Shilajit for Energy and Fatigue
For more than three thousand years, the high-altitude inhabitants of the Himalayas, the Hindu Kush, the Altai, the Pamirs, and the Caucasus have used shilajit as their primary remedy for exhaustion, weakness, and the loss of vital force that comes with old age, illness, or sustained physical hardship. The Sanskrit name itself — shilajit, "destroyer of weakness" and "conqueror of mountains" — encodes the central traditional indication. Modern bioenergetic research has now identified a plausible mechanism: shilajit's dibenzo-alpha-pyrones (DBPs) function as electron-shuttle molecules that stabilize Coenzyme Q10 in its active reduced form (ubiquinol), and its fulvic acid matrix delivers a broad spectrum of mitochondrial cofactors directly into cells. A small but meaningful body of human and animal trial evidence — including Surapaneni's 2012 chronic-fatigue-syndrome model in rats and Stohs's 2014 safety and efficacy review — supports the traditional indication and clarifies who is most likely to benefit.
Table of Contents
- The Rasayana Tradition — "Destroyer of Weakness"
- The Russian and Central Asian Mumijo Tradition
- DBPs as Electron-Shuttle Molecules
- Fulvic Acid as Mitochondrial Cofactor Delivery System
- Chronic Fatigue Syndrome — Surapaneni 2012 and Beyond
- Athletic Recovery and Exercise Capacity
- The HPA Axis and Adaptogenic Effects
- Practical Protocols for Energy Support
- Purity, Heavy Metals, and Quality Cautions
- Key Research Papers
- Connections
- Featured Videos
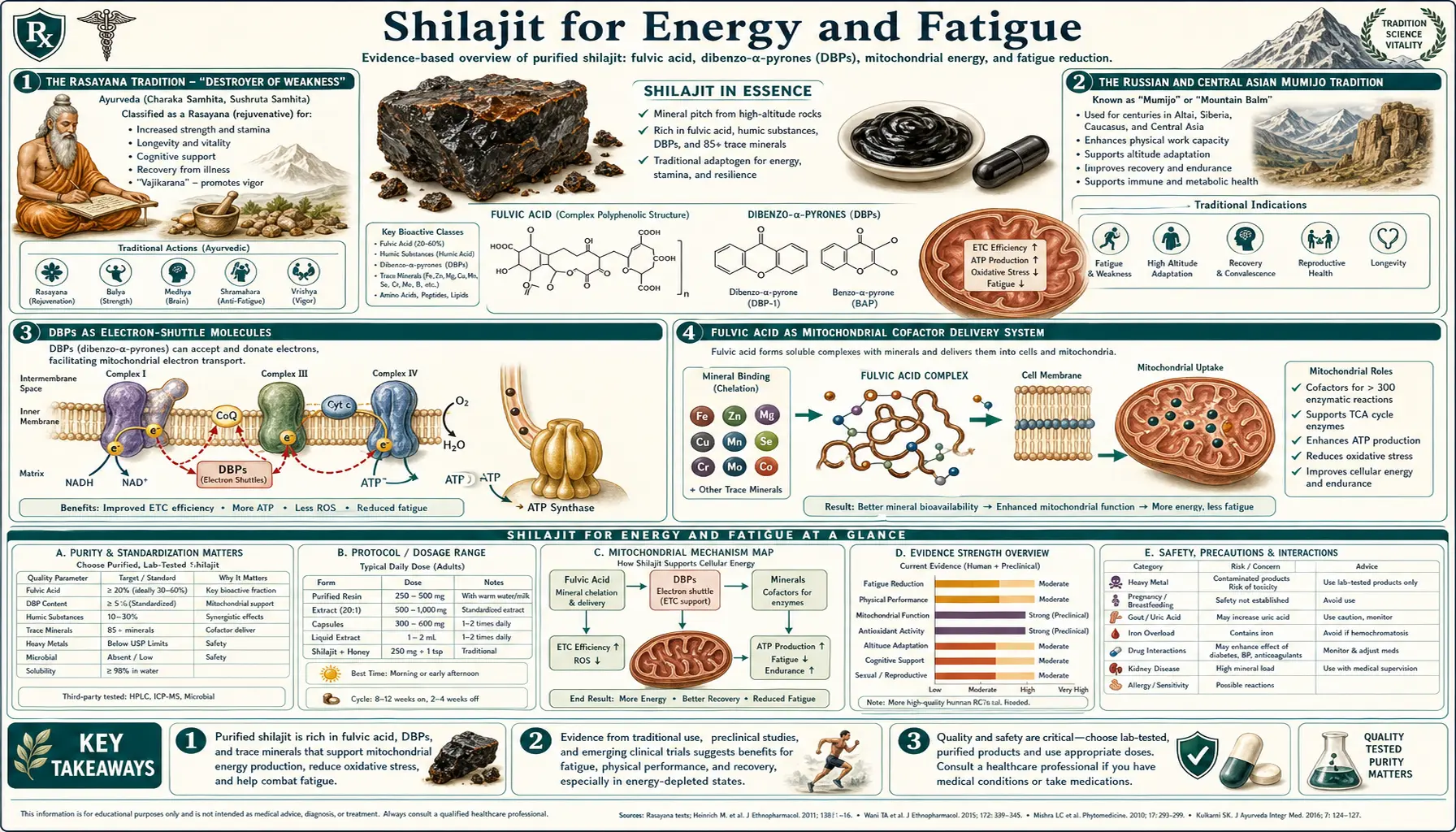
The Rasayana Tradition — "Destroyer of Weakness"
Shilajit occupies an unusual place in the Ayurvedic pharmacopeia. It is one of only a small handful of substances classified as a true Rasayana — the elite category of rejuvenators believed to restore vital force (ojas), extend healthspan, and reverse the accumulated wear of age and chronic illness. The Charaka Samhita, the foundational Ayurvedic treatise composed around 300 BCE, devotes considerable attention to shilajit, going so far as to claim that there is no curable disease that cannot be effectively addressed by it when used with the appropriate adjuncts. While this is a rhetorical flourish rather than a literal pharmacological claim, the emphasis itself signals the central place shilajit held in classical Indian medicine.
