Albumin Test: Serum Albumin — Nutrition, Liver Function, and Critical Illness Marker
Serum albumin is the most abundant protein in human blood plasma, produced exclusively by the liver at a rate of 10–15 grams per day in healthy adults. It performs three irreplaceable functions: maintaining oncotic pressure (the force that keeps fluid in blood vessels), transporting a remarkable variety of molecules through the bloodstream (hormones, fatty acids, bilirubin, calcium, zinc, and dozens of drugs), and acting as a circulating buffer against oxidative stress. Because albumin synthesis requires a functioning liver, adequate protein nutrition, and absence of severe systemic inflammation, serum albumin is a direct readout of multiple intersecting physiological processes at once. Clinicians use it to assess nutritional status, gauge hepatic synthetic function, track the severity of critical illness, and interpret other lab values (especially calcium and drug levels) that are albumin-bound.
Table of Contents
- What Albumin Measures
- Albumin Synthesis and Physiology
- Reference Ranges
- Causes of Low Albumin (Hypoalbuminemia)
- Albumin and Liver Disease
- Albumin and Nutritional Assessment
- Critical Illness and the Acute-Phase Response
- Drug and Calcium Correction with Albumin
- Research References
- Featured Videos
What Albumin Measures
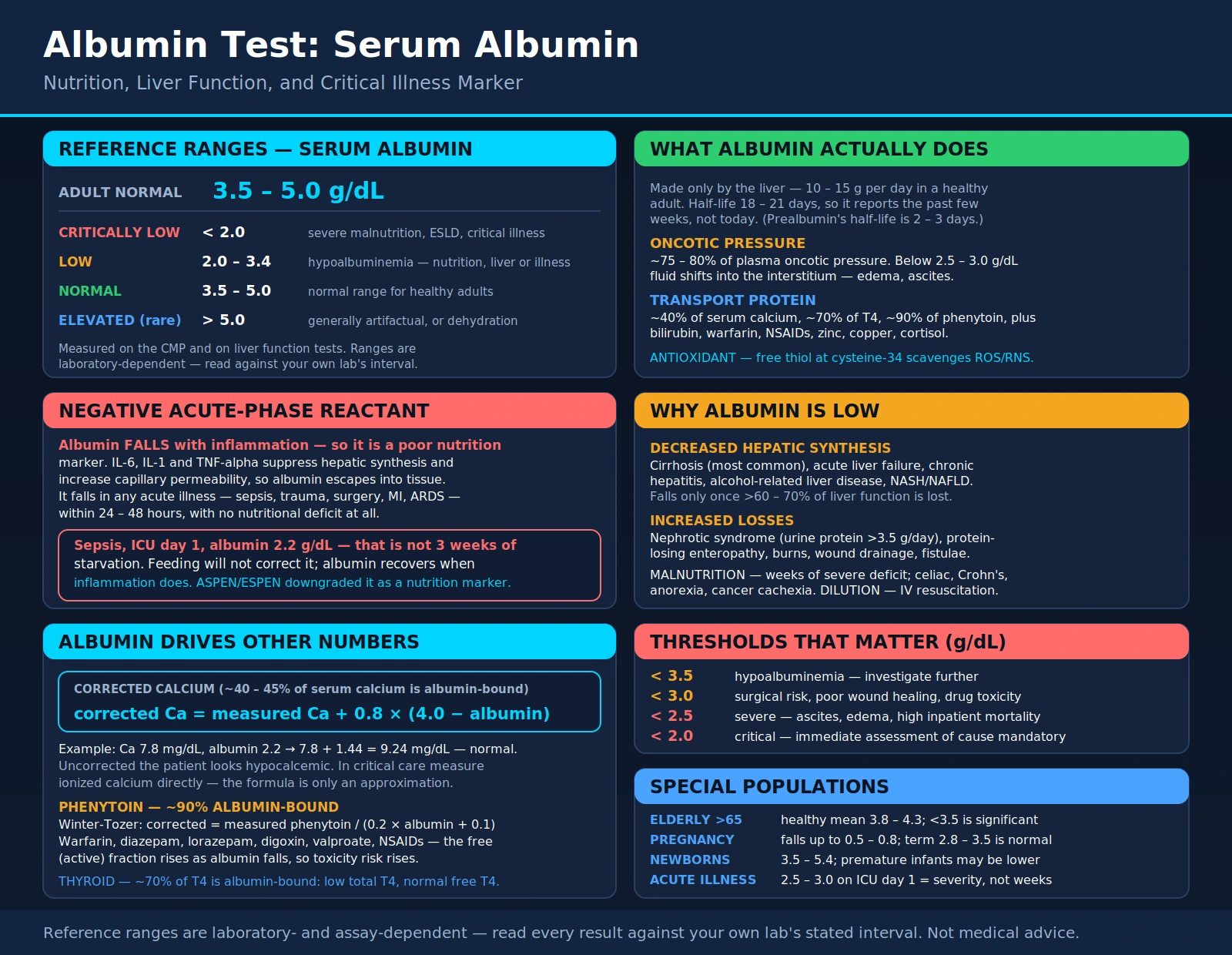
Serum albumin is measured as part of the Comprehensive Metabolic Panel (CMP) and Liver Function Tests (LFTs). A single value of 3.5–5.0 g/dL is reported as normal for adults, but this number carries layered meaning. Because albumin has a long half-life in plasma (approximately 18–21 days), the serum albumin level reflects average protein synthesis and loss over the previous several weeks — not just today. This makes it a reliable medium-term nutritional and hepatic indicator, but a slow-to-respond acute-phase marker.
Contrast this with prealbumin (transthyretin), which has a half-life of just 2–3 days and responds more acutely to changes in nutritional status and inflammation. Together, albumin and prealbumin provide complementary views: albumin tells you about chronic nutritional status and liver reserve; prealbumin (when available) tracks acute changes.
