Manganism (Manganese Toxicity): Mood and Cognitive Changes
Before the trembling hands of classic manganese poisoning ever appear, the first thing to change is often the mind and the mood. Workers heavily exposed to manganese dust have described it for over a century: a creeping irritability, a short fuse, spells of unexplained laughter or weeping, trouble concentrating, and a fog that slows thinking and blunts memory. Doctors once called the early phase “manganese madness.” The honest truth, though, is that irritability and brain fog are among the most common and least specific symptoms in all of medicine — caused far more often by stress, poor sleep, depression, thyroid trouble, or a dozen other things than by a metal. Manganese is a real but uncommon cause, almost always tied to heavy occupational exposure, very high environmental water levels, or failing-liver biology. This page explains how the mood and cognitive changes of manganism feel, the brain chemistry behind them, why they so rarely point to manganese on their own, and the specific clues that should make a clinician look harder.
Table of Contents
- What the Mood & Cognitive Changes Feel Like
- The Mechanism: Why Excess Manganese Disturbs Mood and Thinking
- An Honest Caution: These Symptoms Are Rarely About Manganese
- Clues That Point Toward Manganese
- Where the Excess Manganese Comes From
- Getting Checked
- How Manganese Overload Is Managed
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
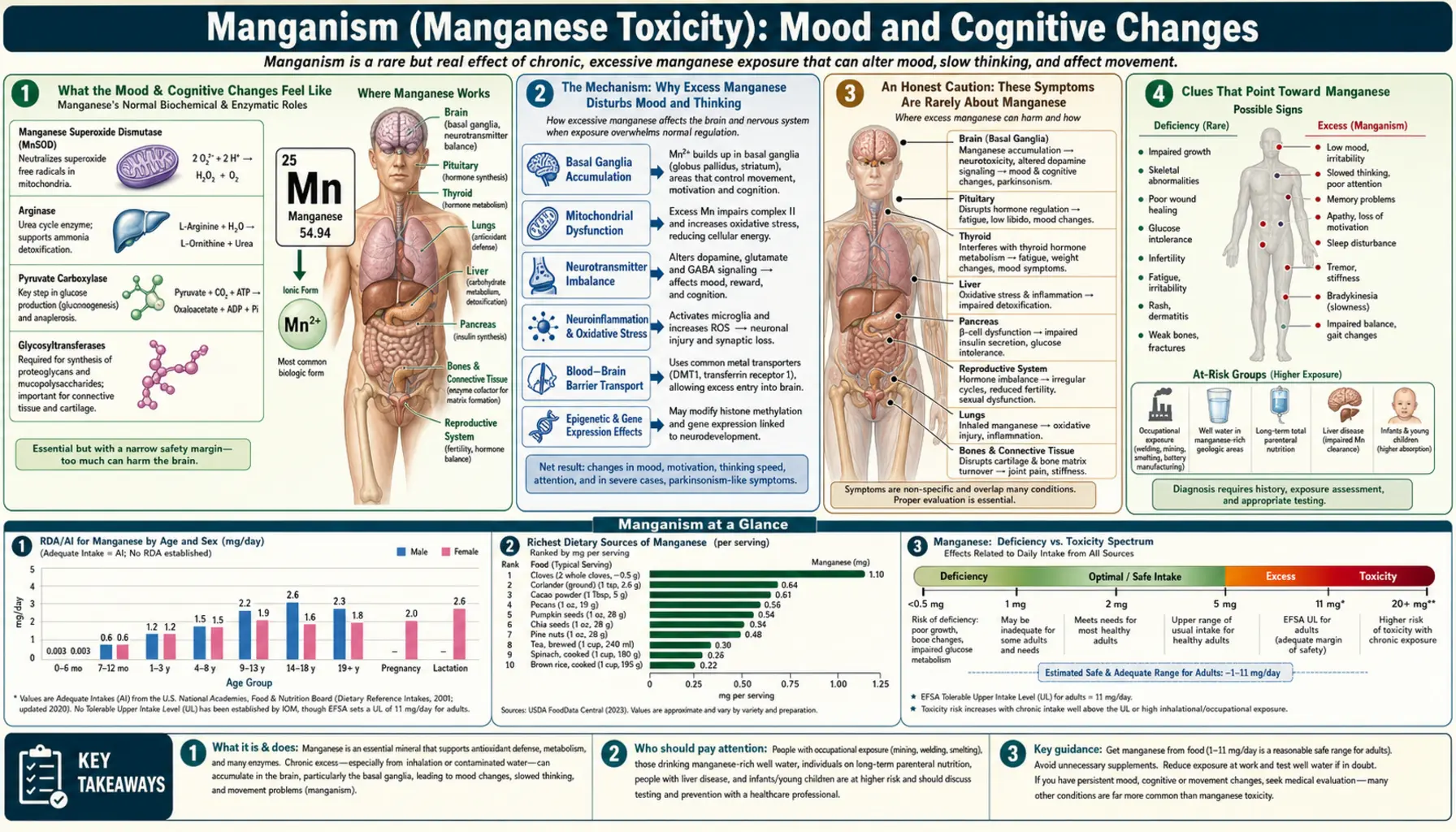
What the Mood & Cognitive Changes Feel Like
The mood and thinking changes of manganese excess are easy to dismiss because, at first, they look like ordinary stress or burnout. They tend to come on gradually, over months, in someone with a heavy ongoing exposure — not as a sudden, dramatic event. When researchers have interviewed manganese-exposed welders and ferroalloy workers, the same descriptions surface again and again:
- Irritability and a short fuse. A person who used to be even-tempered finds themselves snapping at family or coworkers, impatient over small things, quick to anger. Spouses often notice the change before the worker does.