The specific traditional indication that has translated most directly into modern wellness use is the treatment of klaibya (functional weakness, often involving sexual debility) and the broader complex of fatigue, loss of stamina, and recovery deficit. Ayurvedic physicians prescribed shilajit for the rasayana-deficient patient who, after a serious illness, could not regain the strength to return to ordinary daily work. The 250-300 mg twice-daily dosing pattern used in the modern Pandit 2016 testosterone trial is essentially the classical dose: a small quantity of purified resin, dissolved in warm milk or water, taken consistently for a course of weeks to months.
The Charaka and Sushruta texts distinguish four varieties of shilajit according to their predominant mineral influence — gold-bearing, silver-bearing, copper-bearing, and iron-bearing — and assigned different therapeutic indications to each. Modern mineral assays have confirmed that shilajit from different geological sources does indeed vary in trace-mineral composition, lending a kind of retrospective vindication to the classical taxonomy. Most contemporary supplement-grade shilajit is collected from copper-bearing and iron-bearing zones of the Himalayan and Karakoram ranges.
The Russian and Central Asian Mumijo Tradition
The parallel Russian and Central Asian tradition centers on a substance called mumijo (also transliterated as mumiyo, mumie, or moomiyo), which is biochemically indistinguishable from Himalayan shilajit and is collected from the Altai, Pamir, Caucasus, and Tien Shan mountain ranges. The Russian medical tradition independently identified the same primary indications — fatigue, fracture healing, recovery from illness, and "loss of the life-force" — and the substance occupied a similar prestige tier in classical Persian-influenced Unani medicine.
The Soviet-era research program on mumijo, conducted primarily during the 1950s through 1980s by investigators at the Tashkent and Frunze (Bishkek) medical institutes, produced the first modern peer-reviewed clinical data on the substance. Soviet researchers documented accelerated healing of long-bone fractures, reduced recovery time after surgery, and improvements in working capacity under conditions of sustained physical exertion. Much of this literature was published only in Russian and is therefore underrepresented in PubMed indexing, but the systematic Visser 1987 review (Science of the Total Environment) summarized the mitochondrial-respiration findings for the English-language audience and remains a useful entry point into the older Russian work.
