Anti-dsDNA (Lupus Antibody)
Anti-double-stranded DNA — usually written anti-dsDNA — is a blood test that looks for an antibody your immune system is not supposed to make: one that targets your own genetic material. Normally antibodies patrol for germs. In lupus, some of them turn inward and bind the double-stranded DNA inside your own cells. That is why a positive result is meaningful: this particular antibody is strongly tied to systemic lupus erythematosus (SLE, or lupus) and shows up in relatively few other conditions.
If you have been told your ANA test was positive and your doctor has now ordered anti-dsDNA, that is a very normal next step, not a sign that something new has gone wrong. This page explains, in plain language, what the test is, why it is ordered, how it fits into the workflow that starts with a positive ANA, how doctors use rising and falling levels to follow lupus over time (especially when the kidneys are involved), how the lab actually measures it, and how to read your result honestly — including the important fact that a negative test does not rule lupus out. Lupus is a serious, lifelong illness, and getting a clear picture of what this one number can and cannot say is part of feeling less lost in the process.
Table of Contents
- What Anti-dsDNA Is
- Why It Is Ordered: Lupus and Specificity
- The ANA → Anti-dsDNA Workflow
- Lupus Nephritis and Tracking Disease Activity
- How It Is Measured
- How to Interpret Your Result
- Anti-dsDNA in the Classification Criteria
- Related Tests Ordered Alongside It
- When to Talk to a Doctor
- Research Papers
- Connections
- Featured Videos
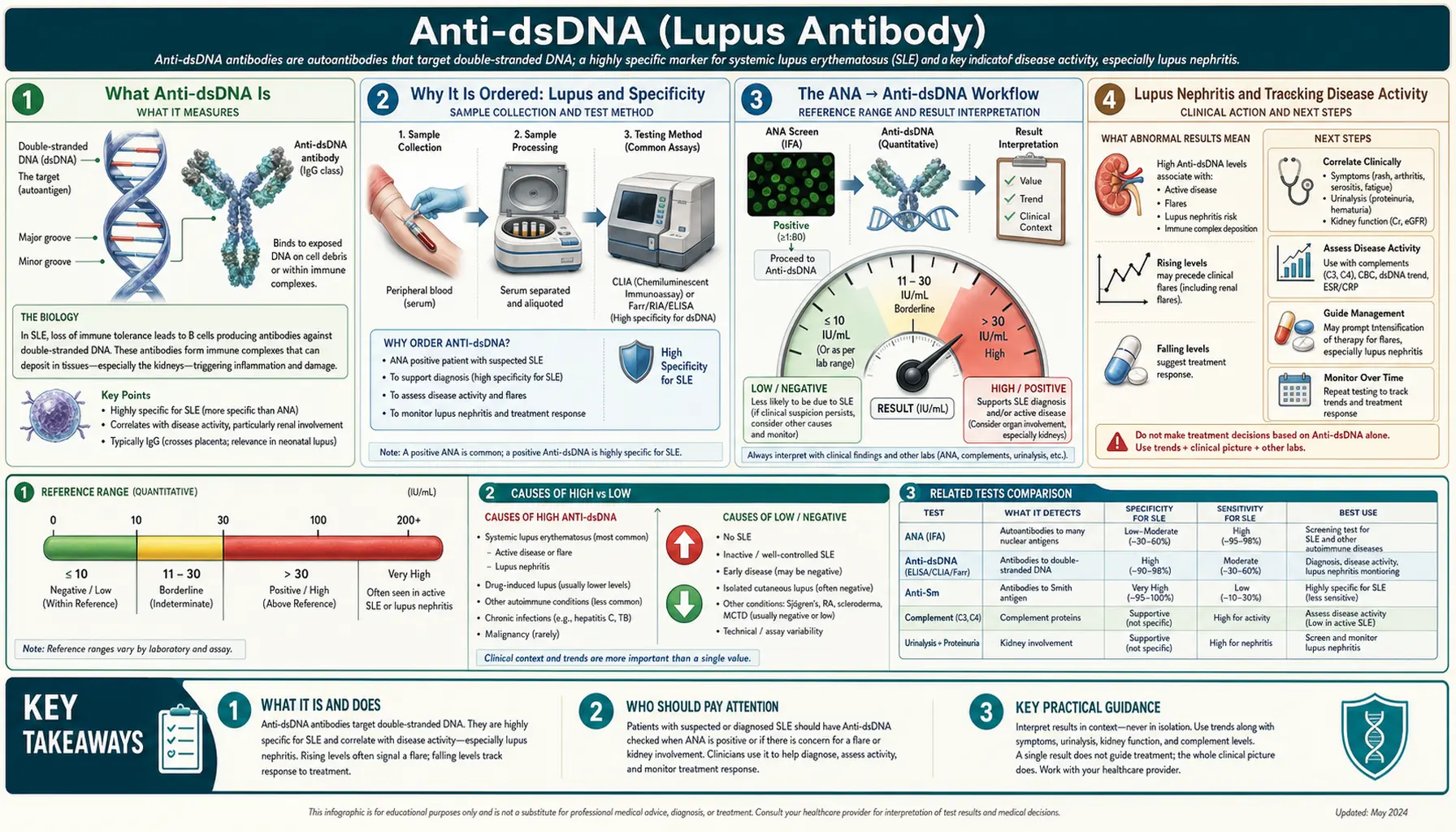
What Anti-dsDNA Is
Every cell in your body stores its instructions on DNA, and that DNA is wound into a double strand — the famous double helix. An anti-dsDNA antibody is an antibody (an autoantibody, meaning “self-targeting”) that binds to that double-stranded DNA. In a healthy immune system this should not happen; the body learns early on to tolerate its own tissues and DNA. When tolerance breaks down, as it does in lupus, the immune system starts producing antibodies against self.
It helps to keep two related terms apart:
- Anti-dsDNA targets double-stranded (native) DNA. This is the one closely linked to lupus and the subject of this page.
- Anti-ssDNA targets single-stranded DNA. It is far less specific — it turns up in many conditions and even in some healthy people — so it is not used the same way and is rarely ordered on its own.
