Anticardiolipin Antibodies
Anticardiolipin antibodies are a blood test that helps doctors understand why someone is forming unexpected blood clots or losing pregnancies. The antibodies themselves are immune proteins that have started, by mistake, to target certain fatty molecules and the proteins attached to them. On their own they can sound alarming, but a single positive result rarely means what people fear it does. This test is really one piece of a careful puzzle used to diagnose antiphospholipid syndrome (APS) — an autoimmune condition that makes the blood more likely to clot. This page explains, in plain language, what the antibodies are, why the test gets ordered, why it almost always has to be repeated before it means anything, and what your result may or may not be telling you. If you are reading this after a frightening event like a clot or a miscarriage, please know that APS is one of the more treatable reasons behind these things — and that a positive test is a starting point for care, not a verdict.
Table of Contents
- What Anticardiolipin Antibodies Are
- Why the Test Is Ordered
- The Antiphospholipid Trio
- Why One Positive Is Not Enough
- How to Read Your Results
- Conditions Linked to These Antibodies
- Antiphospholipid Syndrome and Pregnancy
- Related Tests
- When to Talk to Your Doctor
- Research Papers
- Connections
- Featured Videos
What Anticardiolipin Antibodies Are
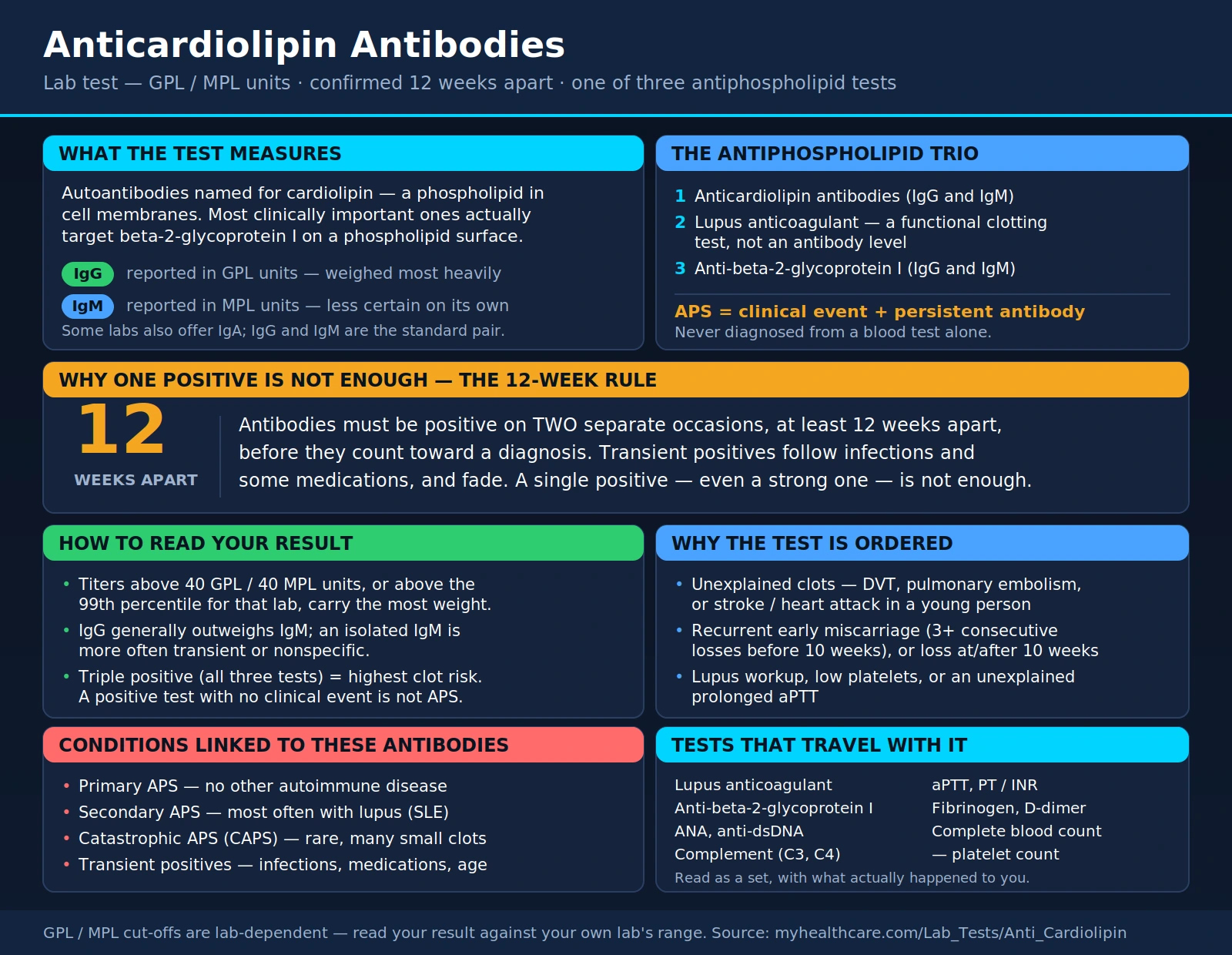
Antibodies are proteins the immune system normally makes to recognize and fight germs. An autoantibody is an antibody that has turned inward and started reacting against the body's own components. Anticardiolipin antibodies are a specific type of autoantibody named after cardiolipin, a phospholipid — that is, a fatty molecule found in the membranes of cells and in the tiny structures inside them that make energy.