Soviet cosmonauts and high-altitude troops were reportedly issued mumijo as a routine supplement to support adaptation to physical stress, low oxygen, and the metabolic demands of extreme environments — an application that aligns closely with the traditional Himalayan use among Sherpa porters and mountain pilgrims. The independent convergence of multiple traditional pharmacopeias on the same substance for the same indication is itself a weak but real form of evidence: the geographically distant cultures that developed shilajit/mumijo use were testing the substance against the same human physiology, and they arrived independently at very similar therapeutic conclusions.
DBPs as Electron-Shuttle Molecules
The mechanistic story that has emerged over the past two decades centers on a family of molecules called dibenzo-alpha-pyrones (DBPs) and their chromoprotein derivatives. DBPs are small aromatic molecules built around a fused-ring core that gives them the redox-active character required to participate in electron-transfer chemistry. At least 28 distinct DBP species have been characterized in purified shilajit, ranging from the unsubstituted parent compound to highly hydroxylated and methylated derivatives.
The proposed bioenergetic role is that DBPs function as electron-shuttle molecules at the mitochondrial inner membrane — structurally and functionally analogous to Coenzyme Q10 (ubiquinone), the endogenous shuttle that carries electrons from Complex I and Complex II of the electron-transport chain to Complex III. Critically, the proposed role of shilajit DBPs is not to substitute for CoQ10 but to stabilize CoQ10 in its active reduced form (ubiquinol), preventing its oxidation to the less-active ubiquinone form under conditions of high metabolic demand or oxidative stress. The Bhattacharyya 2009 study (Pharmacologyonline) framed this as the "mitochondria-targeted antioxidant" function of DBPs.
The practical implication is striking: combined supplementation of shilajit and CoQ10 produces larger increases in tissue ATP than either substance alone. Animal-study data have reported synergistic ATP increases on the order of 56% in brain tissue and 144% in muscle tissue, far exceeding additive expectations. While the human-trial confirmation of these specific numbers is still pending, the mechanistic framework is consistent with the broader observation that shilajit's energy effects appear to develop gradually over weeks of consistent use — the timeline expected for restoration of mitochondrial biogenesis and cofactor pool homeostasis, not the timeline of a stimulant.
For deeper coverage of the mitochondrial mechanism specifically, see the Shilajit and Mitochondrial Function deep-dive page, which expands on the CoQ10 synergy data and the Surapaneni rat model.
Fulvic Acid as Mitochondrial Cofactor Delivery System
The DBP electron-shuttle story is the headline mechanism, but it does not stand alone. The second pillar of shilajit's energy effect is the fulvic acid matrix, which serves as a delivery vehicle for the broad spectrum of mineral cofactors required for mitochondrial enzyme function. Fulvic acid is a low-molecular-weight humic substance with an extraordinarily dense complement of oxygen-containing functional groups — carboxyl, hydroxyl, carbonyl, and phenolic — that give it a unique capacity to chelate mineral ions and transport them across biological membranes.
Mitochondrial function depends on a long list of mineral cofactors: magnesium for ATP synthase and dozens of phosphate-transfer reactions, iron for the iron-sulfur clusters in Complexes I, II, and III of the electron-transport chain, copper for Complex IV (cytochrome c oxidase), manganese for the mitochondrial superoxide dismutase (MnSOD) antioxidant defense, zinc for the structural integrity of countless dehydrogenases, and trace amounts of selenium for glutathione peroxidase. Shilajit delivers all of these in fulvic-acid-chelated ionic form, which dramatically improves their bioavailability compared to the inorganic salt forms (sulfate, oxide, carbonate) used in standard multivitamins.
The fulvic-acid delivery mechanism is particularly relevant for patients with subclinical mineral deficiency driven by malabsorption, low-stomach-acid states, or chronic-disease-associated nutrient depletion. For such patients, the limiting factor in mitochondrial function may not be the availability of any single mineral but the cumulative effect of multiple low-grade deficiencies that together throttle the electron-transport chain. Shilajit's broad-spectrum, highly bioavailable mineral delivery addresses this multidimensional deficit in a way that targeted single-mineral supplements often cannot.