The reason anti-dsDNA matters clinically is not just that it flags an autoimmune process. These antibodies appear to take part directly in the tissue damage of lupus, particularly in the kidney, where DNA-containing immune complexes deposit and trigger inflammation. That is part of why the test does double duty: it both helps identify lupus and helps follow how active the disease is.
Why It Is Ordered: Lupus and Specificity
The headline reason to order anti-dsDNA is lupus. To understand why it is so useful, it helps to think about two qualities every test has: sensitivity and specificity.
- Sensitivity is how good a test is at catching people who truly have the disease. A very sensitive test rarely misses cases.
- Specificity is how good a test is at staying negative in people who do not have the disease. A very specific test rarely raises a false alarm.
The ANA (antinuclear antibody) test is highly sensitive for lupus — almost everyone with lupus has a positive ANA — but it is not specific. A positive ANA also shows up in other autoimmune diseases, in some infections, in a number of healthy people (especially women and older adults), and sometimes for no clear reason at all. So a positive ANA raises the question but rarely answers it.
Anti-dsDNA is the mirror image on the specificity side. It is one of the most specific antibodies for lupus — when it is genuinely present at a meaningful level, lupus becomes a much stronger explanation, because relatively few other conditions produce it. The trade-off is that anti-dsDNA is not very sensitive: only somewhere around half to two-thirds of people with lupus test positive, and levels can rise and fall over time. In short, a positive anti-dsDNA carries a lot of weight, while a negative anti-dsDNA settles very little. That combination — sensitive ANA up front, specific anti-dsDNA to confirm — is exactly why doctors use them together.
The ANA → Anti-dsDNA Workflow
Lupus testing follows a logical sequence, and knowing it can make the string of blood draws feel less arbitrary.
- Step 1 — ANA as the screen. Because ANA is so sensitive, it is the gatekeeper. If someone has symptoms that could be lupus — a facial rash, joint pain, unexplained fatigue, mouth sores, hair loss, kidney findings — the ANA is checked first. A negative ANA makes lupus quite unlikely and often redirects the search elsewhere.
