Calcium Chloride
Calcium chloride is one of the substances that appeared in the 1926 U.S. Dispensatory with a hopeful but mistaken theory behind it. Doctors of that era sometimes gave it by mouth to "acidify the body" when a person was thought to be "too alkaline," in the belief that this would calm itching, allergies, and asthma. That idea was wrong — and it is worth saying so plainly, because a version of it still circulates today as the "alkaline body" or "acid/alkaline" theory of disease. Your blood is held within a razor-thin pH window no supplement can move. The real, life-saving uses of calcium chloride turned out to be entirely different: it is an emergency intravenous (IV) drug given in a hospital for dangerously low blood calcium, for the heart-protecting treatment of high potassium, for magnesium overload, and as an antidote in certain heart-medication overdoses. This page tells the honest history, debunks the acid/alkaline myth with modern evidence, explains what calcium chloride genuinely does today, and is clear about why it is a caustic drug you should never improvise with at home. It is a companion to our broader Calcium page, which covers the mineral itself.
Table of Contents
- What Calcium Chloride Actually Is
- Historical Medical Use (1926 U.S. Dispensatory)
- The Acid/Alkaline-Body Myth, Debunked
- Real IV Emergency Uses
- Calcium Chloride vs. Calcium Gluconate
- Industrial & Food Uses (E509)
- How It's Used Today
- Safety, Cautions & Myths
- Key Research Papers
- Connections
- Featured Videos
What Calcium Chloride Actually Is
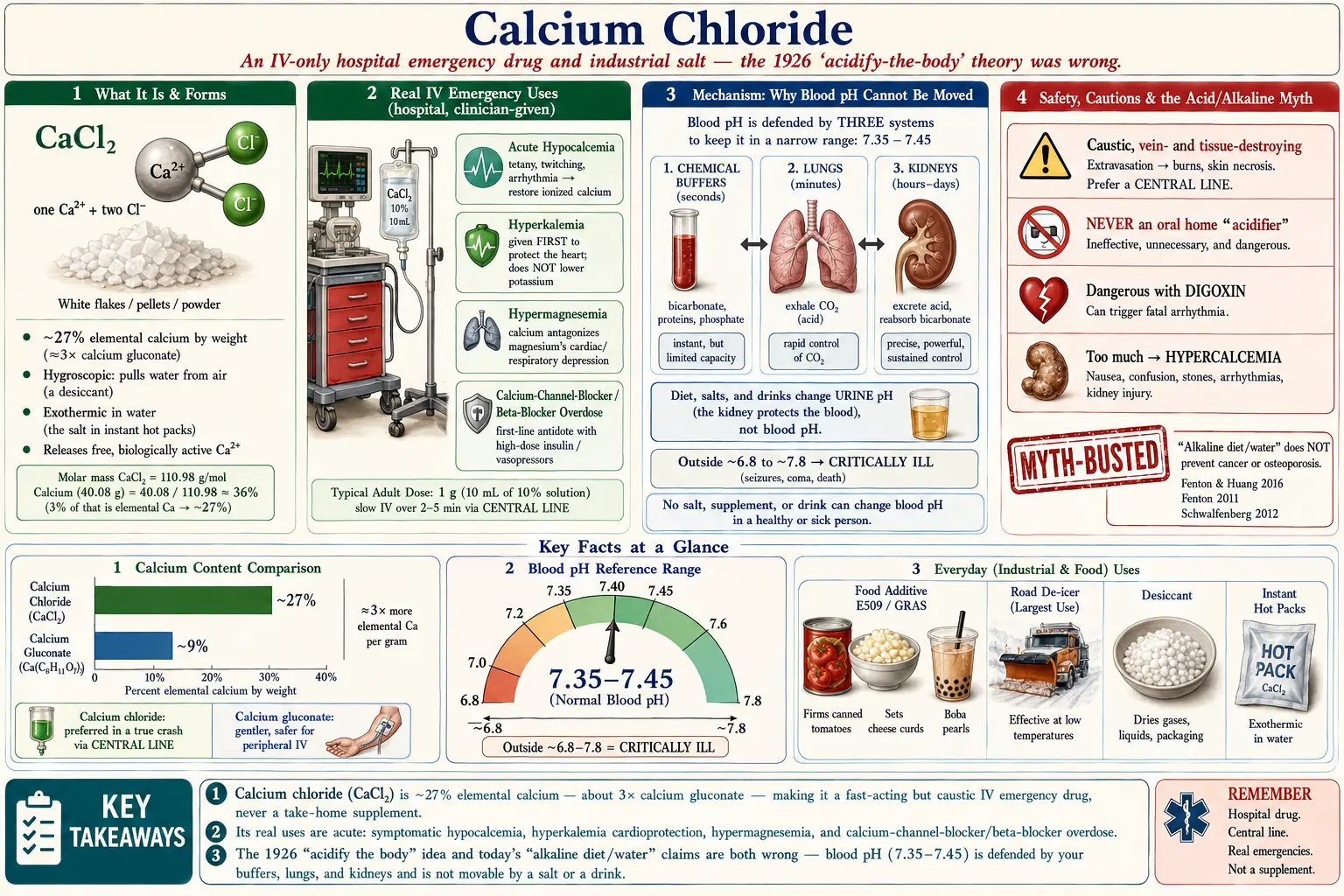
Calcium chloride is a simple salt with the formula CaCl2: one calcium ion paired with two chloride ions. As a dry solid it usually comes as white flakes, pellets, or powder, and it is strongly hygroscopic — meaning it pulls water straight out of the air so eagerly that it is used as a drying agent (desiccant) and clumps if you leave the lid off. When it dissolves in water it gives off noticeable heat (an exothermic reaction), which is exactly why it is the salt inside many instant "hot packs."
