Copper Toxicity (Wilson's Disease): Symptoms, Causes, and Risks
Copper is an essential mineral — you genuinely need a little of it every day — but in excess it becomes a poison. Here is the single most important thing to understand: true copper toxicity is uncommon, and when it happens it almost always has a specific cause rather than “too much in the diet.” The two situations that matter are Wilson's disease, an inherited disorder in which the body cannot clear copper so it slowly builds up in the liver and brain, and acute poisoning from swallowing a large amount of a copper salt at once. A healthy person with normal genes who eats an ordinary diet essentially never develops copper overload, because the liver simply excretes the surplus in bile. That is why this page is honest about the boundary: ordinary copper intake is not a threat, but Wilson's disease is a real, treatable, and — if missed — potentially fatal condition that often stays silent for years before it announces itself through the liver or the nervous system. This hub explains what copper toxicity actually is, why excess copper damages the body, why Wilson's disease so often hides, what causes copper to accumulate, and how it is diagnosed and treated — with deep-dive pages on the stomach, liver, and neuro-psychiatric problems it can cause. Do not try to “detox” copper on your own; genuine copper overload is medical territory.
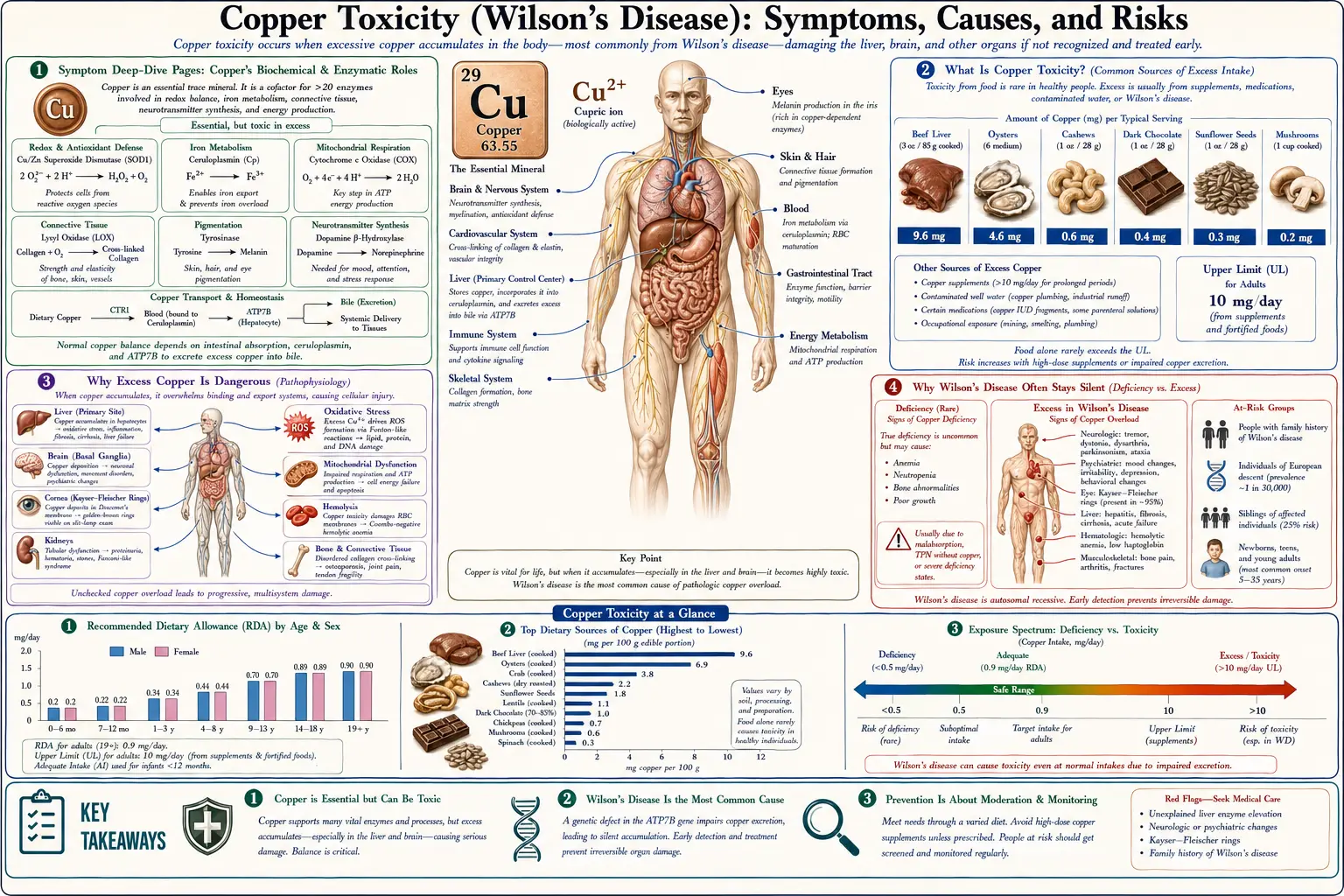
Symptom Deep-Dive Pages
Nausea & Stomach Upset
The most common way acute copper poisoning announces itself — how swallowing too much copper at once irritates the gut, why a metallic taste, nausea, vomiting, and stomach pain are the early warning, and when this becomes an emergency.
Liver Damage
The liver is where copper first accumulates in Wilson's disease and the organ most often injured. How hepatic copper overload can range from a silent rise in liver enzymes to hepatitis, cirrhosis, and rare sudden liver failure.
Neuro & Psychiatric
When copper spills past the liver into the brain it can cause tremor, slurred speech, dystonia, clumsiness, and changes in mood, behavior, or thinking — the often-misread neuropsychiatric face of Wilson's disease.
Table of Contents
- Symptom Deep-Dive Pages
- What Is Copper Toxicity?
