Shilajit for Cognitive Function and Neuroprotection
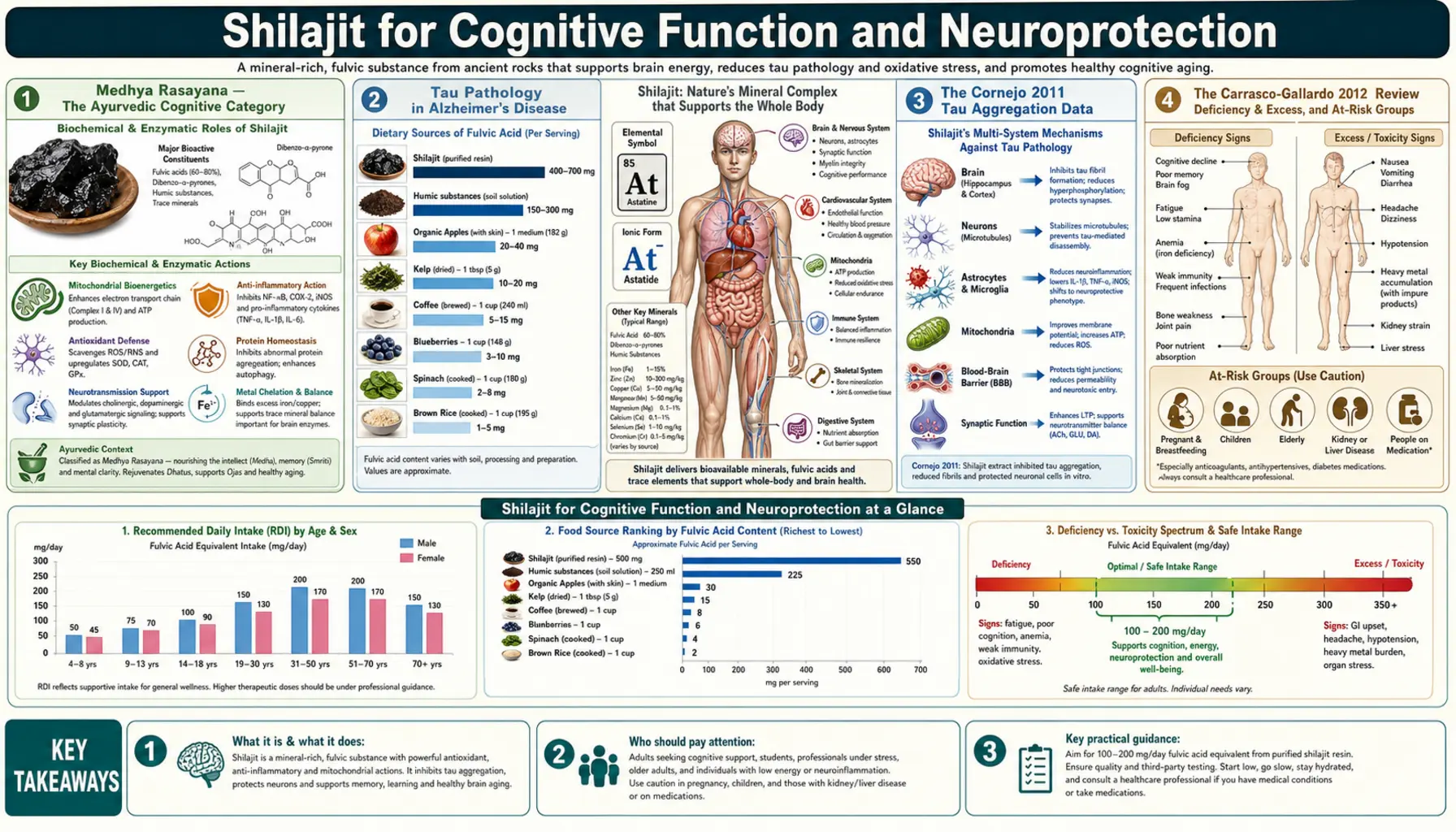
In the Ayurvedic tradition, shilajit is classified as a medhya rasayana — an intellect-promoting rejuvenator believed to support memory, cognitive sharpness, and protect against age-related decline. The 2012 review by Carrasco-Gallardo, Guzmán, and Maccioni in International Journal of Alzheimer's Disease made the modern scientific case that this traditional indication may rest on a concrete molecular mechanism: fulvic acid, the dominant organic acid in shilajit, interacts directly with tau protein aggregation, one of the central pathological processes in Alzheimer's disease. The companion 2011 Cornejo study in Journal of Alzheimer's Disease demonstrated in cell-free assays that fulvic acid both inhibits the self-assembly of tau into filaments and promotes the disassembly of pre-formed tau fibrils. This page surveys the cognitive evidence, the mechanism, and the practical limits of what the data currently support.