- Emotional lability. Moods swing more than usual — bouts of tearfulness, anxiety, or unexpected laughter that don’t match the situation. The older medical literature called this “emotional incontinence.”
- Low mood and loss of drive. A flattened, depressed feeling, low motivation, and loss of interest in things once enjoyed — sometimes hard to separate from simple exhaustion.
- Brain fog and slowed thinking. Trouble concentrating, a sense that the mind is working in slow motion, difficulty finding words, and forgetfulness for recent events and tasks. (See the general symptom page on brain fog.)
- Restlessness, nervousness, and disturbed sleep. Feeling keyed-up or on edge, with trouble falling or staying asleep, is commonly reported alongside the mood changes.
In rare, severe historical cases of heavy mine or smelter exposure, the early psychiatric picture went further — vivid hallucinations, compulsive or impulsive behavior, and episodes of agitation that gave the syndrome its old name, “manganese madness.” That dramatic form is essentially a thing of the past, seen with exposures far higher than today’s regulated workplaces allow. The modern picture is subtler: irritability, anxiety, low mood, and cognitive slowing.
One feature is worth holding onto. In manganism, these psychiatric and cognitive symptoms classically come first — before, and sometimes long before, the movement problems (slowness, stiffness, a characteristic gait, tremor) covered on the sibling page Tremor & Parkinsonism. So mood and cognitive change is the early warning of heavy manganese exposure, not the late stage. That is exactly what makes it both important and treacherous: it is the first thing to appear, yet it looks like everything else.
The Mechanism: Why Excess Manganese Disturbs Mood and Thinking
Manganese is an essential nutrient — in the small amounts we get from food it is a vital part of enzymes that handle antioxidant defense, bone formation, and energy metabolism (see manganese and the Mn-SOD antioxidant enzyme). The body normally keeps it on a tight leash: the gut absorbs only a few percent of dietary manganese, and the liver promptly dumps the excess into bile so it leaves in the stool. Trouble begins only when that leash breaks — when manganese is inhaled (bypassing the gut entirely), when intake is enormous, or when a failing liver can no longer clear it.
When manganese does accumulate, it concentrates in a deep brain region called the basal ganglia — in particular the globus pallidus and nearby nuclei — the same circuitry that fine-tunes movement, motivation, and emotion. Several overlapping mechanisms then disturb the brain’s chemistry:
- It tangles dopamine signaling. The basal ganglia run on the neurotransmitter dopamine, which governs not only movement but also drive, reward, and mood. Excess manganese disrupts how dopamine is stored, released, and handled, which helps explain both the later movement problems and the early changes in motivation and mood.
- It generates oxidative stress. Manganese can cycle between chemical forms and drive the formation of reactive, damaging molecules inside neurons. In excess it impairs the cell’s power plants (the mitochondria), starving energy-hungry neurons — one plausible contributor to the fog and slowed thinking.
- It inflames support cells and shifts other neurotransmitters. Manganese accumulates heavily in astrocytes, the brain’s support cells, provoking inflammation and disturbing the handling of glutamate and GABA — the brain’s main “go” and “stop” signals. An imbalance there can plausibly tip a person toward irritability, anxiety, and trouble concentrating.