- Why Excess Copper Is Dangerous
- Why Wilson's Disease Often Stays Silent
- What Causes Copper to Build Up
- How Copper Toxicity Is Diagnosed
- How Copper Overload Is Treated
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
What Is Copper Toxicity?
Copper is a trace mineral — the body holds only about 50 to 120 milligrams of it in total — yet it is essential. It sits at the heart of enzymes that help you make energy, build connective tissue, form the protective myelin around nerves, and load iron into red blood cells (see Copper for the full picture of what it does). The adult Recommended Dietary Allowance is roughly 0.9 mg per day, and the tolerable upper intake level for adults is set at about 10 mg per day from food and supplements combined. Because copper is needed in such small amounts, the difference between “enough” and “too much” is narrower than for many nutrients — but the body has a powerful safety valve, described below, that protects almost everyone.
Copper toxicity means there is more copper in the body than it can safely handle. It comes in two very different forms, and keeping them apart is the key to understanding the whole topic:
- Chronic copper overload — almost always Wilson's disease. Wilson's disease (also called hepatolenticular degeneration) is an inherited disorder in which a faulty gene cripples the liver's ability to package copper for disposal. Surplus copper therefore cannot leave the body normally, so it accumulates slowly — first in the liver, then, once the liver is saturated, spilling into the bloodstream and depositing in the brain, eyes, and other organs over years. It is the single most important cause of true, sustained copper toxicity in people, and it is the reason “copper toxicity” and “Wilson's disease” are so often spoken of together.
- Acute copper poisoning — a single large dose. Swallowing a large quantity of a copper compound at once — for example copper sulfate, contaminated water or drinks stored in corroded copper or brass vessels, or industrial/agricultural products — can cause sudden poisoning. This is a different event entirely: instead of a slow build-up over years, it is an immediate chemical injury, beginning in the stomach and intestines. The deep-dive on Nausea & Stomach Upset covers this form in detail.