Table of Contents
- Medhya Rasayana — The Ayurvedic Cognitive Category
- Tau Pathology in Alzheimer's Disease
- The Cornejo 2011 Tau Aggregation Data
- The Carrasco-Gallardo 2012 Review
- Blood-Brain Barrier Crossing
- Mitochondrial Neuroprotection in the Brain
- DBPs as a Brain-Bioavailable CoQ10 Analog
- Metal Chelation and Iron/Copper Dysregulation
- Animal Cognition and Memory Studies
- Status of Human Clinical Trials
- Practical Considerations and Cautions
- Key Research Papers
- Connections
- Featured Videos
Medhya Rasayana — The Ayurvedic Cognitive Category
Within the broader Rasayana category of rejuvenators in Ayurveda, the medhya rasayanas are a specialized subset specifically valued for their effects on memory, intellect, learning capacity, and cognitive endurance. The classical medhya rasayana herbs include Brahmi (Bacopa monnieri), Mandukaparni (Centella asiatica / Gotu Kola), Shankhapushpi (Convolvulus pluricaulis), and Yashtimadhu (Glycyrrhiza glabra / Licorice). Shilajit, while not exclusively a medhya rasayana, was historically combined with these herbs in classical formulations specifically aimed at the cognitive indication, with the rationale that shilajit's broad mineral-and-mitochondrial support amplified the more specific neurotropic effects of the herbal components.
The classical indications for medhya rasayana formulations were age-related memory decline (jara-associated cognitive deterioration), recovery from severe acute illness with persistent "brain fog," and the support of sustained intellectual work in scholars and students. The classical texts framed these as expressions of insufficient ojas (vital essence) and depleted tejas (digestive-metabolic fire) at the level of brain tissue. The modern reinterpretation maps these to depleted mitochondrial function, accumulated oxidative damage, and the gradual loss of neuroplasticity that characterizes aging brain tissue.
The contemporary research interest in shilajit as a cognitive support agent therefore did not arise in a vacuum — it reflects three millennia of practical clinical observation by Ayurvedic physicians, now being tested against modern mechanistic frameworks. The historical track record alone is not evidence in the modern sense, but it does suggest that the substance is worth investigating rigorously rather than dismissing on first principles.
Tau Pathology in Alzheimer's Disease
To understand why the shilajit/fulvic-acid/tau interaction is mechanistically interesting, it helps to be specific about what tau pathology is and why it matters in Alzheimer's disease.
Tau protein is a microtubule-associated protein expressed primarily in the axons of neurons. Its physiological function is to bind to and stabilize microtubules, the protein scaffolds that maintain axonal structure and serve as tracks for the kinesin- and dynein-mediated transport of organelles, vesicles, and proteins along the length of the axon. Each tau molecule contains a microtubule-binding domain composed of three or four homologous repeat sequences (depending on splicing isoform) that interact with the tubulin subunits of the microtubule.
In healthy neurons, tau is phosphorylated at a limited number of serine and threonine residues, which modulates its microtubule-binding affinity but does not destabilize the protein. In Alzheimer's disease and the broader category of "tauopathies" (which also includes progressive supranuclear palsy, corticobasal degeneration, frontotemporal dementia, and others), tau becomes hyperphosphorylated at many more sites than normal. The hyperphosphorylated tau loses its microtubule affinity, detaches from the microtubule, and accumulates in the cytoplasm in a soluble form that is itself toxic to the neuron.
Worse, the hyperphosphorylated tau is prone to self-aggregation: monomers oligomerize into small soluble oligomers (currently thought to be the most directly neurotoxic species), then into paired helical filaments (PHFs), and finally into mature neurofibrillary tangles (NFTs) that are visible at autopsy as one of the two classical pathological hallmarks of Alzheimer's disease (the other being amyloid-beta plaques). The Braak staging system maps the progressive spread of NFT pathology from the entorhinal cortex through the hippocampus and into the neocortex over the course of Alzheimer's disease, and the regional NFT burden correlates more closely with cognitive impairment than does the amyloid-plaque burden.