Chemically, calcium chloride matters because of what it does once it splits apart in solution. It releases free calcium ions (Ca2+) — the same biologically active form your body uses to fire nerves, contract muscle, clot blood, and run countless cell-signaling pathways (all covered on the main Calcium page). Compared with most other calcium salts, calcium chloride delivers a relatively large amount of that active calcium per gram: roughly 27% elemental calcium by weight (about three times more, gram for gram, than calcium gluconate). That high, immediately available calcium content is the whole reason it is useful as an emergency drug — and also the reason it is harsh on tissues, as you will see in the safety section.
It is the same compound whether it is keeping a road from icing over, firming up canned tomatoes, or sitting in an ampule in a crash cart. The dose, the purity grade, and the route of delivery are what separate a de-icer from a medicine.
Historical Medical Use (1926 U.S. Dispensatory)
In the early twentieth century, before the chemistry of body pH was well understood, physicians had a theory that many complaints stemmed from the body being "too alkaline," and that gently "acidifying" a patient might help. Because calcium chloride leaves an acidic residue when it is metabolized (the body handles the chloride in a way that can nudge the blood very slightly toward acid), it was reached for as a mild systemic acidifier. Doctors of that era used oral calcium chloride to try to relieve conditions thought to be "allergic" or driven by excess alkalinity — things like itching (urticaria/hives), allergic reactions, and asthma. There was also a related belief that calcium given under acidic conditions helped relax muscle spasm, drawing on the genuine observation that very low blood calcium causes muscles to twitch and cramp (a state called tetany).
It is fair and accurate to report this as history: in 1926, this is what some physicians believed and did. Two strands of that thinking even contained a kernel of real biology — calcium truly is essential for normal nerve and muscle function, and severe calcium deficiency really does cause spasm. But the framing — that you treat disease by shifting the body's overall acid/alkaline balance with a salt — was mistaken. The next section explains why, using what we have since learned about how the body actually controls its pH.
The Acid/Alkaline-Body Myth, Debunked
This is the most important correction on the page, because the same idea is still sold today — as "alkaline diets," "alkaline water," pH test strips, and warnings that your body is "too acidic." Whether the 1926 version aimed to acidify you or the modern version aims to alkalinize you, the underlying premise is the same, and it is not how human physiology works.
Your blood pH is held within an extraordinarily tight range, about 7.35 to 7.45 — slightly alkaline, and almost completely non-negotiable. The body defends this set point with three powerful systems working continuously:
- Chemical buffers (mainly the bicarbonate system, plus proteins and phosphate) soak up excess acid or base within seconds.
- The lungs adjust how much carbon dioxide you breathe off within minutes — exhale more and you become slightly more alkaline; exhale less and you become slightly more acidic. This is a fast, second-by-second pH dial.
- The kidneys fine-tune things over hours to days by deciding how much acid and bicarbonate to keep or dump in the urine.
The practical upshot: you cannot meaningfully "acidify" or "alkalinize" your blood with a supplement, a salt, or a diet. If your blood pH actually drifted outside roughly 6.8–7.8, you would be critically ill in a hospital — that is not a "wellness" state you nudge with capsules. What food and salts can change is the pH of your urine, because the kidney is the very organ doing the dumping. That is real, and it is exactly why diet can be used clinically to make urine more alkaline (helpful for certain kidney stones or to speed clearance of some drugs) — Kanbara and colleagues showed dietary change shifts urine pH and uric-acid handling. But shifting urine pH is the kidney protecting your blood pH, not evidence that the blood itself has been moved.