- Step 2 — specific antibodies to confirm. If the ANA is positive and the clinical picture fits, the doctor orders the lupus-specific antibodies to firm up the diagnosis. The two classic confirmatory ones are anti-dsDNA and anti-Sm (anti-Smith). Anti-Sm is even more specific for lupus but appears in fewer patients; anti-dsDNA is more common and has the bonus of tracking disease activity.
- Step 3 — supporting labs. Alongside the antibodies, the doctor usually checks complement (C3 and C4), a urinalysis for protein and blood, kidney function, and a complete blood count. These fill in whether the immune system is actively consuming complement and whether organs like the kidney are affected.
So anti-dsDNA is almost never a standalone test. It is the confirmatory move that follows a positive screen, interpreted next to the rest of the panel and, above all, next to how you actually feel and what the exam shows.
Lupus Nephritis and Tracking Disease Activity
This is the part of anti-dsDNA that is genuinely, day-to-day useful — and it goes beyond diagnosis. In many people with lupus, anti-dsDNA levels move with the disease: they tend to rise when lupus is flaring and fall when treatment brings it under control. That makes the test a way to monitor lupus over months and years, not just to label it once.
The organ where this matters most is the kidney. Lupus nephritis — inflammation of the kidney driven by lupus — is one of the more serious complications, and it can be quiet, causing little that you would notice until it is advanced. Anti-dsDNA antibodies are thought to be directly involved in the kidney injury, forming immune complexes with DNA that lodge in the filtering units and set off inflammation. Because of that link, a rising anti-dsDNA level is one of the warning flags clinicians watch for kidney involvement.
Two other numbers usually move in step with it during a flare:
- Falling complement (C3 and C4). Complement proteins get used up when immune complexes are actively driving inflammation, so their levels drop when lupus is active. A pattern of rising anti-dsDNA together with falling C3/C4 is a classic signature of an active flare, especially in the kidney. See Complement (C3, C4, CH50) for how those are measured.
- Protein in the urine. When the kidney filter is inflamed, protein leaks into the urine. New or worsening proteinuria on a urinalysis, alongside rising anti-dsDNA and dropping complement, strongly points at active lupus nephritis and often prompts closer evaluation.
A fair caution: the relationship between anti-dsDNA and flares is real but not perfect. Some people run persistently high levels while feeling well; others flare with only modest changes. That is why doctors read the trend in one person over time, using the same lab and method, rather than treating a single number as a verdict. A rising titer is a reason to look harder, not an automatic diagnosis of a flare.
How It Is Measured
Anti-dsDNA is a simple blood draw for you, but behind the scenes the lab can measure it in several different ways, and the method affects the answer. The three traditional approaches are:
- Farr assay (radioimmunoassay). An older, highly regarded method that detects high-strength (high-avidity) antibodies. It tends to be very specific and correlates well with disease activity, but it uses radioactive materials, so fewer labs run it today.
- ELISA (enzyme-linked immunosorbent assay). The most common modern method. It is convenient, automated, and sensitive, but somewhat less specific — it can pick up lower-strength antibodies that are less tied to active disease, which is one reason a mildly positive ELISA is interpreted cautiously.
- Crithidia luciliae immunofluorescence (CLIFT). This test uses a single-celled organism whose whip-like tail structure (the kinetoplast) is packed with pure double-stranded DNA. If your serum lights up that structure under the microscope, you have genuine anti-dsDNA. It is very specific and is often used to confirm a positive ELISA.
The practical takeaways are worth keeping in mind. First, results come as a number (a titer or units), and because the methods differ, a value from one lab is not directly interchangeable with a value from another. Second, when a result is borderline or does not match the clinical picture, labs and doctors may cross-check with a second method (for example, confirming an ELISA with Crithidia). Third, for tracking your disease over time, it is best to stay with the same lab and the same method so that a change reflects your biology rather than a switch in technique.
How to Interpret Your Result
Reference ranges vary by lab and by method, so your report will state its own cutoff for “negative,” “borderline/equivocal,” and “positive.” Always read your result against the range printed on your report. With that in mind, here is how to think about the common scenarios:
- A clearly positive result supports a diagnosis of lupus, particularly when you also have a positive ANA and symptoms that fit. It does not, by itself, prove lupus — the result always has to fit the whole clinical picture — but it moves the needle substantially.