Here is a subtlety worth understanding, because it explains a lot about how the test behaves. Despite the name, these antibodies do not usually attack cardiolipin all by itself. Most of the clinically important ones actually recognize phospholipid-binding proteins — especially a blood protein called beta-2-glycoprotein I — when those proteins are sitting on a phospholipid surface. For this reason, anticardiolipin antibodies are grouped into a larger family called antiphospholipid antibodies. When these antibodies coat the surfaces where clotting normally starts and stops, they can tip the balance toward forming clots.
The lab measures anticardiolipin antibodies in two main forms, or "isotypes":
- IgG — the longer-lasting antibody class, and generally the one doctors weigh most heavily.
- IgM — often the first antibody the body makes; on its own it tends to carry less certainty.
Results are reported in named units — GPL units for IgG and MPL units for IgM — along with a reference range from the specific laboratory. (Some labs also offer an IgA version, but IgG and IgM are the standard pair.) The exact numbers matter less than the pattern, which the sections below unpack.
Why the Test Is Ordered
The flagship reason to check anticardiolipin antibodies is a suspicion of antiphospholipid syndrome (APS) — an autoimmune clotting disorder. Unlike an ordinary clotting problem caused by immobility or surgery, APS reflects an underlying tendency, driven by these antibodies, for blood to clot when it should not. Doctors reach for this test when the story does not add up on its own.
Two kinds of events raise the question of APS:
- Unexplained blood clots. A deep vein thrombosis (a clot in a leg vein), a pulmonary embolism (a clot that travels to the lungs), or an arterial clot such as a stroke or heart attack in a young person with few other risk factors. A clot in an unusual location, or clots that keep coming back despite treatment, are also flags.
- Characteristic pregnancy complications. Recurrent early miscarriage (often defined as three or more consecutive losses before 10 weeks), one or more losses of a normally-formed baby at or after 10 weeks, or a premature birth driven by severe preeclampsia or a poorly functioning placenta.
The test is sometimes added for other reasons too — as part of evaluating lupus or another autoimmune disease, when platelets are unexpectedly low, or when a routine clotting test (the aPTT) comes back mysteriously prolonged. In every case, the antibody test is answering a "why" question raised by something that already happened.
The Antiphospholipid Trio
Anticardiolipin is not a solo act. It is one of three laboratory tests used together to identify antiphospholipid syndrome. Understanding the trio makes your results far easier to interpret. The three tests are:
- Anticardiolipin antibodies (IgG and IgM) — the test described on this page.
- Lupus anticoagulant — despite its confusing name, this is not an antibody level at all. It is a functional clotting test that detects antibodies interfering with clotting reactions in the test tube. (The name is a historical accident; it neither means you have lupus nor that your blood is thinner.)
- Anti-beta-2-glycoprotein I antibodies (IgG and IgM) — measuring antibodies against the very protein that most anticardiolipin antibodies really target.
Now the part that matters most. A diagnosis of APS is never made from a blood test alone. By international agreement, it requires both of the following:
- A clinical event — a confirmed blood clot, or one of the defined pregnancy complications; and
- A persistently positive antibody test — at least one of the three tests above, positive and confirmed over time.
A positive antibody with no clinical event is not APS. A clot with no confirmed antibody is not APS. The syndrome lives in the overlap of the two.
Why One Positive Is Not Enough
This is the single most important idea on the page, and the one most likely to spare you unnecessary worry. Antiphospholipid antibodies must be positive on two separate occasions, at least 12 weeks apart, before they count toward a diagnosis. A single positive result — even a strongly positive one — is not enough.
The reason is that these antibodies frequently appear transiently and then disappear. Common triggers for a short-lived positive include:
- Recent infections, which can stir up antiphospholipid antibodies that fade once the illness resolves.
- Certain medications.
- Sometimes no identifiable reason at all — low-level positives turn up in some healthy people, more often with age.
These fleeting antibodies usually do not carry the clotting risk of the persistent kind. That is why the retest is scheduled around 12 weeks (roughly three months) later — long enough to let a temporary blip fade. If the antibody is still there at the second draw, it is far more likely to be the real, meaningful kind. So if you have had one positive result, try to hold off on conclusions until the confirming test is done. A repeat is not a sign that something was missed; it is exactly how the test is designed to be used.