An analogy. Think of the basal ganglia as a recording studio’s mixing board, where dopamine is the engineer’s hand setting the levels on movement, mood, and focus. A trace of manganese is part of the equipment that keeps the board running. Flood the board with too much of it, though, and it is like spilling liquid into the console: the sliders stick and jump, channels distort, and the mix that comes out is jittery and uneven — a short temper here, a flattened mood there, a foggy delay on every thought. Crucially, mop the spill up early and the board can still recover; let it soak in for years and some channels are damaged for good. That mirrors what doctors see: caught early, the mood and cognitive symptoms of manganism can improve once exposure stops, but advanced, long-standing manganism can leave permanent changes.
An Honest Caution: These Symptoms Are Rarely About Manganese
This is the most important section to read. Irritability, low mood, anxiety, and brain fog are some of the most common and least specific complaints anyone brings to a doctor. The overwhelming majority of people with these symptoms have nothing whatsoever to do with manganese. Before a metal is even considered, the far more likely explanations should be thought through:
- Sleep deprivation and chronic stress — by a wide margin the most common causes of irritability and a foggy, slowed mind.
- Mood and anxiety disorders — depression and generalized anxiety routinely produce poor concentration, low motivation, emotional swings, and a short temper.
- Thyroid disease — both an underactive and an overactive thyroid classically cause mood change and cognitive trouble, and both are easily checked with a blood test.
- Nutritional shortfalls — low iron (anemia), vitamin B12 or vitamin D deficiency are common, treatable causes of fatigue and brain fog.
- Medications, alcohol, and other substances — many drugs, heavy alcohol use, and withdrawal states change mood and thinking.
- Other medical conditions — perimenopause, chronic pain, infections, blood-sugar swings, and early cognitive disorders such as Alzheimer’s disease can all present this way.
Manganese excess belongs near the bottom of that list for a person with no unusual exposure. A clinician does not order a manganese test for everyday irritability or forgetfulness, and neither should you reach for that explanation first. Manganism is genuinely uncommon, and it is essentially a disease of specific circumstances — heavy occupational inhalation, extreme environmental water levels, certain forms of liver failure, or unusual intravenous exposure. The symptom on this page is real, but it earns serious attention only when it sits on top of one of those circumstances. Without that, the honest, accurate answer is that the cause is almost certainly something more ordinary and more treatable.
Clues That Point Toward Manganese
So when should manganese cross a clinician’s mind? The mood and cognitive changes start to point toward manganism only when they keep company with a recognizable backdrop:
- A high-exposure occupation. Welding (especially in confined spaces), steel and ferroalloy manufacturing, smelting, dry-cell battery making, mining and ore processing, and the manufacture or grinding of manganese-containing products. A new short temper, fogginess, or low mood in a long-time welder deserves more than a shrug.
- Movement changes creeping in behind the mood changes. If subtle slowness, stiffness, clumsiness, a shuffling or “cock-walk” gait, or a tremor begins to follow the psychiatric symptoms, the combination is far more suggestive than mood change alone. That motor side is detailed on Tremor & Parkinsonism.
- A specific high-manganese exposure outside work. Well water with very high manganese, or long-term high-dose manganese supplementation. The pediatric and environmental angle is covered on Occupational & Water Exposure.
- Advanced liver disease. Because the liver is the body’s exit route for manganese, people with cirrhosis or other severe liver disease can accumulate manganese in the brain even without any outside exposure — sometimes contributing to the confusion of hepatic encephalopathy.
- Long-term intravenous nutrition. People dependent on long-term total parenteral nutrition (TPN) receive manganese directly into the bloodstream, bypassing the gut’s protective gatekeeping, and can accumulate it over time.
The pattern that should raise a real flag, then, is not “I’ve been irritable and foggy” on its own — it is “I’ve been irritable and foggy, and I weld for a living (or have very high well-water manganese, or advanced liver disease), and my coordination or walking is starting to change.” That cluster is what turns an ordinary complaint into a reason to test.
Where the Excess Manganese Comes From
Understanding the route of exposure matters, because the body’s defenses against dietary manganese are strong — so toxicity nearly always means one of those defenses has been bypassed or overwhelmed:
- Inhaled manganese fumes and dust (the classic cause). When manganese is breathed in — from welding fumes, smelting, ferroalloy work, mining, or battery manufacture — it skips the gut’s tight absorption control entirely and can travel from the airways and nose toward the brain. This is why manganism is, above all, an occupational, airborne disease, and why fume control and respiratory protection are central to prevention.
- Very high environmental water levels. Naturally manganese-rich groundwater (some private wells) can deliver large oral doses. Most studies of cognitive effects from drinking water involve children, whose developing brains appear more vulnerable.
- High-dose oral supplementation. Manganese is widely available as a supplement and is present in many multivitamins and mineral blends. Ordinary dietary intake is safe and necessary, but chronically excessive supplemental doses — especially in someone with reduced liver clearance — can contribute to overload.