- A high or rising level with low complement and protein in the urine is the pattern that most concerns doctors: together these strongly suggest active lupus, often with kidney involvement. This combination usually triggers a closer look and sometimes a change in treatment.
- A negative result does not rule out lupus. This is the single most important caveat. Because anti-dsDNA is specific but not very sensitive, a large minority of people with lupus test negative — and someone who was positive during a flare can turn negative once treatment calms the disease. A negative test is reassuring evidence, not an all-clear.
- A borderline or low-positive result is common and often just means “keep watching.” It may be rechecked, confirmed by a second method, or simply followed over time, especially if you feel well and the rest of the panel is normal.
- A stable, modestly elevated level in someone who feels well does not necessarily call for a change in treatment. Some people carry a steady positive without active disease, which is exactly why the trend and your symptoms matter more than any one snapshot.
The honest summary: anti-dsDNA is a strong piece of evidence, not a switch that turns lupus on or off. It is most powerful when read together with your ANA, complement, urine findings, blood counts, and — most of all — how you are actually doing.
Anti-dsDNA in the Classification Criteria
Anti-dsDNA is important enough that it is written into the formal classification criteria that experts use to define lupus for research and, informally, to structure diagnosis. In the 2019 EULAR/ACR criteria, a positive ANA is the required entry point — the gate you must pass through — and then various clinical and laboratory features are scored and added up. Anti-dsDNA sits in the immunology section and carries meaningful weight, especially when it appears with the low-complement pattern.
A word of care about what “classification criteria” really are: they were designed mainly to make sure research studies enroll comparable patients, not to diagnose an individual in the clinic. Real diagnosis is a judgment made by an experienced clinician weighing your whole story. Still, the criteria are useful shorthand for understanding why your doctor is checking these particular antibodies and what each one contributes. If you would like to go deeper, see ACR/EULAR 2019 Classification Criteria for SLE.
Related Tests Ordered Alongside It
Anti-dsDNA rarely travels alone. To make sense of it, doctors line it up next to several other tests, each answering a different question:
- ANA (antinuclear antibody) — the sensitive screening test that usually comes first and sets the stage.
- Anti-Sm (anti-Smith) — the other highly specific lupus antibody, often ordered together with anti-dsDNA as part of an extractable-nuclear-antigen panel.
- Complement (C3, C4, CH50) — falling levels signal active immune-complex disease and pair with rising anti-dsDNA during flares.
- Urinalysis and urine protein — the earliest window on whether the kidneys are involved. See also Microalbumin & ACR for quantifying urine protein.
- Complete Blood Count (CBC) — lupus can lower white cells, red cells, or platelets, so the CBC helps gauge activity and safety.
- Kidney function tests (creatinine, eGFR) — to check how well the kidneys are filtering.
Other autoimmune antibody tests such as Rheumatoid Factor and the ANCA test target different diseases, but they sometimes come up in the same evaluation when the diagnosis is not yet clear.
When to Talk to a Doctor
This test is ordered and interpreted by a clinician — usually a rheumatologist — and the result on its own is not something to act on alone. It is worth reaching out to your doctor if:
- You have symptoms that could suggest lupus — a butterfly-shaped facial rash, joint pain and swelling, unexplained fatigue, mouth ulcers, hair loss, chest pain when breathing, or a rash that flares in sunlight — and want to know whether testing makes sense.
- Your ANA has come back positive and you are unsure what the follow-up tests, including anti-dsDNA, are looking for.
- You already have a lupus diagnosis and your anti-dsDNA is rising, especially if you also notice swelling in your legs or around your eyes, foamy urine, or new fatigue — these can be early signs of kidney involvement worth prompt attention.
- You are confused by a positive result while feeling well, or a negative result despite feeling unwell — both happen, and both deserve a real conversation rather than a single number.
Lupus can be frightening to face, but it is a manageable condition for most people, and treatment has improved a great deal. Understanding what anti-dsDNA does and does not tell you is one small way to walk into that conversation feeling more informed and less alone. Bring your questions; a good clinician will welcome them.
