules and plaques, predominantly on the face, trunk, and extremities. PKDL patients harbor viable parasites in skin lesions and serve as an important reservoir for ongoing sandfly transmission — making treatment not only a clinical priority but a public health imperative.
Diagnosis
Diagnosis of leishmaniasis combines clinical judgment with laboratory confirmation, and the approach differs by clinical form.
Cutaneous Leishmaniasis
- Giemsa-stained smear or touch preparation from the lesion edge: sensitivity 50–70%; simple and inexpensive but operator-dependent
- Culture on NNN (Novy-MacNeal-Nicolle) medium: specific but slow (2–4 weeks) and requires specialized laboratory
- PCR on lesion biopsy: most sensitive (~95%) and can identify species — the preferred method where available
- Punch biopsy with histopathology: demonstrates granulomatous inflammation and intracellular amastigotes (Leishman-Donovan bodies) within macrophages
- Montenegro skin test (leishmanin test): intradermal injection of killed promastigotes; a positive DTH response indicates prior or current exposure but is not useful for diagnosing active VL (anergic in acute disease)
Visceral Leishmaniasis
- Splenic aspirate smear: highest sensitivity (93–99%) and the gold standard in reference centers, but carries a real risk of hemorrhage (0.1–0.5% fatality) — requires expert hands and surgical backup
- Bone marrow aspirate: sensitivity 53–86%, considerably safer than splenic aspiration; the preferred invasive method at most centers
- rK39 rapid diagnostic test (RDT): immunochromatographic strip detecting antibodies against the recombinant K39 antigen; sensitivity ~93.9%, specificity ~95.3% in South Asia and East Africa; less reliable in South America (Brazil) and Europe; inexpensive and easy to perform at the point of care
- PCR on peripheral blood or bone marrow: sensitivity >90% for active VL; also useful for monitoring treatment response and detecting relapse
- ELISA for anti-leishmania antibodies: useful for epidemiological studies and confirmation; cross-reactivity with Chagas disease limits specificity in South America
- Complete blood count: pancytopenia is a consistent finding and strongly supports the diagnosis in a febrile patient from an endemic area
- Aldehyde (formol-gel) test: historical non-specific test based on hypergammaglobulinemia; positive result indicates protein >3 g/dL; no longer recommended as a standalone diagnostic
Treatment
Treatment decisions for leishmaniasis depend on the clinical form, the infecting Leishmania species, the geographic region, and the patient's immune status. No single drug is universally applicable.
Cutaneous Leishmaniasis — Self-Healing Species
For CL caused by species with a tendency to self-heal (e.g., L. major, L. mexicana), treatment is guided by lesion size, number, location, and patient preference. Small, uncomplicated lesions may be observed. Local treatment options include intralesional injections of pentavalent antimonials (Sbv), cryotherapy with liquid nitrogen, or thermotherapy (localized heat application at 50°C for 30 seconds). Systemic therapy is indicated for multiple or large lesions, facial lesions, or immunocompromised patients.
Cutaneous Leishmaniasis — L. braziliensis (MCL Risk)
All cases of CL caused by L. braziliensis should receive systemic treatment to prevent progression to mucocutaneous disease. First-line options include:
- Miltefosine (oral): 2.5 mg/kg/day × 28 days; teratogenic — contraindicated in pregnancy; gastrointestinal side effects common
- Meglumine antimoniate (Glucantime) or sodium stibogluconate (Pentostam): 20 mg/kg/day intramuscularly × 20 days; pentavalent antimonials (Sbv) have been first-line for decades but carry significant toxicity (see below)
Established MCL requires higher doses of Sbv for 30 days. Sbv-refractory MCL is treated with liposomal amphotericin B or conventional amphotericin B deoxycholate.
Visceral Leishmaniasis — First-Line by Region
South Asia (India, Bangladesh, Nepal): Single-dose liposomal amphotericin B (AmBisome) at 10 mg/kg intravenously achieves cure rates exceeding 95% with excellent tolerability. This is now the WHO-recommended first-line treatment for the Indian subcontinent and represents a major therapeutic advance. Alternatives include miltefosine (2.5 mg/kg/day × 28 days), paromomycin (11 mg/kg/day IM × 21 days), or combination regimens to shorten treatment duration and reduce resistance pressure.