A few facts about Wilson's disease anchor the rest of this page. It is rare — classically estimated at roughly 1 in 30,000 people, though genetic studies suggest carriers of the gene are more common than once thought. It is caused by mutations in a gene called ATP7B, which a person must inherit from both parents to develop the disease (it is “autosomal recessive”). It usually first appears between the ages of about 5 and 35, although it can show up in young children and in older adults. And, crucially, it is one of the few genetic diseases that is genuinely treatable: caught in time and managed for life, most people with Wilson's disease do very well. Untreated, it is progressive and can be fatal.
It is just as important to say plainly what copper toxicity is not. In a person with normal genes and a normal liver, eating copper-rich foods — shellfish, organ meats, nuts, seeds, dark chocolate — does not cause copper poisoning, because the healthy liver simply excretes the extra. There is a popular notion of widespread “copper toxicity” from diet, cookware, or water supplements that the medical evidence does not support for healthy people. Real chronic overload essentially requires either the inherited inability to clear copper (Wilson's disease) or, very rarely, an extraordinary external exposure. If you have been told you have “copper toxicity,” the right next step is the specific testing described below — not a self-directed cleanse.
Why Excess Copper Is Dangerous
If copper is essential, why is too much of it so harmful? The danger comes down to a single property of the copper atom: it is a redox-active metal, meaning it readily flips back and forth between two charged states (Cu¹⁺ and Cu²⁺), shedding and grabbing electrons as it does. That very property is what makes copper useful inside carefully controlled enzymes — but when free, unbound copper builds up where it should not be, the same chemistry turns destructive.
Here is the idea in plain language. Free copper inside cells catalyzes the formation of reactive oxygen species — aggressive molecules, sometimes called free radicals, that behave like sparks. A few sparks are harmless and even useful for signaling; a steady shower of them is not. These radicals attack the fatty membranes that wrap each cell and its internal compartments, damage proteins, and injure DNA. The cell's antioxidant defenses (which themselves depend on minerals and nutrients) are eventually overwhelmed. This process — copper-driven oxidative stress — is the central mechanism by which copper overload injures tissue, and it has been studied in detail (Gaetke & Chow 2003).
Where this damage lands explains the pattern of Wilson's disease:
- The liver — the first and most common target. Because the liver is where copper is normally processed and where it first piles up, it bears the earliest brunt. The injury can be utterly silent at first — nothing but a rise in liver-enzyme blood tests — then progress to a hepatitis-like inflammation, to scarring (cirrhosis), and, in a minority, to sudden severe liver failure. The Liver Damage deep-dive walks through this whole spectrum.
- The brain — once the liver overflows. When the liver can hold no more, copper enters the bloodstream not safely bound to its carrier protein but as loosely-bound “free” copper, and it deposits in the brain — especially in a region called the basal ganglia that fine-tunes movement. The result can be tremor, stiffness, abnormal postures (dystonia), slurred speech, drooling, clumsiness, and difficulty with fine movements, as well as changes in mood, personality, and thinking. The Neuro & Psychiatric deep-dive explores why these are so easily misdiagnosed.
- The eyes — a visible clue. Copper can deposit at the edge of the cornea, forming a faint golden-brown or greenish ring called a Kayser–Fleischer ring. It usually causes no vision problems but is an important diagnostic sign, especially in people with neurological symptoms.
- The blood and kidneys. A sudden release of copper from a damaged liver can rupture red blood cells, causing a type of anemia (hemolysis). Copper can also injure the kidney's filtering tubules.
In acute poisoning the mechanism is more immediate: a large dose of a copper salt is directly corrosive and irritating to the lining of the stomach and intestines, and, if enough is absorbed, it can overwhelm the liver and red blood cells within hours to days. Either way — slow build-up or sudden dose — the harm traces back to the same root: copper in the wrong place, in the wrong amount, doing oxidative damage.
Why Wilson's Disease Often Stays Silent
One of the most important — and most dangerous — features of Wilson's disease is that it builds up quietly, for years, before it produces any symptom at all. A child can be born with the faulty gene and accumulate copper steadily through childhood while feeling completely well. The liver, with its large reserve capacity, absorbs the rising copper without complaint until it is genuinely overloaded. By the time the first symptom appears — often in the teens or twenties — significant copper has already accumulated. Feeling fine is not the same as being unaffected.