The broader "acid/alkaline theory of disease" — the claim that an "acidic body" causes cancer, osteoporosis, and chronic illness, and that alkalizing reverses them — has been examined directly and does not hold up. A systematic review by Fenton and Huang (2016) found no evidence that an alkaline diet or alkaline water prevents or treats cancer. Earlier, Fenton and colleagues (2011) applied formal causal criteria to the "acid-ash" idea that dietary acid leaches calcium from bone and causes osteoporosis, and found the hypothesis was not supported — the body does not sacrifice your skeleton to buffer your dinner. Schwalfenberg's (2012) review reached the same overall conclusion: while eating more vegetables and fruit is genuinely good for you, the benefit is not because they "alkalize your blood." There is one honest sliver of truth worth keeping: tumor cells create an acidic local micro-environment in the tissue immediately around them, and there is active cancer research into that micro-environment — but that is a localized tissue effect, the opposite causal direction, and it has nothing to do with the pH of your whole body or with drinking alkaline water.
So the 1926 logic was upside down in two ways: blood pH cannot be steered by a salt, and "balancing" body acidity is not a real treatment for hives, allergies, or asthma. Modern allergy and asthma care uses antihistamines, inhaled corticosteroids, bronchodilators, and (where appropriate) epinephrine — not pH manipulation.
Real IV Emergency Uses
Here is where calcium chloride earns its place in medicine. Given intravenously, in a hospital, by clinicians, it is a genuine emergency drug. Its value comes from flooding the bloodstream quickly with active calcium ions. The main uses are:
- Symptomatic low blood calcium (acute hypocalcemia). When ionized calcium drops far enough to cause tetany (muscle spasms, twitching, tingling around the mouth and fingers), seizures, or — most dangerously — heart-rhythm changes, IV calcium quickly restores it. This can happen after neck/thyroid surgery, in critical illness, after large transfusions (the citrate preservative in stored blood binds calcium), or in severe pancreatitis. This is the use that connects, distantly, to the old "tetany" observation — except the modern version is precise: measure the calcium, then replace it.
- High blood potassium (hyperkalemia) — to protect the heart. Severely elevated potassium can make the heart's electrical activity dangerously unstable and cause fatal arrhythmias. IV calcium is given first in emergency hyperkalemia to stabilize the heart and buy time, while other treatments (insulin with glucose, etc.) actually lower the potassium. Importantly, calcium does not lower the potassium level itself — it is cardioprotective cover. Recent work by Piktel and colleagues (2024) even challenges the old textbook explanation that calcium "stabilizes the membrane," suggesting the mechanism is more nuanced than taught — but the clinical benefit of giving calcium in this setting remains standard practice (Kumar and colleagues, 2025, systematic review).
- Magnesium overload (hypermagnesemia). Too much magnesium — for example from over-aggressive magnesium therapy in kidney failure or in obstetric care — can depress the heart and breathing. IV calcium directly antagonizes magnesium's effects and is the immediate counter-measure.
- Calcium-channel-blocker and beta-blocker overdose. These common heart and blood-pressure medications, in overdose, can drop the heart rate and blood pressure to lethal levels. IV calcium is one of the first-line antidotes — especially for calcium-channel-blocker poisoning, where giving extra calcium can help overcome the blockade — alongside therapies like high-dose insulin and vasopressors (Suarez, Koyfman, and Long, 2026).
Notice the pattern: every legitimate use is an acute, measured, monitored intervention for a specific, often life-threatening derangement — not a daily tonic, and never about "body pH."
Calcium Chloride vs. Calcium Gluconate
In the hospital, calcium comes in two main IV forms, and the choice matters. Calcium chloride contains about three times more elemental calcium per equal volume than calcium gluconate, so it raises blood calcium faster and is often preferred in a true crash (for example, cardiac arrest with hyperkalemia, given through a central line). The trade-off is that calcium chloride is far more irritating and damaging to veins and tissue. Calcium gluconate is gentler, much safer if it leaks out of a vein, and is the usual choice when calcium can be replaced through a regular peripheral IV at a steadier pace. Neither is an oral home product for these purposes; both are prescription IV drugs. This is purely a clinical decision — there is no version of this choice that applies to taking calcium for everyday bone health, which is covered on the Calcium page.