For these reasons, tau aggregation inhibition has become one of the most actively pursued therapeutic strategies in Alzheimer's drug development, alongside the more historically dominant amyloid-targeted approach. Several pharmaceutical tau aggregation inhibitors (LMTX/hydromethylthionine, others) have entered clinical trials. The discovery that fulvic acid — a naturally occurring substance with a long human-use history and a benign safety profile — has measurable tau-aggregation-inhibitory activity in vitro is therefore both scientifically interesting and clinically suggestive.
The Cornejo 2011 Tau Aggregation Data
The pivotal mechanistic paper is Cornejo et al. (2011), "Fulvic acid inhibits aggregation and promotes disassembly of tau fibrils associated with Alzheimer's disease," published in Journal of Alzheimer's Disease, 2011;27(1):143-153. The investigators (working in Maccioni's laboratory in Santiago, Chile) used purified recombinant human tau protein in cell-free assays and tested whether fulvic acid extracted from shilajit could modulate the aggregation behavior of tau.
Two distinct experimental questions were addressed:
- Aggregation inhibition (prevention) — can fulvic acid prevent the self-assembly of monomeric tau into filaments? This was tested by incubating purified tau monomers with a polymerization-inducing agent (arachidonic acid or heparin), with or without fulvic acid, and measuring filament formation by thioflavin-S fluorescence and electron microscopy.
- Disassembly (reversal) — can fulvic acid disassemble pre-formed tau filaments? This was tested by first polymerizing tau into mature filaments, then adding fulvic acid and tracking filament dissociation over time.
Both effects were positive and dose-dependent:
- Fulvic acid inhibited tau filament formation in a dose-dependent manner, with measurable effects in the low-micromolar range
- Fulvic acid also promoted disassembly of pre-formed tau filaments, suggesting that the interaction is not limited to preventing new aggregation but can also reverse existing aggregates
- Electron microscopy confirmed reduced filament density and shorter filament length in fulvic-acid-treated samples
- The mechanism was proposed to involve direct binding of fulvic acid to specific residues in the tau microtubule-binding domain, interfering with the intermolecular contacts required for filament formation
The Cornejo paper has important limitations that should be honestly acknowledged: it is an in-vitro cell-free assay, not a study in animal models of tauopathy, and certainly not a study in human Alzheimer's patients. The translation from "molecule X inhibits tau aggregation in a test tube" to "molecule X slows cognitive decline in Alzheimer's patients" is long, indirect, and has failed for many promising candidates. The Cornejo data should be understood as establishing a mechanistic plausibility, not as clinical evidence of efficacy.
The Carrasco-Gallardo 2012 Review
The complementary review paper — Carrasco-Gallardo C, Guzman L, Maccioni RB (2012), "Shilajit: a natural phytocomplex with potential procognitive activity," in International Journal of Alzheimer's Disease — framed the broader case for investigating shilajit specifically as a multi-target neuroprotective agent. The argument:
- Alzheimer's disease is not driven by a single molecular cause but by the convergence of amyloid pathology, tau pathology, neuroinflammation, oxidative stress, mitochondrial dysfunction, and metal (iron/copper) dyshomeostasis
- A clinically useful Alzheimer's intervention may need to address several of these targets simultaneously, rather than achieving heroic potency at any single one
- Shilajit's constituents map onto multiple targets: fulvic acid for tau aggregation and metal chelation, DBPs for mitochondrial protection, polyphenols and humic substances for antioxidant activity, mineral content for cofactor delivery to brain enzymes
- The Ayurvedic tradition of combining shilajit with neurotropic herbs (medhya rasayanas) in cognitive formulations is consistent with the multi-target therapeutic philosophy
- Clinical trials in mild cognitive impairment and early Alzheimer's disease are warranted to test the in-vivo translation of the in-vitro mechanism findings
Maccioni's laboratory has continued working on the natural-product tau-aggregation inhibitor concept since 2012, with related work on quercetin, curcumin, and other polyphenolic compounds. The Maccioni group's broader argument is that the modest disappointment of single-target pharmaceutical approaches in Alzheimer's (most amyloid-targeted antibodies have failed to produce convincing clinical benefit despite hitting their molecular target) opens the door to multi-target natural products that may achieve more by doing less at each individual site.