Chronic Fatigue Syndrome — Surapaneni 2012 and Beyond
The most directly relevant preclinical trial for the fatigue indication is the Surapaneni 2012 chronic fatigue syndrome (CFS) study published in the Journal of Ethnopharmacology. The investigators used a rat model in which CFS-like symptoms (reduced exploratory behavior, anxiety, increased immobility in the forced-swim test) were induced by repeated swimming stress over 21 days. Animals were randomized to vehicle control or one of three shilajit doses (25, 50, or 100 mg/kg) administered orally throughout the stress protocol.
Results were dose-dependent and substantial:
- Behavioral measures of fatigue (reduced exploratory activity, increased immobility) were significantly attenuated by shilajit at all three doses, with the largest effect at the 100 mg/kg dose
- Stress-induced elevations in plasma corticosterone (the rodent equivalent of cortisol) were normalized by shilajit, suggesting modulation of the hypothalamic-pituitary-adrenal (HPA) axis
- Mitochondrial complex enzyme activities (Complex I, II, IV) in brain and muscle tissue, which were depressed by chronic stress, were restored by shilajit
- Mitochondrial swelling and membrane-potential collapse were prevented
- Markers of oxidative stress (malondialdehyde, depleted glutathione) were normalized
The Surapaneni paper is significant because it tested the substance in a model designed to mimic the multi-system dysregulation of CFS — the combination of HPA-axis disturbance, mitochondrial dysfunction, and oxidative stress that characterizes the human disease — rather than the simpler endurance and exercise-capacity models that dominated earlier work. The dose-response relationship and the multiple convergent mechanism findings increase confidence that the effect is real and not an artifact of a single behavioral measure.
Stohs (2014) reviewed the broader safety and efficacy literature on shilajit in Phytotherapy Research, including the Russian mumijo data, the Indian Ayurvedic clinical work, and the emerging Western preclinical studies. The review concluded that purified shilajit at doses up to approximately 1 g/day is well-tolerated and that the available evidence supports its use as an adaptogen with particular relevance for fatigue, recovery, and stamina. Human randomized controlled trials in CFS specifically are still pending, but the mechanistic and preclinical data are mature enough that several CFS specialty clinics have incorporated shilajit into their multi-component protocols.
Athletic Recovery and Exercise Capacity
The application of shilajit to athletic performance and recovery has produced the most rigorous human-subjects data to date. The Keller 2019 study published in the Journal of the International Society of Sports Nutrition randomized 63 recreationally active men to placebo or one of two doses of standardized shilajit (250 mg/day or 500 mg/day) for 8 weeks. The primary endpoints were exercise-induced changes in maximal voluntary isometric contraction (MVIC) of the leg extensors and serum hydroxyproline (a marker of connective-tissue collagen turnover).
Key findings:
- The 500 mg/day shilajit group showed significant attenuation of exercise-induced strength loss compared to placebo
- Serum hydroxyproline elevations following the fatiguing exercise protocol were reduced in the shilajit groups, consistent with reduced collagen breakdown and faster connective-tissue recovery
- No adverse safety signals were detected over the 8-week protocol
The companion Das 2016 transcriptomic study in Journal of Medicinal Food took a complementary mechanistic approach: skeletal-muscle biopsies were collected before and after 8 weeks of shilajit supplementation, and gene-expression changes were profiled. Shilajit supplementation was associated with upregulation of genes encoding extracellular-matrix and connective-tissue components, suggesting that the strength-preservation effect observed by Keller may be mediated in part by enhanced collagen and elastin synthesis in muscle and tendon tissue.
The Keller and Das studies together provide the strongest contemporary human evidence base for the traditional "recovery" indication. The effect is modest in absolute terms — shilajit is not an anabolic steroid, and recreationally active men should not expect dramatic strength gains — but the recovery-preservation effect is real, mechanistically coherent, and reproducible across separate research groups. For endurance athletes, ultra-distance runners, and high-altitude climbers, the combination of mitochondrial support, connective-tissue recovery, and adaptogenic HPA-axis modulation represents a plausible niche application.