How to Read Your Results
Interpreting anticardiolipin antibodies is less about a single cutoff and more about weighing several features together. A few guiding principles:
- Height matters. Medium-to-high titers are far more meaningful than low ones. Many labs and classification criteria only count values above a defined threshold — commonly above 40 GPL or 40 MPL units, or above the 99th percentile for that laboratory. A result that hovers just above the reference range carries much less weight than one that is clearly elevated.
- IgG generally outweighs IgM. An elevated IgG anticardiolipin is usually taken more seriously than an isolated IgM elevation, which is more prone to being a transient or nonspecific finding.
- A positive test without a clinical event is not APS. It is entirely possible to carry these antibodies and never have a problem. Such a result may warrant awareness and, in some situations, prevention around high-risk times — but by itself it is not a diagnosis and not a reason for lifelong treatment.
- "Triple positive" is the highest-risk pattern. When all three tests — anticardiolipin, lupus anticoagulant, and anti-beta-2-glycoprotein I — are positive together, the risk of clotting is meaningfully higher than with a single positive test. This pattern especially shapes how aggressively doctors recommend prevention and long-term anticoagulation.
Put simply: a persistent, high-titer IgG anticardiolipin in someone who has had a clot or a defined pregnancy loss is a strong finding. A single, low-level IgM in a person who feels well is usually not.
Conditions Linked to These Antibodies
Anticardiolipin antibodies show up in several settings, and the context changes their meaning:
- Primary APS. The syndrome occurs on its own, without another underlying autoimmune disease. Clots or pregnancy losses are the presenting problem.
- Secondary APS. The syndrome accompanies another autoimmune condition — most often systemic lupus erythematosus (SLE). A substantial share of people with lupus carry antiphospholipid antibodies, which is one reason these tests are often checked together.
- Catastrophic APS (CAPS). A rare but grave form in which many small clots develop across several organs over a short period. It is a medical emergency requiring intensive hospital care. CAPS is uncommon, and mentioning it is not meant to frighten — it simply explains why doctors take persistent, high-level antibodies seriously.
- Transient or incidental positives. As noted earlier, infections, some medications, and simply getting older can produce low-level antibodies that carry little or no clotting risk. These are exactly the results that the 12-week retest is designed to sort out.
Antiphospholipid Syndrome and Pregnancy
For many people, this is the most personal part of the story, and it deserves a gentle, honest telling. Recurrent miscarriage and later pregnancy loss are heartbreaking, and they are rarely anyone's fault. Among the many possible causes, APS stands out for an encouraging reason: it is one of the few that is genuinely treatable.
In APS, the antibodies appear to interfere with the placenta — through clotting and through direct effects on the tissues that connect a pregnancy to the mother's blood supply. This can lead to repeated early losses, loss later in pregnancy, or complications such as severe preeclampsia and a placenta that stops supporting the baby well.
The good news is that treatment can meaningfully improve outcomes. The standard approach in a pregnancy affected by APS is low-dose aspirin, usually combined with heparin (typically a low-molecular-weight heparin given by injection). Studies of this combination in women with antiphospholipid antibodies and recurrent loss have shown improved live-birth rates. This is not something to attempt alone — it calls for coordinated care, often shared between an obstetrician and a rheumatologist or hematologist, with monitoring throughout the pregnancy. If you have had recurrent losses and have not been tested, it is a reasonable and important question to raise with your doctor.
Related Tests
Because anticardiolipin antibodies are interpreted alongside other results, it helps to know the tests that usually travel with them:
- Lupus anticoagulant and anti-beta-2-glycoprotein I — the other two members of the antiphospholipid trio, ordered together with anticardiolipin.
- ANA and anti-dsDNA — antibody tests used to look for lupus, which frequently coexists with APS.
- Clotting studies — the aPTT (which the lupus anticoagulant can prolong), PT/INR, fibrinogen, and D-dimer, used to evaluate clotting and to monitor treatment.
- Complete blood count — especially the platelet count, since APS can be associated with a low platelet count.
- Complement (C3, C4) — sometimes checked when lupus is part of the picture.
No single one of these makes or breaks a diagnosis. Doctors read them as a set, together with what actually happened to you.
When to Talk to Your Doctor
Reach out to a clinician if any of the following apply, and bring your questions with you:
- You have had an unexplained blood clot, particularly at a young age, in an unusual place, or one that keeps recurring.
- You have experienced recurrent miscarriage or a late pregnancy loss, or a pregnancy complicated by severe preeclampsia or placental failure.
- You have received a positive anticardiolipin result. If so, the most useful next steps are usually a confirming test after about 12 weeks and a conversation about whether a clinical event was ever present. Try not to let a single number alarm you before that fuller picture is in.