This long silent phase is compounded by a second problem: when symptoms finally do appear, they are notoriously non-specific and easy to attribute to something else. Consider how the early presentations look on their own:
- A teenager with mildly elevated liver enzymes on a routine blood test — easily blamed on a virus, a medication, or, wrongly, on body weight.
- A young adult with a new hand tremor or clumsiness — attributed to anxiety, caffeine, or stress.
- A student with falling grades, irritability, depression, or behavioral change — mistaken for an ordinary mental-health or adolescent issue. A large share of people with Wilson's disease are first seen by a psychiatrist, sometimes for years, before the underlying copper problem is recognized.
- Vague fatigue or appetite loss — the kind of thing anyone might shrug off.
None of these, by itself, shouts “copper.” That is exactly the trap. Because the symptoms are so ordinary-looking and the disease so rare, the average gap between the first symptom and the correct diagnosis can be a year or more — time during which copper keeps accumulating and damage keeps progressing. This is why specialists emphasize a simple rule: Wilson's disease should be actively considered in any unexplained liver disease in a person under 40, and in any young person with an unexplained movement disorder or new psychiatric illness, precisely because you cannot count on the body to make the diagnosis obvious.
The silence has one more dimension worth naming: family members. Because Wilson's disease is inherited, the brothers and sisters of a diagnosed person each have about a 1-in-4 chance of having the disease themselves — and they may be in the long silent phase right now, accumulating copper with no symptoms at all. Guidelines therefore strongly recommend screening first-degree relatives. Catching a sibling before symptoms start is one of the great wins in this disease: treatment begun pre-symptomatically can prevent organ damage entirely.
The take-home message mirrors the one for high potassium and other quiet conditions: a normal-feeling day is not a substitute for the right test. In Wilson's disease, the test — not the symptom — tells the truth.
What Causes Copper to Build Up
Copper accumulates for one of a few reasons, and they are very unevenly common. Understanding them is the best protection against the widespread myth that ordinary diet or cookware causes copper poisoning. Here are the causes worth knowing, roughly from most to least important.
- Wilson's disease (inherited ATP7B mutations) — the overwhelming cause of chronic overload. The ATP7B gene builds a protein that does two jobs in the liver cell: it helps load copper onto its blood-carrier protein (ceruloplasmin) and, critically, it ferries surplus copper into bile so it can leave the body in the stool. When both copies of the gene are faulty, both jobs fail — copper cannot be excreted, so it builds up. More than 600 different mutations in this gene have been described, which is part of why the disease looks so different from one person to the next (Bull et al. 1993; Ferenci et al. 2003). Because two faulty copies are needed, the disease can appear “out of nowhere” in a family where both parents are silent carriers.
- Acute ingestion of a copper compound — the cause of sudden poisoning. Swallowing a large amount of a copper salt at once — most classically copper sulfate (a blue crystalline chemical used in agriculture, swimming pools, and some traditional remedies), or copper-based fungicides — can poison anyone, regardless of genes. This is occasionally accidental (a child swallowing a product), occupational, or, in some parts of the world, an act of deliberate self-harm. It is a true medical emergency.
- Contaminated water or beverages — uncommon, exposure-dependent. Acidic drinks (or simply water) left standing in corroded copper or brass plumbing, kettles, or vessels can pick up enough copper to cause stomach upset, and very rarely more. Modern water systems and standards make significant exposure unusual, but it remains a recognized cause of cluster outbreaks of gastrointestinal illness.
- Other rare childhood copper-overload syndromes. A handful of very rare disorders — such as Indian childhood cirrhosis and idiopathic copper toxicosis — involve copper overload in young children, historically linked to a combination of genetic susceptibility and high copper intake (for example milk stored in copper or brass containers). These are exceptional and largely of historical and regional interest.