East Africa: Liposomal amphotericin B (3 mg/kg on days 1–5, 14, and 21, totaling 21 mg/kg) is recommended. Alternatively, Sbv (20 mg/kg/day × 30 days) remains in use where monitoring permits, or combination Sbv plus paromomycin for 17 days. Due to variable Sbv efficacy in different African regions, treatment is often guided by national programs.
South America: Sbv (20 mg/kg/day × 30 days) remains the standard of care, given lower resistance rates and limited availability of liposomal AmB. Liposomal AmB is used for treatment failures.
Toxicity of Pentavalent Antimonials (Sbv)
Sbv drugs (meglumine antimoniate, sodium stibogluconate) are highly effective but carry serious toxicity risks that require monitoring:
- Cardiotoxicity: QTc prolongation and T-wave changes are common; potentially fatal arrhythmias can occur — ECG monitoring before and during treatment is mandatory
- Pancreatitis: Elevated serum amylase/lipase occurs in up to 100% of treated patients; clinical pancreatitis is less common but can be severe
- Hepatotoxicity: Elevated transaminases; liver function tests must be monitored
- Nephrotoxicity: Dose-dependent renal impairment; creatinine monitoring required
- Contraindicated in pregnancy, significant hepatic or renal disease, and cardiac conduction abnormalities
HIV-Leishmaniasis Coinfection
HIV-VL coinfection demands aggressive treatment and long-term secondary prophylaxis. Liposomal amphotericin B is the treatment of choice. Following successful treatment, monthly liposomal AmB (3–5 mg/kg) is given as secondary prophylaxis until CD4 counts rise above 200 cells/μL on antiretroviral therapy (ART). Despite treatment, relapse rates exceed 50% in HIV-coinfected patients, and atypical presentations (involving unusual anatomical sites such as the GI tract, lungs, or skin) are common. The prognosis remains significantly worse than in immunocompetent patients.
Complications
Leishmaniasis — particularly the visceral form — carries a spectrum of potentially life-threatening complications:
- Massive splenomegaly: The dramatically enlarged spleen is susceptible to spontaneous rupture from minor abdominal trauma, causing intra-abdominal hemorrhage. Hypersplenism drives the pancytopenia that characterizes VL.
- Secondary bacterial infections: Profound immunosuppression and neutropenia leave patients vulnerable to pneumonia, tuberculosis, enteric infections (typhoid, dysentery), and septicemia. These opportunistic infections are the most common proximate cause of death in untreated VL.
- Hemorrhage: Thrombocytopenia plus the coagulopathy of hepatic dysfunction creates significant bleeding risk — epistaxis, gingival bleeding, and gastrointestinal hemorrhage are all documented.
- Hepatic failure: Severe hepatomegaly with hepatocyte damage can progress to liver failure in advanced or prolonged VL, compounding coagulopathy.
- MCL airway compromise: Progressive destruction of the pharynx and larynx in MCL can narrow the airway to a critical degree, causing aspiration pneumonia or respiratory failure.
- PKDL as transmission reservoir: Post-kala-azar dermal leishmaniasis perpetuates sandfly transmission within communities, contributing to ongoing endemic cycles — a public health complication as much as a clinical one.
- Drug toxicity: Treatment itself carries risks of cardiotoxicity (Sbv), nephrotoxicity (conventional amphotericin B), and gastrointestinal disturbance (miltefosine), which may limit treatment options in patients with comorbidities.
Prevention
There is currently no licensed vaccine for human leishmaniasis, placing the burden of prevention on personal protection, vector control, and reservoir management.