Research Papers
- Aringer M, Costenbader K, Daikh D, et al. 2019 European League Against Rheumatism/American College of Rheumatology classification criteria for systemic lupus erythematosus. Arthritis & Rheumatology. 2019;71(9):1400–1412. doi:10.1002/art.40930 — the current classification criteria; a positive ANA is the entry gate and anti-dsDNA carries substantial weight in the immunology domain.
- Fanouriakis A, Kostopoulou M, Alunno A, et al. 2019 update of the EULAR recommendations for the management of systemic lupus erythematosus. Annals of the Rheumatic Diseases. 2019;78(6):736–745. doi:10.1136/annrheumdis-2019-215089 — management guidance that uses anti-dsDNA and complement to gauge activity and steer therapy.
- Kavanaugh AF, Solomon DH. Guidelines for immunologic laboratory testing in the rheumatic diseases: anti-DNA antibody tests. Arthritis Care & Research. 2002;47(5):546–555. doi:10.1002/art.10558 — a foundational guideline on when and how anti-DNA testing is genuinely useful.
- Isenberg DA, Manson JJ, Ehrenstein MR, Rahman A. Fifty years of anti-ds DNA antibodies: are we approaching journey’s end? Rheumatology. 2007;46(7):1052–1056. doi:10.1093/rheumatology/kem112 — a readable retrospective on what anti-dsDNA does and does not tell us.
- Pisetsky DS. Anti-DNA antibodies — quintessential biomarkers of SLE. Nature Reviews Rheumatology. 2016;12(2):102–110. doi:10.1038/nrrheum.2015.151 — why anti-dsDNA is such a defining marker and the biology behind it.
- Rahman A, Isenberg DA. Systemic lupus erythematosus. New England Journal of Medicine. 2008;358(9):929–939. doi:10.1056/NEJMra071297 — a clear, comprehensive overview of lupus.
- Tsokos GC. Systemic lupus erythematosus. New England Journal of Medicine. 2011;365(22):2110–2121. doi:10.1056/NEJMra1100359 — a mechanism-focused review of how lupus damages tissue.
- Hahn BH. Antibodies to DNA. New England Journal of Medicine. 1998;338(19):1359–1368. doi:10.1056/NEJM199805073381906 — a classic review of anti-DNA antibodies and their clinical meaning.
- Linnik MD, Hu JZ, Heilbrunn KR, et al. Relationship between anti–double-stranded DNA antibodies and exacerbation of renal disease in patients with systemic lupus erythematosus. Arthritis & Rheumatism. 2005;52(4):1129–1137. doi:10.1002/art.20980 — trial data linking rising anti-dsDNA to kidney (renal) flares.
- ter Borg EJ, Horst G, Hummel EJ, Limburg PC, Kallenberg CGM. Measurement of increases in anti–double-stranded DNA antibody levels as a predictor of disease exacerbation in systemic lupus erythematosus. Arthritis & Rheumatism. 1990;33(5):634–643. doi:10.1002/art.1780330505 — the classic prospective study showing rising titers can precede flares.
- Yung S, Chan TM. Mechanisms of kidney injury in lupus nephritis — the role of anti-dsDNA antibodies. Frontiers in Immunology. 2015;6:475. doi:10.3389/fimmu.2015.00475 — how anti-dsDNA antibodies actually injure the kidney.
- Enocsson H, Sjöwall C, Wirestam L, et al. Four anti-dsDNA antibody assays in relation to systemic lupus erythematosus disease specificity and activity. The Journal of Rheumatology. 2015;42(5):817–825. doi:10.3899/jrheum.140677 — why the assay method matters: different tests give different specificity and activity correlations.
Connections
- ANA Test (Antinuclear Antibody)
- Complement (C3, C4, CH50)
- Urinalysis
- Microalbumin & ACR (Urine Protein)
- Complete Blood Count (CBC)
- Rheumatoid Factor (RF)
- ANCA Test
- Lupus (SLE)
- ANA, dsDNA, and Lupus Autoantibodies
- Lupus Nephritis and Kidney Involvement
- ACR/EULAR 2019 Classification Criteria for SLE
- All Rheumatology
- Immunology
- All Lab Tests