- What does not cause it: ordinary diet and cookware in healthy people. This deserves its own line because the misconception is so common. In a person with two working copies of ATP7B, the liver excretes dietary copper surplus efficiently, so copper-rich foods do not cause overload. The small amount that can leach from a well-maintained copper or copper-lined pan during normal cooking is far below harmful levels. High-dose copper supplements taken long-term could in theory push intake past the upper limit, but even that rarely causes clinical toxicity in someone with normal liver function — the body's safety valve is that effective. The honest bottom line: if a healthy person genuinely has high body copper, the search should be for a specific cause, not for blame on everyday food or pots.
A note on copper and zinc, because the two minerals are linked. Copper and zinc compete for absorption in the gut, and very high zinc intake (for example from over-the-counter zinc lozenges or denture creams used in excess) can actually cause copper deficiency — the opposite problem, covered on the Copper Deficiency hub. This same competition is harnessed as a treatment for Wilson's disease, where zinc is given deliberately to block copper absorption — see the treatment section below.
How Copper Toxicity Is Diagnosed
Because copper toxicity is uncommon and Wilson's disease hides so well, diagnosis rests on actively looking for it with the right combination of tests — no single test is perfect on its own. The general lab panels you might have for a check-up can hint at trouble (for instance, abnormal liver enzymes on a Comprehensive Metabolic Panel), but confirming a copper disorder requires specific copper testing. Doctors typically assemble the picture from several pieces (Roberts & Schilsky 2008; EASL 2012):
- Serum ceruloplasmin. Ceruloplasmin is the main copper-carrying protein in the blood. In most people with Wilson's disease it is low, because the faulty liver cannot load copper onto it properly. A low value is a useful clue — but it is not definitive, since it can be normal in some Wilson's patients and low for unrelated reasons, so it is always interpreted alongside other tests.
- Serum copper and “free” (non-ceruloplasmin-bound) copper. Total serum copper can be misleadingly low in Wilson's disease (because so much of the blood's copper normally rides on ceruloplasmin, which is low). What matters more is the free copper — the loosely-bound fraction that does the damage — which tends to be elevated. In acute poisoning, by contrast, serum copper is typically high.
- 24-hour urinary copper. Collecting all urine over a full day and measuring its copper is one of the most informative tests: in Wilson's disease the body tries to dump excess copper through the kidneys, so urinary copper is usually high. This test is also used to monitor treatment over time.
- Slit-lamp eye examination for Kayser–Fleischer rings. An ophthalmologist uses a special microscope to look for the tell-tale copper ring at the edge of the cornea. It is present in most people who already have neurological Wilson's disease, though it can be absent in those whose disease is still confined to the liver.
- Liver biopsy with quantitative copper measurement. When the diagnosis remains uncertain, a small sample of liver tissue can be tested for its actual copper content, which is markedly elevated in Wilson's disease. This is considered one of the strongest pieces of evidence, used selectively.
- Genetic testing. Sequencing the ATP7B gene can confirm the diagnosis by identifying disease-causing mutations, and is especially valuable for screening family members of someone already diagnosed. Because there are hundreds of possible mutations, it is most powerful when the family's specific mutation is already known.
Specialists often combine these into a structured scoring system (the Leipzig criteria) so that no single imperfect test carries the whole decision. The practical message for a patient is reassuring: this is a diagnosable condition. If Wilson's disease is genuinely on the table — an unexplained liver problem in a young person, an unexplained movement disorder, or a sibling of a diagnosed patient — the path forward is a clear, specific work-up, ideally guided by a hepatologist or a center familiar with the disease.
How Copper Overload Is Treated
The two forms of copper toxicity are treated very differently, and it is worth taking them in turn. The good news that runs through both is that copper overload, unlike many genetic and toxic conditions, can usually be controlled — but only with proper medical care, never by self-treatment.