Industrial & Food Uses (E509)
Most of the calcium chloride made in the world never goes near medicine. Being honest about these everyday uses helps put the "supplement" idea in perspective — this is, first and foremost, a bulk industrial chemical.
- Road de-icer and dust control. Because it lowers the freezing point of water and gives off heat as it dissolves, calcium chloride is spread on roads to melt ice and is used to keep gravel roads from getting dusty. This is its single largest use.
- Food additive E509 (a firming agent and stabilizer). In food, calcium chloride is a recognized additive, labeled E509 in Europe and "generally recognized as safe" (GRAS) by the U.S. FDA at the small amounts used. It keeps canned vegetables (tomatoes, beans, pickles) crisp, supplies the calcium that makes cheese curds set, is the salt used in making the gel "pearls" of molecular gastronomy and bubble-tea popping boba, and is added to some bottled and brewing water to adjust mineral content. It is also the saltiness and mild bitterness you taste in some electrolyte products. Used this way it is safe — but eating canned tomatoes is not "supplementing calcium chloride" in any meaningful medical sense.
- Desiccant and concrete additive. Its thirst for water makes it a common drying agent (those moisture-absorbing tubs for damp closets), and it is added to concrete to make it set faster.
- Instant hot packs. The heat released when it dissolves is harnessed in self-heating packs and some self-heating meals.
How It's Used Today
Putting it together, here is the honest modern picture:
- As a medicine, calcium chloride is an IV-only, hospital-only emergency drug for the specific situations above — acute symptomatic hypocalcemia, hyperkalemia cardioprotection, hypermagnesemia, and calcium-channel-blocker/beta-blocker overdose. Dosing is weight- and situation-specific, titrated to lab values and the heart monitor by trained clinicians. There is no general-purpose, take-home, "feel-better" dose.
- For ordinary calcium needs — building and maintaining bone, covering dietary shortfalls — calcium chloride is not the supplement people use. Oral supplements use gentler salts such as calcium carbonate (cheap, take with food) and calcium citrate (absorbed even without stomach acid). See the Calcium page for how to meet calcium needs sensibly, ideally from food first.
- In everyday life, you most often encounter it as a food-firming additive (E509), a de-icer, a desiccant, or the warmth in a hot pack.
The bottom line on "use today": treat calcium chloride as a hospital drug and an industrial salt — not as a wellness supplement, and absolutely not as a way to change your body's pH.
Safety, Cautions & Myths
This is the section the original 1926-style enthusiasm leaves out, and it is the part that matters most.
- IV calcium chloride is caustic and can destroy tissue. It is highly concentrated and irritating to veins. If it leaks out of the vein into surrounding tissue (a complication called extravasation), it can cause severe burns, skin death (necrosis), and the deposit of calcium in the tissue — sometimes needing surgery. For this reason it is preferentially given through a central line rather than a small arm vein, and slowly. Documented case reports describe serious skin necrosis after calcium chloride extravasation (Lin and colleagues, 2007; reviewed among irritant non-cytotoxic drugs by Le and Patel, 2014).
- It is not an oral "acidifier" you should ever improvise. Swallowing concentrated calcium chloride irritates and can burn the mouth, throat, and stomach, and using it to chase a pH theory has no benefit and real risk. The acid/alkaline-body premise behind that use is, as explained above, pseudoscience.
- Too much calcium, too fast, is dangerous. Rapid IV calcium can itself trigger heart-rhythm problems and a feeling of intense heat. It is especially hazardous in someone taking digoxin, where extra calcium can precipitate fatal arrhythmias. This is one of many reasons it belongs only in monitored medical hands.
- High blood calcium (hypercalcemia) has its own harms. Overshooting calcium — whether by IV or, in a different context, by chronic over-supplementation with oral calcium — can cause nausea, confusion, constipation, kidney stones, and heart-rhythm disturbances. More is not better.
- Myth: "balancing body acidity" treats allergies, asthma, or disease." It does not. Real allergy/asthma treatment is described above; real disease prevention comes from a good overall diet, not from chasing pH.
- Myth: "alkaline water/diet changes your blood pH and prevents cancer or osteoporosis." The blood pH is defended by your lungs and kidneys and is not movable by drinks or salts; the cancer and bone claims are not supported by evidence (Fenton & Huang 2016; Fenton 2011; Schwalfenberg 2012). Eat the vegetables — just not for the pH reason.