- Liver failure. With the biliary exit route impaired by cirrhosis or severe liver disease, manganese builds up in the basal ganglia even on a normal diet.
- Intravenous routes. Long-term TPN and, historically, intravenous drug use involving manganese-contaminated preparations deliver manganese straight into the blood, bypassing the gut.
A reassuring counterpoint: a normal, varied diet — whole grains, legumes, nuts, leafy greens, tea — supplies plenty of manganese and does not cause manganism. Eating manganese-rich foods is healthy. Toxicity is about how and how much manganese enters the body, not about ordinary food.
Getting Checked
There is no single perfect test for manganese toxicity, and this is an important honesty point: a manganese level cannot, by itself, diagnose manganism. The evaluation weaves together the exposure history, the symptoms, blood work, and imaging.
Blood manganese can be measured, but it is an imperfect window. Because manganese is cleared quickly and stored in tissues, a blood level mostly reflects recent exposure and correlates poorly with how much has accumulated in the brain or how severe the symptoms are. A normal blood level does not rule out past or ongoing harm, and a mildly elevated one does not prove it. A clinician will usually also check a comprehensive metabolic panel — especially liver function — because liver disease is a key route to manganese accumulation, and will screen for the far more common causes of mood and cognitive symptoms (thyroid testing, iron studies, vitamin B12, blood sugar).
Brain MRI is the most telling test when manganism is genuinely suspected. Manganese is naturally paramagnetic, so accumulation produces a characteristic bright signal in the globus pallidus on a particular MRI sequence (T1-weighted images) — a recognizable fingerprint of manganese deposition. Combined with a fitting exposure history and symptoms, that imaging pattern carries far more weight than a blood number.
Finally, because the early symptoms are subtle and overlap with everyday complaints, formal neuropsychological testing can document and track the cognitive changes objectively, and a neurologist’s exam can detect the early movement signs that strengthen the case. The diagnosis, in short, is a picture assembled from exposure, symptoms, imaging, and the exclusion of commoner causes — not a single lab value.
How Manganese Overload Is Managed
Managing manganese toxicity rests on one principle above all others, and several supporting measures:
- Stop the exposure — the single most important step. Removing the source is the cornerstone of treatment: improving workplace fume extraction and respiratory protection, reassigning a worker away from heavy manganese exposure, switching to a low-manganese water supply (filtration or an alternate source), or stopping unnecessary high-dose manganese supplements. With ongoing exposure halted, mild and early symptoms can improve over time as the brain slowly offloads manganese.
- Treat the underlying liver disease. When accumulation stems from cirrhosis or other liver disease, the focus shifts to managing that condition; manganese can fall as liver function is supported (or after transplantation in advanced cases). For people on long-term TPN, the manganese content of the formula is reviewed and reduced.
- Chelation has only a limited role. Unlike lead or some other metals, manganese is not reliably removed by chelation therapy. Agents such as EDTA have been tried with inconsistent results and are not a standard, dependable cure. This is a sobering reality and another reason prevention matters so much.
- Symptom-directed and supportive care. The movement symptoms of established manganism generally respond poorly to the levodopa used for Parkinson’s disease — an important difference from idiopathic Parkinson’s, since manganese damages targets downstream of where levodopa acts. Treatment is therefore largely supportive: managing depression or anxiety, physical and occupational therapy, and addressing sleep.
The hard truth is that prevention is far more effective than cure. Once-established, advanced manganism can be partly or wholly irreversible, which is exactly why workplace exposure limits, fume controls, and prompt action on the early mood and cognitive warning signs — before movement problems set in — matter so much.
When to Seek Care / Red Flags
Because everyday irritability and brain fog are usually not about manganese, the trigger to seek care is the combination of these symptoms with a real exposure or with new neurological signs. See a doctor — and mention your exposure history specifically — if you notice:
- New or worsening mood and cognitive changes in a high-exposure worker — a welder, smelter, miner, ferroalloy or battery worker who has become uncharacteristically irritable, anxious, low, or foggy. Tell the clinician about the manganese exposure; they may not ask.
- Mood or cognitive change followed by movement problems — new slowness, stiffness, clumsiness, tremor, balance trouble, or a changed (shuffling or stiff-legged) gait appearing behind the psychiatric symptoms. This cluster warrants prompt neurological evaluation.
- Symptoms plus very high well-water manganese, or long-term high-dose supplements — particularly worth raising if children in the household are affected (see Occupational & Water Exposure).