Acute copper poisoning is a medical emergency handled in a hospital. Care is supportive and urgent: protecting the airway and treating shock, replacing fluids lost to vomiting and diarrhea, watching for and treating damage to the red blood cells, liver, and kidneys, and, in severe cases, using a chelating drug (a medicine that binds copper so it can be removed) and occasionally other measures to clear copper from the blood. The key point for the public is simply this: a large copper ingestion is an emergency — seek care immediately and, where available, contact a poison-control service.
Wilson's disease is treated as a lifelong condition, and the strategy has a clear logic: first remove the copper that has accumulated, then keep new copper from building up — for life. The disease cannot be cured (the gene cannot be fixed), but its damage can be halted and often reversed if treatment starts early enough and is never stopped. Stopping treatment, even after years of feeling well, can lead to a dangerous — sometimes fatal — relapse. The main tools are (Roberts & Schilsky 2008; Schilsky et al. 2023; Czlonkowska et al. 2018):
- Chelating agents — to pull copper out. Medicines such as penicillamine and trientine bind the excess copper in the body and carry it out through the urine. They are typically the first step for someone who already has symptoms, working to “de-copper” the body over months. They require careful dosing and monitoring, as they can have side effects — and in a minority of patients with neurological disease, treatment must be introduced cautiously because symptoms can briefly worsen as copper is mobilized.
- Zinc — to block new copper from getting in. Taken as a salt (such as zinc acetate), zinc induces a protein in the gut lining that traps dietary copper inside intestinal cells, which are then shed in the stool — so copper never reaches the bloodstream. Zinc is gentle and is often used for maintenance once the body has been de-coppered, and for treating people who have no symptoms yet (including screened relatives). It is the same copper–zinc competition described in the causes section, turned to therapeutic advantage.
- A lower-copper diet — a supporting role. Patients are usually advised to limit the most copper-dense foods, especially early in treatment — liver and organ meats, shellfish, nuts, chocolate, and mushrooms — and to avoid copper supplements and copper-contaminated water. Diet alone cannot treat Wilson's disease (the problem is excretion, not intake), but it lightens the load the medicines must handle.
- Liver transplantation — for the most severe cases. Because the defect lives in the liver, a transplant effectively corrects the underlying metabolic problem. It is reserved for people with sudden acute liver failure or with advanced cirrhosis that no longer responds to medical therapy — a last resort, but a potentially curative one for the liver disease.
Two themes deserve emphasis. First, early treatment changes the outcome dramatically: a person diagnosed before symptoms (often a screened relative) and treated consistently can expect a normal life expectancy and may never develop organ damage at all. Second, monitoring is lifelong — periodic blood and 24-hour urine copper measurements check that treatment is working and not over-shooting into copper deficiency. As with so much in this disease, the test, not how the person feels, guides the care.
When to Seek Care / Red Flags
Copper toxicity spans a true emergency (acute poisoning) and a slow, hidden disease (Wilson's), so the warning signs differ. The most important “red flag” for Wilson's disease is often a situation rather than a symptom — an unexplained liver problem or movement/psychiatric change in a young person, or being the sibling of someone diagnosed — that should prompt specific testing even if you feel well. Beyond that, the following warrant prompt or emergency medical attention:
- After swallowing a copper product (such as copper sulfate or a copper-based fungicide): a metallic taste, repeated vomiting (sometimes blue-green), severe stomach pain, or any large ingestion — seek emergency care immediately and contact poison control. Do not wait to see if it passes.
- Signs of serious liver trouble: yellowing of the skin or eyes (jaundice), a swollen abdomen, easy bruising or bleeding, vomiting blood, or confusion/extreme drowsiness — these can signal severe liver injury or failure and need urgent assessment.
- New, unexplained neurological symptoms in a young person: a hand tremor, slurred speech, drooling, difficulty with fine movements or walking, stiffness, or abnormal postures — especially when combined with any liver abnormality — deserve evaluation for Wilson's disease.
- Unexplained psychiatric or cognitive change: a marked, out-of-character shift in mood, behavior, personality, or school/work performance in a child, teen, or young adult — particularly alongside any physical sign above — should not simply be assumed to be “just” a mental-health issue without considering a medical cause.