Personal protection measures:
- Insect repellents containing DEET (20–50%) applied to exposed skin are effective against sandflies, which are most active at dusk and dawn
- Permethrin-treated clothing (long sleeves, trousers tucked into socks) reduces bite exposure
- Fine-mesh bed nets (at minimum 25 holes/cm²) impregnated with permethrin — standard mosquito nets have too large a mesh for sandflies, which are roughly 2–3 mm in length and can pass through
- Air-conditioned or well-screened accommodations reduce exposure in endemic areas
Vector control:
- Indoor residual spraying (IRS) with insecticides (DDT, pyrethroids) targets adult sandflies resting on walls
- Environmental modification: removing rubble, leaf litter, animal burrows, and vegetation near dwellings disrupts sandfly breeding and resting sites
- Large-scale IRS campaigns in the Indian subcontinent, implemented as part of WHO's kala-azar elimination program, have achieved significant reductions in VL incidence
Reservoir control:
- In zoonotic settings (South America, Mediterranean), domestic dogs are the primary reservoir for L. infantum/chagasi. Dog culling programs have historically been used but are controversial and largely ineffective; dog collars impregnated with deltamethrin significantly reduce sandfly feeding on dogs and transmission to humans
- Vaccinating dogs (a veterinary Leishmania vaccine, Letifend, is licensed in Europe) reduces the canine reservoir burden
Traveler guidance: Travelers to endemic regions should apply DEET repellent, wear permethrin-treated clothing, use fine-mesh bed nets, and sleep in screened accommodations. No chemoprophylaxis regimen is available. Any traveler returning with a skin ulcer that does not heal within 2–4 weeks after visiting an endemic area should be evaluated for cutaneous leishmaniasis.
Research and Advances
Leishmaniasis research has accelerated in recent years, driven in part by the Drugs for Neglected Diseases initiative (DNDi) and international partnerships committed to eliminating VL from the Indian subcontinent by 2030.
New drug candidates:
- Fexinidazole: An oral nitroimidazole drug developed by DNDi, originally approved for sleeping sickness; Phase II clinical trials for VL are underway and early results are encouraging
- Combination therapy: Using two drugs at lower doses (e.g., AmB + miltefosine, or miltefosine + paromomycin) shortens treatment duration, reduces toxicity, and may delay emergence of resistance — a core strategy in the WHO elimination campaign
- LXE408: An oral antileishmanial compound in early clinical development targeting the proteasome
Vaccine development:
- LEISH-F3+GLA-SE: A recombinant polyprotein antigen with a TLR4 agonist adjuvant; completed Phase 1 trials with acceptable safety and immunogenicity
- ChAd63/MVA-KH: A viral-vectored prime-boost vaccine in Phase 2 trials in Sudan; designed to induce a strong Th1 (IFN-γ) cellular immune response — the correlate of protection
- First-generation killed-parasite vaccines (e.g., Leishvax) are being tested in combination with adjuvants
Drug resistance mechanisms:
- Miltefosine resistance has emerged in South Asia and is associated with reduced intracellular drug accumulation mediated by overexpression of ABC transporters and downregulation of the miltefosine transporter (LdMT-LdRos3 complex)
- Sbv resistance in the Indian subcontinent (Bihar state) is widespread; genetic studies using whole-genome sequencing have identified resistance-associated single nucleotide polymorphisms in the L. donovani genome
- CRISPR-Cas9 gene editing is being applied to systematically validate drug resistance genes and identify new therapeutic targets
Diagnostics:
- Loop-mediated isothermal amplification (LAMP) assays for Leishmania are being developed as rapid, low-cost molecular diagnostics suitable for field use without sophisticated laboratory equipment
- Multiplexed lateral flow assays combining rK39 with other antigens may improve specificity in regions where cross-reactivity with Chagas disease is a concern
References
- Alvar J, Vélez ID, Bern C, et al. Leishmaniasis worldwide and global estimates of its incidence. PLoS One. 2012;7:e35671. DOI: 10.1371/journal.pone.0035671 — PMID 22693548
- Bern C, Maguire JH, Alvar J. Complexities of assessing the disease burden attributable to leishmaniasis. PLoS Negl Trop Dis. 2008;2:e313. DOI: 10.1371/journal.pntd.0000313 Search PubMed
- Sundar S, Rai M. Laboratory diagnosis of visceral leishmaniasis. Clin Diagn Lab Immunol. 2002;9:951–958. DOI: 10.1128/CDLI.9.5.951-958.2002 Search PubMed
- Reithinger R, Dujardin JC, Louzir H, et al. Cutaneous leishmaniasis. Lancet Infect Dis. 2007;7:581–596. DOI: 10.1016/S1473-3099(07)70209-8 Search PubMed
- Sundar S, Chakravarty J. Leishmaniasis: an update of current pharmacotherapy. Expert Opin Pharmacother. 2013;14:53–63. DOI: 10.1517/14656566.2013.755022 — PMID 23256501
- Bhattacharya SK, Sur D, Sinha PK, et al. Elimination of kala-azar and post-kala-azar dermal leishmaniasis in the Indian subcontinent. Bull World Health Organ. 2006;84:816–824. DOI: 10.2471/blt.05.031997 Search PubMed
- Bern C, Adler-Moore J, Berenguer J, et al. Liposomal amphotericin B for the treatment of visceral leishmaniasis. Clin Infect Dis. 2006;43:917–924. DOI: 10.1086/507530 Search PubMed
- Croft SL, Sundar S, Fairlamb AH. Drug resistance in leishmaniasis. Clin Microbiol Rev. 2006;19:111–126. DOI: 10.1128/CMR.19.1.111-126.2006 Search PubMed
- Murray HW, Berman JD, Davies CR, et al. Advances in leishmaniasis. Lancet. 2005;366:1561–1577. DOI: 10.1016/S0140-6736(05)67629-5 Search PubMed
- Desjeux P. Leishmaniasis: current situation and new perspectives. Comp Immunol Microbiol Infect Dis. 2004;27:305–318. DOI: 10.1016/j.cimid.2004.03.004 — PMID 15225981
- Chappuis F, Sundar S, Hailu A, et al. Visceral leishmaniasis: what are the needs for diagnosis, treatment and control? Nat Rev Microbiol. 2007;5:873–882. DOI: 10.1038/nrmicro1748 — PMID 17938629
- Goto H, Lindoso JA. Current diagnosis and treatment of cutaneous and mucocutaneous leishmaniasis. Expert Rev Anti Infect Ther. 2010;8:419–433. DOI: 10.1586/eri.10.19 — PMID 20377337
PubMed Searches
The following PubMed search links provide access to the latest peer-reviewed research on leishmaniasis:
- Visceral leishmaniasis treatment
- Cutaneous leishmaniasis diagnosis
- Mucocutaneous leishmaniasis L. braziliensis
- Liposomal amphotericin B for kala-azar
- Leishmaniasis HIV coinfection
- Post-kala-azar dermal leishmaniasis (PKDL)
- Leishmaniasis vaccine clinical trials
- Miltefosine resistance in leishmaniasis
Connections
- Infectious Disease
- Toxoplasmosis
- Rocky Mountain Spotted Fever
- HIV/AIDS
- Lyme Disease
- Dengue Fever
- Immune Boosting
- Typhoid Fever
- Malaria
- Iron
- Leishmania: Sandfly-Borne Parasite — the parasite hub with symptom and treatment deep dives.
- Leishmania Symptoms: Three Faces of a Global Disease — cutaneous, mucocutaneous, and visceral presentations compared.
- Cutaneous and Mucosal Leishmaniasis — skin ulcers, espundia, and the species behind each form.
- Diagnosing Leishmaniasis: Microscopy, PCR, and Rapid Tests — how the diagnosis is confirmed and why species identification changes treatment.
- Visceral Leishmaniasis (Kala-Azar) — the fatal systemic form: prolonged fever, massive splenomegaly, pancytopenia, and PKDL.
- Leishmaniasis Treatments — liposomal amphotericin B, miltefosine, antimonials, and vector control.
- Antimony — the toxic metalloid behind sodium stibogluconate and meglumine antimoniate, and their cardiac and pancreatic side effects.