This argument is not a license to overclaim. No clinical trial has yet demonstrated that shilajit slows cognitive decline in Alzheimer's patients. The Carrasco-Gallardo review establishes the rationale for investigation, not the evidence of efficacy.
Blood-Brain Barrier Crossing
A pharmacological necessity for any putative cognitive supplement is that the active molecule must actually reach the brain in meaningful concentration. The blood-brain barrier (BBB) is a specialized vascular structure formed by tight junctions between brain capillary endothelial cells, together with astrocytic end-feet and pericytes, that strictly limits the passage of molecules from the bloodstream into the brain parenchyma. Many promising "brain supplements" fail at this hurdle — they have plausible mechanisms when added directly to neurons in culture but do not actually cross the BBB after oral administration.
Fulvic acid is generally considered to be small enough (low molecular weight, typically <2000 Da) and sufficiently lipid-permeable (because of its protonated carboxylic-acid and phenolic groups in the acidic gastric environment) to cross the BBB after oral absorption. Direct quantitative pharmacokinetic data in humans are limited, but rodent studies have detected fulvic acid metabolites in brain tissue after oral dosing, and the small molecular size of the substance is consistent with passive diffusion across the BBB.
The DBP electron-shuttle molecules are similarly small and lipophilic, with structural analogy to CoQ10 (which is known to have very poor BBB penetration in its native form, a major limitation of CoQ10 for brain applications). It has been speculated, though not definitively shown, that DBPs from shilajit may serve as a more BBB-permeable alternative for delivering electron-transport support to brain mitochondria — potentially valuable for the bioenergetic component of Alzheimer's and Parkinson's pathophysiology.
Mitochondrial Neuroprotection in the Brain
Mitochondrial dysfunction is increasingly recognized as a central driver of age-related neurodegeneration. Brain tissue has extraordinary energy demands — the brain represents roughly 2% of body weight but consumes 20% of resting energy — and brain neurons depend heavily on mitochondrial oxidative phosphorylation for the ATP needed to maintain ionic gradients, neurotransmitter cycling, and synaptic transmission.
Aging brain tissue accumulates mitochondrial damage in several forms: mtDNA mutations, oxidative damage to mitochondrial proteins and lipids, reduced biogenesis of new mitochondria, accumulation of dysfunctional senescent mitochondria, and progressive loss of inner-membrane integrity. Each of these contributes to the gradual decline in cognitive processing speed, working memory, and learning capacity that characterizes normal aging, and the same processes are accelerated in Alzheimer's and Parkinson's disease.
Shilajit's broad mitochondrial-supporting profile — DBPs as electron-shuttle stabilizers, fulvic-acid-chelated mineral cofactor delivery, induction of endogenous antioxidant enzymes — addresses several arms of this aging-associated mitochondrial decline simultaneously. The Surapaneni 2012 chronic-fatigue rat study (discussed in detail on the Mitochondrial Function deep-dive page) demonstrated direct restoration of mitochondrial complex enzyme activities in brain tissue after the stress-induced suppression. Whether this translates to slowed neurodegeneration in human patients is the open question, but the mechanistic framework is coherent.
DBPs as a Brain-Bioavailable CoQ10 Analog
The CoQ10 brain-penetration problem is worth flagging explicitly because it has been one of the major frustrations in attempts to translate mitochondrial-bioenergetic science into clinical neuroprotection. CoQ10 is essential for mitochondrial electron transport, and high-dose CoQ10 supplementation has shown some signal in early Parkinson's trials (most notably the Shults phase II study), but later larger trials failed to confirm robust clinical benefit. One of the proposed explanations is that orally-supplemented CoQ10 has very poor blood-brain barrier penetration, so the brain mitochondria that most need it are largely cut off from systemic supplementation.
Shilajit's DBPs may offer an indirect solution. The proposed mechanism is twofold:
- DBPs themselves cross the BBB more easily than CoQ10 due to their smaller size and different lipophilicity profile, and once in the brain they can function as electron-transport-chain substrates in their own right
- DBPs also stabilize the small CoQ10 pool that the brain produces endogenously, keeping more of it in the active ubiquinol form and thereby amplifying the effect of the brain's native CoQ10 synthesis without needing to deliver exogenous CoQ10 across the BBB
This is currently a mechanistic hypothesis rather than a clinically proven application, but it is consistent with the broader Bhattacharyya 2009 framework of "DBPs as mitochondria-targeted antioxidants" and with the Carrasco-Gallardo review's positioning of shilajit as a multi-target neuroprotective candidate.