- You have a first-degree relative with Wilson's disease. Ask your doctor about screening even with no symptoms; treatment started before damage begins offers the best possible outcome.
A final word on perspective and honesty. Most people worried about “copper toxicity” from diet, water, or cookware do not have it — the healthy liver is a remarkably good guardian. But genuine copper overload, almost always Wilson's disease, is real, serious, and eminently treatable when found. If your concern is the everyday-diet kind, reassurance and, if needed, simple copper testing are the answer. If your concern is a young person with unexplained liver, movement, or psychiatric problems — or a family history — that is precisely the scenario where pressing for the specific tests above can be life-changing. For the symptom-specific detail, see the Liver Damage and Neuro & Psychiatric deep-dives.
Key Research Papers
- Ala A, Walker AP, Ashkan K, Dooley JS, Schilsky ML (2007). Wilson's disease. The Lancet;369(9559):397-408. — DOI: 10.1016/S0140-6736(07)60196-2
- Czlonkowska A, Litwin T, Dusek P, et al. (2018). Wilson disease. Nature Reviews Disease Primers;4(1):21. — DOI: 10.1038/s41572-018-0018-3
- European Association for the Study of the Liver (2012). EASL Clinical Practice Guidelines: Wilson's disease. Journal of Hepatology;56(3):671-685. — DOI: 10.1016/j.jhep.2011.11.007
- Roberts EA, Schilsky ML (2008). Diagnosis and treatment of Wilson disease: an update. Hepatology;47(6):2089-2111. — DOI: 10.1002/hep.22261
- Roberts EA, Schilsky ML (2003). A practice guideline on Wilson disease. Hepatology;37(6):1475-1492. — DOI: 10.1053/jhep.2003.50252
- Schilsky ML, Roberts EA, Bronstein JM, et al. (2023). A multidisciplinary approach to the diagnosis and management of Wilson disease: 2022 Practice Guidance from the AASLD. Hepatology;77(4):1428-1455. — DOI: 10.1002/hep.32801
- Ferenci P, Caca K, Loudianos G, et al. (2003). Diagnosis and phenotypic classification of Wilson disease. Liver International;23(3):139-142. — DOI: 10.1034/j.1600-0676.2003.00824.x
- Bull PC, Thomas GR, Rommens JM, Forbes JR, Cox DW (1993). The Wilson disease gene is a putative copper transporting P-type ATPase similar to the Menkes gene. Nature Genetics;5(4):327-337. — DOI: 10.1038/ng1293-327
- Gaetke LM, Chow CK (2003). Copper toxicity, oxidative stress, and antioxidant nutrients. Toxicology;189(1-2):147-163. — DOI: 10.1016/S0300-483X(03)00159-8
- Litwin T, Dusek P, Szafranski T, et al. Psychiatric manifestations in Wilson's disease: possibilities and difficulties for diagnosis and treatment. — PubMed
- Gamakaranage CS, et al. Complications and management of acute copper sulphate poisoning; a case discussion. — PubMed
PubMed Topic Searches
- PubMed — Wilson disease: diagnosis, treatment, and management
- PubMed — Copper toxicity, oxidative stress, and the liver
- PubMed — ATP7B gene mutations and copper metabolism
- PubMed — Wilson disease: neurological and psychiatric presentation
- PubMed — Penicillamine, trientine, and zinc therapy in Wilson disease
Connections
- Copper Toxicity: Nausea & Stomach Upset
- Copper Toxicity: Liver Damage
- Copper Toxicity: Neuro & Psychiatric
- Copper Overview
- Copper Deficiency Hub
- Copper Benefits Hub
- Copper, Hemoglobin & Ceruloplasmin
- Copper Toxicity (Toxic Minerals)
- Toxic Minerals Hub
- Zinc
- Iron
- Molybdenum
- Liver Disease
- Cirrhosis
- Neurology
- Comprehensive Metabolic Panel
- Wilson's Disease — the inherited disorder that causes almost all chronic copper overload.