- You already carry a diagnosis of lupus or another autoimmune disease and want to understand your clotting risk.
One practical caution: never start or stop a blood thinner on your own based on a lab result. Anticoagulation decisions in APS are individualized, and they depend on the whole story — the antibody pattern, whether you have clotted, and your other risks. Your doctor is the right partner for those choices. This page is here to help you walk into that conversation informed, not to replace it.
Research Papers
- Miyakis S, Lockshin MD, Atsumi T, Branch DW, et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). Journal of Thrombosis and Haemostasis. 2006;4(2):295–306. doi:10.1111/j.1538-7836.2006.01753.x — the revised Sydney criteria that set the "clinical event plus persistent antibody, confirmed 12 weeks apart" framework.
- Garcia D, Erkan D. Diagnosis and Management of the Antiphospholipid Syndrome. New England Journal of Medicine. 2018;378(21):2010–2021. doi:10.1056/NEJMra1705454 — a clear clinical review of how APS is recognized and treated.
- Wilson WA, Gharavi AE, Koike T, Lockshin MD, et al. International consensus statement on preliminary classification criteria for definite antiphospholipid syndrome: report of an international workshop. Arthritis & Rheumatism. 1999;42(7):1309–1311. doi:10.1002/1529-0131(199907)42:7<1309::AID-ANR1>3.0.CO;2-F — the original Sapporo criteria that first standardized the diagnosis.
- Barbhaiya M, Zuily S, Naden R, Hendry A, et al. 2023 ACR/EULAR antiphospholipid syndrome classification criteria. Annals of the Rheumatic Diseases. 2023;82(10):1258–1270. doi:10.1136/ard-2023-224609 — the newest, weighted classification system for APS.
- Cervera R, Piette JC, Font J, Khamashta MA, et al. Antiphospholipid syndrome: clinical and immunologic manifestations and patterns of disease expression in a cohort of 1,000 patients. Arthritis & Rheumatism. 2002;46(4):1019–1027. doi:10.1002/art.10187 — the Euro-Phospholipid cohort describing how APS actually presents in real patients.
- Pengo V, Ruffatti A, Legnani C, Gresele P, et al. Clinical course of high-risk patients diagnosed with antiphospholipid syndrome. Journal of Thrombosis and Haemostasis. 2010;8(2):237–242. doi:10.1111/j.1538-7836.2009.03674.x — evidence that "triple positive" patients carry the highest clotting risk.
- Galli M, Luciani D, Bertolini G, Barbui T. Anti-beta-2-glycoprotein I, antiprothrombin antibodies, and the risk of thrombosis in the antiphospholipid syndrome. Blood. 2003;102(8):2717–2723. doi:10.1182/blood-2002-11-3334 — how the specificity of the antibody relates to clotting risk.
- Devreese KMJ, de Groot PG, de Laat B, Erkan D, et al. Guidance from the Scientific and Standardization Committee for lupus anticoagulant/antiphospholipid antibodies of the ISTH. Journal of Thrombosis and Haemostasis. 2020;18(11):2828–2839. doi:10.1111/jth.15047 — laboratory guidance on titer thresholds and test timing.
- Tektonidou MG, Andreoli L, Limper M, Amoura Z, et al. EULAR recommendations for the management of antiphospholipid syndrome in adults. Annals of the Rheumatic Diseases. 2019;78(10):1296–1304. doi:10.1136/annrheumdis-2019-215213 — guideline recommendations on prevention, anticoagulation, and pregnancy.
- Schreiber K, Sciascia S, de Groot PG, Devreese K, et al. Antiphospholipid syndrome. Nature Reviews Disease Primers. 2018;4:17103. doi:10.1038/nrdp.2017.103 — a comprehensive primer covering mechanisms, testing, and treatment.
- Rai R, Cohen H, Dave M, Regan L. Randomised controlled trial of aspirin and aspirin plus heparin in pregnant women with recurrent miscarriage associated with phospholipid antibodies (or antiphospholipid antibodies). BMJ. 1997;314(7076):253–257. doi:10.1136/bmj.314.7076.253 — a foundational trial of aspirin plus heparin for obstetric APS.
- Empson M, Lassere M, Craig JC, Scott JR. Prevention of recurrent miscarriage for women with antiphospholipid antibody or lupus anticoagulant. Cochrane Database of Systematic Reviews. 2005;(2):CD002859. doi:10.1002/14651858.CD002859.pub2 — a systematic review weighing treatments to prevent recurrent pregnancy loss in APS.
Connections
- Coagulation Panel
- aPTT (Lupus Anticoagulant Screen)
- D-Dimer
- Prothrombin Time (PT/INR)
- ANA Test
- Anti-dsDNA
- Complement (C3/C4)
- Lupus (SLE)
- Rheumatology
- Reproductive Medicine
- Deep Vein Thrombosis
- Stroke
- All Lab Tests