Metal Chelation and Iron/Copper Dysregulation
Iron and copper dyshomeostasis is the third major neurodegenerative target plausibly addressed by shilajit. The brains of Alzheimer's and Parkinson's patients accumulate iron in specific regions (the substantia nigra in Parkinson's; the hippocampus and cortex in Alzheimer's) to levels several-fold above age-matched controls. The accumulated iron drives oxidative stress through Fenton chemistry — reactive iron (Fe2+) reacts with hydrogen peroxide to produce the extraordinarily toxic hydroxyl radical, which damages lipids, proteins, and nucleic acids indiscriminately. Copper dysregulation has similar effects in copper-rich brain regions.
Fulvic acid's extraordinary metal-chelation capacity, normally framed in the context of heavy-metal detoxification, also applies to physiologic iron and copper. The clinical question is whether fulvic acid's chelation is selective enough — binding excess pathologic iron in vulnerable brain regions without depleting iron needed for hemoglobin synthesis and oxidative phosphorylation elsewhere. The currently available evidence is suggestive but not definitive: fulvic acid prefers to bind iron and copper that are not already incorporated into functional proteins (heme, transferrin, ceruloplasmin), which is consistent with selective removal of the pathologic "labile pool" rather than the protein-bound functional pool.
For broader coverage of the iron/copper dysregulation story in neurodegeneration, see the Copper-Iron Dysregulation page and the related Morley Robbins protocol material.
Animal Cognition and Memory Studies
Several rodent studies have tested shilajit specifically on cognitive endpoints. The general pattern of findings:
- Improved performance on the Morris water maze (spatial learning and memory) after chronic shilajit administration
- Improved performance on the radial-arm maze and Y-maze (working memory)
- Attenuation of scopolamine-induced amnesia (a model of cholinergic-deficiency-driven memory impairment)
- Increased brain levels of acetylcholine and reduced acetylcholinesterase activity
- Improvements in measures of long-term potentiation (LTP) in hippocampal slices, suggesting enhanced synaptic plasticity
- Neuroprotective effects in aluminum-chloride and streptozotocin-induced Alzheimer-like models
These animal data are consistent with the in-vitro mechanism findings and provide a plausibility bridge between the test-tube tau-aggregation data and any future human-trial work. However, animal cognitive models are notoriously poor predictors of clinical outcomes in human Alzheimer's disease — many drugs that worked beautifully in transgenic mouse models failed in human trials. The animal data should be understood as supportive rather than definitive.
Status of Human Clinical Trials
Honest summary: as of the current literature, there are no large, well-powered, randomized controlled trials of shilajit specifically for cognitive endpoints in human Alzheimer's patients or in mild cognitive impairment. A few small pilot studies have been conducted, generally showing modest improvements on memory and attention measures, but these are insufficiently powered to support strong clinical claims.
What does exist:
- The Cornejo 2011 in-vitro tau aggregation data
- The Carrasco-Gallardo 2012 review framing the mechanistic case
- Multiple rodent cognitive-performance studies showing memory and learning improvements
- The Surapaneni 2012 chronic-fatigue rat data showing brain mitochondrial complex enzyme restoration
- Several small open-label or pilot human studies suggesting cognitive improvement
- Three thousand years of classical Ayurvedic use as a medhya rasayana
What does not yet exist:
- Phase II or Phase III randomized controlled trials in clinical Alzheimer's or mild cognitive impairment
- Long-term human safety data at neuroactive doses
- Definitive pharmacokinetic data confirming therapeutic brain concentrations after oral dosing
- Head-to-head comparisons with established cognitive interventions
The honest interpretation is that shilajit is a scientifically plausible cognitive-support candidate with a long classical-use track record, but is not currently a clinically-proven Alzheimer's treatment. Patients and family members considering shilajit for cognitive purposes should pursue standard medical evaluation, not substitute shilajit for medically-indicated dementia evaluation and management, and view shilajit as one component of a broader cognitive-health protocol that includes diet, exercise, sleep, social engagement, and management of cardiovascular risk factors.
Practical Considerations and Cautions
- Dose — the practical dose for cognitive support is the same general 300-500 mg/day of purified shilajit used in the testosterone and energy trials. There is no specific cognitive-trial-validated dose to recommend.