- Cognitive change with known advanced liver disease — new confusion, drowsiness, or disorientation in someone with cirrhosis needs urgent assessment, as it may signal hepatic encephalopathy.
Seek emergency care for any sudden, severe change — abrupt confusion or disorientation, a marked behavioral change, hallucinations, fainting, or thoughts of harming yourself. Those are not typical of the slow, creeping picture of manganism and point to a different, urgent problem that needs immediate evaluation. For the gradual symptoms, the goal is simpler: get exposure recognized and stopped early, while the changes are still most likely to improve.
Key Research Papers
- Horning KJ, Caito SW, Tipps KG, Bowman AB, Aschner M (2015). Manganese Is Essential for Neuronal Health. Annual Review of Nutrition;35:71-108. — DOI: 10.1146/annurev-nutr-071714-034419
- Guilarte TR, Gonzales KK (2015). Manganese-Induced Parkinsonism Is Not Idiopathic Parkinson's Disease: Environmental and Genetic Evidence. Toxicological Sciences;146(2):204-212. — DOI: 10.1093/toxsci/kfv099
- Bowler RM, Gysens S, Diamond E, Nakagawa S, Drezgic M, Roels HA (2006). Manganese exposure: Neuropsychological and neurological symptoms and effects in welders. NeuroToxicology;27(3):315-326. — DOI: 10.1016/j.neuro.2005.10.007
- Bouchard M, Mergler D, Baldwin M, Panisset M, Roels HA (2007). Neuropsychiatric symptoms and past manganese exposure in a ferro-alloy plant. NeuroToxicology;28(2):290-297. — DOI: 10.1016/j.neuro.2006.08.002
- Bouchard M, Mergler D, Baldwin M (2003). Blood Manganese and Alcohol Consumption Interact on Mood States Among Manganese Alloy Production Workers. NeuroToxicology;24(4-5):641-647. — DOI: 10.1016/s0161-813x(03)00028-7
- Lucchini R, Selis L, Folli D, Apostoli P, Mutti A, Vanoni O, Iregren A, Alessio L (1995). Neurobehavioral effects of manganese in workers from a ferroalloy plant after temporary cessation of exposure. Scandinavian Journal of Work, Environment & Health;21(2):143-149. — DOI: 10.5271/sjweh.1369
- Bouchard MF, Sauvé S, Barbeau B, Legrand M, Brodeur ME, Bouffard T, Limoges E, Bellinger DC, Mergler D (2011). Intellectual Impairment in School-Age Children Exposed to Manganese from Drinking Water. Environmental Health Perspectives;119(1):138-143. — DOI: 10.1289/ehp.1002321
- Bouchard M, Laforest F, Vandelac L, Bellinger D, Mergler D (2007). Hair Manganese and Hyperactive Behaviors: Pilot Study of School-Age Children Exposed through Tap Water. Environmental Health Perspectives;115(1):122-127. — DOI: 10.1289/ehp.9504
- Mena I, Marin O, Fuenzalida S, Cotzias GC (1967). Chronic manganese poisoning: Clinical picture and manganese turnover. Neurology;17(2):128-136. — DOI: 10.1212/wnl.17.2.128
- Racette BA, Antenor JA, McGee-Minnich L, Moerlein SM, Videen TO, Kotagal V, Perlmutter JS (2005). [18F]FDOPA PET and clinical features in parkinsonism due to manganism. Movement Disorders;20(4):492-496. — DOI: 10.1002/mds.20381
- Bouchard M, Mergler D, Baldwin M, Panisset M, Bowler R, Roels HA (2005). Manganese exposure and age: neurobehavioral performance among alloy production workers. Environmental Toxicology and Pharmacology;19(3):687-694. — DOI: 10.1016/j.etap.2004.12.037
PubMed Topic Searches
- PubMed — Manganese, neuropsychiatric symptoms, mood, and irritability
- PubMed — Manganese, welders, and cognitive/neurobehavioral effects
- PubMed — Manganism, globus pallidus, MRI, and the basal ganglia
- PubMed — Manganese in drinking water and children's cognition
- PubMed — Manganese, liver disease, and hepatic encephalopathy
Connections
- Manganese Toxicity Hub
- Manganism and Tremor & Parkinsonism
- Manganese Occupational & Water Exposure
- Manganese Deficiency Hub
- Manganese Overview
- Manganese and the Mn-SOD Antioxidant Enzyme
- Manganism (Toxic Minerals)
- Toxic Minerals Hub
- Iron
- Parkinson's Disease
- Alzheimer's Disease
- Cirrhosis
- Liver Disease
- Brain Fog
- Comprehensive Metabolic Panel