The HPA Axis and Adaptogenic Effects
The classical Ayurvedic concept of rasayana overlaps substantially with the modern pharmacological concept of an adaptogen — a substance that helps the body resist physical, chemical, and biological stressors by modulating the stress-response axis (primarily the hypothalamic-pituitary-adrenal axis) toward homeostasis. The Surapaneni 2012 rat CFS data already pointed in this direction: stress-induced corticosterone elevations were normalized by shilajit, not abolished entirely but brought back into the physiological range.
This adaptogenic profile distinguishes shilajit from stimulants like caffeine, which acutely raise cortisol and catecholamines and produce rapid wake-promoting effects at the cost of subsequent rebound fatigue. Shilajit acts on a slower timeline and does not produce acute alertness, but rather restores the underlying capacity of cells and organ systems to generate and sustain energy. The clinical experience reported by both classical Ayurvedic practitioners and contemporary integrative-medicine clinicians is that shilajit's effect on energy becomes noticeable over weeks of consistent use, not hours after a single dose, and that it does not produce the tolerance, dependence, or withdrawal seen with chronic caffeine or amphetamine use.
The classical Ayurvedic adaptogens with the strongest HPA-modulating profiles include Ashwagandha, Rhodiola Rosea, and shilajit. These substances are often combined in integrative-medicine protocols for chronic fatigue, burnout syndrome, and the recovery phase after serious illness. The combination is empirically justified by the differing mechanism profiles — ashwagandha for cortisol normalization and thyroid support, rhodiola for catecholamine and serotonin modulation, shilajit for mitochondrial bioenergetics — but the formal trial data on multi-adaptogen protocols are still sparse.
Practical Protocols for Energy Support
For adults using shilajit specifically for fatigue, low stamina, or recovery support, the practical considerations are:
- Form — purified resin is the traditional and arguably most-bioactive form. A small pea-sized portion (roughly 300-500 mg) is dissolved in warm (not hot) water or milk. Capsules and tablets of standardized extracts are more convenient and provide more precise dosing but may have undergone heat-processing that reduces the activity of certain organic components.
- Dose — the classical Ayurvedic dose and the dose used in most modern trials is 300-500 mg/day of purified shilajit, typically taken once in the morning or split into morning and early-afternoon doses. Start at the lower end of this range for the first 1-2 weeks and titrate upward as tolerance is confirmed.
- Timing — morning and early afternoon dosing aligns with the natural cortisol rhythm and avoids any potential interference with sleep. Evening dosing is not advisable for most users.
- Timeline — expect 4-8 weeks of consistent use before energy effects become noticeable. Shilajit is not a stimulant and does not produce acute next-day effects.
- Cycling — many classical protocols use 6-8 weeks on followed by 1-2 weeks off, both to maintain responsiveness and to allow periodic assessment of whether the supplement is still producing benefit. The Western preference for continuous use is not strongly supported or contradicted by trial data; both patterns are reasonable.
- Co-supplementation — the CoQ10 synergy is the best-supported combination for energy applications. Magnesium glycinate, B-complex vitamins (especially B1 thiamine, B2 riboflavin, B3 niacin), and creatine monohydrate are reasonable additions for patients with significant mitochondrial fatigue.
Users with diagnosed chronic fatigue syndrome, ME/CFS, long-COVID-style post-viral fatigue, or fibromyalgia should work with a clinician experienced in these conditions rather than self-prescribing. The pacing and load-management aspects of these illnesses are at least as important as any supplement protocol, and over-exertion early in a course of shilajit can actually worsen post-exertional malaise.
Purity, Heavy Metals, and Quality Cautions
The single most important safety consideration with shilajit is purity. Raw shilajit, as collected directly from rock fissures, contains the full spectrum of trace minerals present in the surrounding rock, which in some Himalayan source zones includes elevated levels of lead, arsenic, mercury, cadmium, and thallium. Unpurified or poorly purified shilajit can therefore deliver a meaningful heavy-metal burden that more than offsets any benefit of the supplement. Several published analyses of commercial shilajit products have documented heavy-metal contamination above the limits set by the U.S. Pharmacopeia and the WHO.