- Industrial-grade is not food- or medical-grade. De-icer and desiccant calcium chloride may contain impurities and is never to be consumed. Only food-grade (E509) belongs in food, and only pharmaceutical-grade, prescribed and administered by clinicians, belongs in a vein.
If you are worried about your calcium, your potassium, or symptoms like muscle cramps, tingling, or palpitations, that is a reason to get tested and seen — a comprehensive metabolic panel measures these electrolytes — not a reason to buy a salt and self-treat.
Key Research Papers
Every citation below was checked against Crossref or PubMed. Author, title, and journal are plain text; only the year/volume/pages is the working link.
- Suarez F, Koyfman A, Long B. Pearls and Pitfalls for the Emergency Clinician: Beta Blocker and Calcium Channel Blocker Toxicity. Journal of Emergency Medicine. 2026;84:1–11. — Reviews emergency management of calcium-channel-blocker and beta-blocker overdose, including the role of IV calcium as a first-line antidote. (PMID: 41833262)
- Piktel JS, Wan X, Kouk S, et al. Beneficial Effect of Calcium Treatment for Hyperkalemia Is Not Due to "Membrane Stabilization". Critical Care Medicine. 2024;52(10):1499–1508. — Confirms calcium's cardioprotective benefit in hyperkalemia while challenging the classic "membrane-stabilization" explanation. (PMID: 39046789)
- Kumar M, Ahmad R, Arslan FS, et al. Managing Hyperkalemia in Heart Failure Patients: A Systematic Review. Cardiology in Review. 2025 (online ahead of print). — Systematic review of acute and chronic hyperkalemia management, situating IV calcium as immediate cardioprotection. (PMID: 41233949)
- Fenton TR, Huang T. Systematic review of the association between dietary acid load, alkaline water and cancer. BMJ Open. 2016;6(6):e010438. — Found no evidence that an alkaline diet or alkaline water prevents or treats cancer; a direct rebuttal of the acid/alkaline-body theory. (PMID: 27297008)
- Fenton TR, Tough SC, Lyon AW, Eliasziw M. Causal assessment of dietary acid load and bone disease: a systematic review & meta-analysis applying Hill's epidemiologic criteria for causality. Nutrition Journal. 2011;10:41. — The "acid-ash" claim that dietary acid leaches calcium from bone and causes osteoporosis is not supported by the evidence. (PMID: 21529374)
- Schwalfenberg GK. The alkaline diet: is there evidence that an alkaline pH diet benefits health? Journal of Environmental and Public Health. 2012;2012:727630. — Reviews the alkaline-diet literature; benefits of more produce are real, but not because of "alkalinizing the blood." (PMID: 22013455)
- Kanbara A, Miura Y, Hyogo H, Chayama K, et al. Effect of urine pH changed by dietary intervention on uric acid clearance. Nutrition Journal. 2012;11:39. — Demonstrates that diet shifts urine pH (the kidney's doing), illustrating why blood pH itself is not what changes. (PMID: 22676161)
- Le A, Patel S. Extravasation of noncytotoxic drugs: a review of the literature. Annals of Pharmacotherapy. 2014;48(7):870–886. — Reviews tissue injury from extravasated irritant drugs, including concentrated calcium salts. (PMID: 24714850)
- Lin CY, Hsieh KC, Yeh MC, et al. Skin necrosis after intravenous calcium chloride administration as a complication of parathyroidectomy. Surgery Today. 2007;37(9):778–781. — Case report of severe skin necrosis from IV calcium chloride, underscoring its caustic, sclerosing nature. (PMID: 17713732)
Live PubMed Searches
- Calcium chloride & hyperkalemia treatment
- Calcium-channel-blocker overdose & calcium
- Acute hypocalcemia management
- Alkaline diet & acid-base disease claims
- Calcium chloride extravasation & necrosis
- Hypermagnesemia & calcium treatment
Connections
- Calcium — the mineral itself: bone, muscle, nerves, clotting, and how to meet your needs.
- Magnesium — the electrolyte calcium counters in hypermagnesemia.
- Potassium — high potassium (hyperkalemia) is a key IV-calcium emergency.
- Phosphorus & Acid-Base Balance — how the body actually buffers pH.
- Sodium — the other major electrolyte the body regulates closely.
- Arrhythmia — the heart-rhythm danger behind hyperkalemia and drug overdose.
- Kidney Disease — the kidneys defend blood pH and clear electrolytes.
- Comprehensive Metabolic Panel — the blood test that measures calcium, potassium, and CO2.
- Magnesium Test — measuring magnesium status.
- All Minerals — the full minerals index.