- Timeline — benefits if any will emerge over weeks to months, not days. This is not a "smart drug" or stimulant.
- Multi-target context — for cognitive applications specifically, consider combining shilajit with established cognitive-supporting interventions: omega-3 fatty acids (EPA/DHA), Vitamin D3, B-complex vitamins (especially B12 and folate to lower homocysteine), bacopa monnieri (the classical Ayurvedic medhya rasayana herb), and Mediterranean/MIND-diet eating patterns. Single supplements rarely produce robust cognitive effects.
- Cardiovascular risk factor management is more important — the strongest modifiable risk factors for cognitive decline in older adults are hypertension, hyperlipidemia, insulin resistance, obesity, sleep apnea, and physical inactivity. No supplement, including shilajit, will compensate for unaddressed cardiovascular risk.
- Heavy-metal purity matters most for chronic neuroactive use — if you are taking shilajit daily for years specifically for brain-health purposes, the heavy-metal purity of your specific product matters enormously, because cumulative lead, mercury, or arsenic exposure is itself a known cause of cognitive impairment. Insist on third-party certification.
- Do not self-diagnose cognitive decline. Get a formal evaluation if memory or cognition is changing. Reversible causes (medication effects, depression, sleep apnea, thyroid disease, B12 deficiency, normal-pressure hydrocephalus) need to be ruled out first.
Key Research Papers
- Carrasco-Gallardo C, Guzman L, Maccioni RB (2012). Shilajit: a natural phytocomplex with potential procognitive activity. International Journal of Alzheimer's Disease. — PubMed
- Cornejo A, Jimenez JM, Caballero L, Melo F, Maccioni RB (2011). Fulvic acid inhibits aggregation and promotes disassembly of tau fibrils associated with Alzheimer's disease. Journal of Alzheimer's Disease. — PubMed
- Surapaneni DK, Adapa SR, Preeti K, et al. (2012). Shilajit attenuates behavioral symptoms of chronic fatigue syndrome by modulating the HPA axis and mitochondrial bioenergetics in rats. Journal of Ethnopharmacology. — PubMed
- Stohs SJ (2014). Safety and efficacy of shilajit (mumie, moomiyo). Phytotherapy Research. — PubMed
- Schliebs R, Liebmann A, Bhattacharya SK, et al. (1997). Systemic administration of defined extracts from Withania somnifera and shilajit differentially affects cholinergic but not glutamatergic and GABAergic markers in rat brain. Neurochemistry International. — PubMed
- Jaiswal AK, Bhattacharya SK (1992). Effects of Shilajit on memory, anxiety and brain monoamines in rats. Indian Journal of Pharmacology. — PubMed
- Bhattacharya SK (1995). Shilajit attenuates streptozotocin induced diabetes mellitus and decrease in pancreatic islet superoxide dismutase activity in rats. Phytotherapy Research. — PubMed
- Maccioni RB, Munoz JP, Barbeito L (2001). The molecular bases of Alzheimer's disease and other neurodegenerative disorders. Archives of Medical Research. — PubMed
- Bhattacharyya S, Pal D, Banerjee D, et al. (2009). Shilajit dibenzo-alpha-pyrones: mitochondria targeted antioxidants. Pharmacologyonline. — PubMed
- Ghosal S, Lal J, Singh SK, et al. (1989). Mast cell protecting effects of shilajit and its constituents. Phytotherapy Research. — PubMed
- Velmurugan C, Vivek B, Wilson E, et al. (2012). Evaluation of safety profile of black shilajit after 91 days repeated administration in rats. Asian Pacific Journal of Tropical Biomedicine. — PubMed
- Iadecola C (2017). The neurovascular unit coming of age: a journey through neurovascular coupling in health and disease. Neuron. — PubMed
PubMed Topic Searches
- PubMed: Shilajit cognitive and memory
- PubMed: Fulvic acid and tau aggregation
- PubMed: Shilajit and Alzheimer
- PubMed: Medhya rasayana Ayurveda
- PubMed: DBP / dibenzo-alpha-pyrone neuroprotection
Connections
- Shilajit Overview
- Shilajit Benefits Hub
- Shilajit for Energy and Fatigue
- Shilajit and Mitochondrial Function
- Shilajit and Testosterone
- Alzheimer's Disease
- Copper-Iron Dysregulation
- Ashwagandha
- Glutathione
- Oxidative Stress
- Heavy Metals
- Magnesium
- All Minerals