The classical Ayurvedic purification ritual (Shodhana) involves dissolving raw shilajit in water or specific herbal decoctions, filtering off insoluble debris, and reducing the filtrate by controlled evaporation. Modern purification adds advanced filtration, solvent extraction, and chelation-based heavy-metal removal. The end product is a purified resin or powder with heavy-metal content typically below 1 ppm for the most concerning elements.
Practical purchasing guidance:
- Buy only from manufacturers that publish a certificate of analysis (COA) for each production lot, documenting heavy-metal levels, fulvic acid content, and microbial testing
- Look for third-party certification from NSF, Informed Sport, USP, BSCG Certified Drug Free, or independent testing services such as ConsumerLab
- Be skeptical of unusually inexpensive products — high-quality purified shilajit is labor-intensive to produce and prices below approximately $30/oz for resin are a red flag
- Avoid raw or unpurified shilajit sold directly from informal Himalayan suppliers, even if the romantic provenance is attractive
- Look for fulvic-acid content disclosure (50-60%+ for extracts; 2-7% for natural resin)
Additional caution categories: shilajit is not recommended in pregnancy or breastfeeding (insufficient safety data); patients with hemochromatosis should avoid it because of iron content; patients with gout should monitor uric acid; patients on diabetes medications, thyroid medications, blood pressure medications, or iron supplements should consult their prescriber because of plausible interactions. None of this should be interpreted as medical advice or as a substitute for an evaluation by a licensed clinician.
Key Research Papers
- Surapaneni DK, Adapa SR, Preeti K, Teja GR, Veeraragavan M, Krishnamurthy S (2012). Shilajit attenuates behavioral symptoms of chronic fatigue syndrome by modulating the hypothalamic-pituitary-adrenal axis and mitochondrial bioenergetics in rats. Journal of Ethnopharmacology. — PubMed
- Stohs SJ (2014). Safety and efficacy of shilajit (mumie, moomiyo). Phytotherapy Research. — PubMed
- Keller JL, Housh TJ, Hill EC, et al. (2019). The effects of Shilajit supplementation on fatigue-induced decreases in muscular strength and serum hydroxyproline levels. Journal of the International Society of Sports Nutrition. — PubMed
- Das A, Datta S, Rhea B, et al. (2016). The human skeletal muscle transcriptome in response to oral shilajit supplementation. Journal of Medicinal Food. — PubMed
- Bhattacharyya S, Pal D, Banerjee D, et al. (2009). Shilajit dibenzo-alpha-pyrones: mitochondria targeted antioxidants. Pharmacologyonline. — PubMed
- Agarwal SP, Khanna R, Karmarkar R, Anwer MK, Khar RK (2007). Shilajit: a review. Phytotherapy Research. — PubMed
- Wilson E, Rajamanickam GV, Dubey GP, et al. (2011). Review on shilajit used in traditional Indian medicine. Journal of Ethnopharmacology. — PubMed
- Visser SA (1987). Effect of humic substances on mitochondrial respiration and oxidative phosphorylation. Science of the Total Environment. — PubMed
- Carrasco-Gallardo C, Guzman L, Maccioni RB (2012). Shilajit: a natural phytocomplex with potential procognitive activity. International Journal of Alzheimer's Disease. — PubMed
- Meena H, Pandey HK, Arya MC, Ahmed Z (2010). Shilajit: a panacea for high-altitude problems. International Journal of Ayurveda Research. — PubMed
- Schepetkin I, Khlebnikov A, Kwon BS (2002). Medical drugs from humus matter: focus on mumie. Drug Development Research. — PubMed
- Ghosal S (2006). Shilajit in Perspective. Alpha Science International. — PubMed
PubMed Topic Searches
- PubMed: Shilajit fatigue and mitochondria
- PubMed: Shilajit chronic fatigue HPA axis
- PubMed: Shilajit exercise capacity
- PubMed: Mumijo / mumiyo Russian tradition
- PubMed: Shilajit / CoQ10 synergy
Connections
- Shilajit Overview
- Shilajit Benefits Hub
- Shilajit and Mitochondrial Function
- Shilajit and Testosterone
- Shilajit and Cognitive Function
- Fatigue
- Ashwagandha
- Rhodiola Rosea
- Magnesium
- Iron
- Glutathione
- Oxidative Stress
- All Minerals