The three primary reasons clinicians check albumin are: (1) to assess hepatic synthetic function (is the liver making enough protein?), (2) to evaluate nutritional status (is the patient getting and absorbing adequate protein?), and (3) as a general severity marker in chronic and acute illness, since albumin falls predictably as inflammation, critical illness, or organ failure worsens.
Albumin Synthesis and Physiology
Albumin is synthesized by hepatocytes (liver parenchymal cells), processed through the endoplasmic reticulum and Golgi apparatus, and secreted directly into the sinusoids. The liver preferentially maintains albumin synthesis over other hepatic protein production; only when more than 60–70% of liver function is lost does serum albumin begin to fall significantly in pure liver disease — meaning a low albumin from liver disease represents far-advanced dysfunction.
The primary physiological roles of albumin:
Oncotic Pressure Maintenance: Albumin accounts for approximately 75–80% of plasma oncotic pressure — the colloid osmotic pressure that opposes the outward filtration of water from capillaries. When albumin falls below 2.5–3.0 g/dL, oncotic pressure drops and fluid shifts out of the vascular space into the interstitium, causing edema (ankle swelling, ascites in liver disease, pulmonary edema in severe hypoalbuminemia).
Transport Protein: Albumin has multiple binding sites for diverse molecules: bilirubin (bound tightly; displaceability by certain drugs causes jaundice), long-chain fatty acids, calcium (approximately 40% of serum calcium is albumin-bound), zinc, copper, thyroxine (T4), cortisol, drugs (warfarin, NSAIDs, phenytoin, digitalis, sulfonamides — critical for pharmacokinetics). When albumin is low, free (unbound) fractions of these substances increase, altering their activity and toxicity.
Antioxidant: The cysteine residue at position 34 of albumin carries a free thiol group that directly scavenges reactive oxygen species and reactive nitrogen species. In critical illness, albumin is progressively oxidized, losing this antioxidant capacity — contributing to oxidative organ injury.
Distribution Volume: Because albumin is largely confined to the intravascular space (and lymphatics), its concentration reflects the balance between hepatic synthesis rate, vascular escape (transcapillary leakage), degradation (~10% per day), and urinary loss.
Reference Ranges
Normal: 3.5–5.0 g/dL (adults)
| Range | Value (g/dL) | Clinical Significance |
|---|---|---|
| Critically Low | <2.0 | CRITICAL — severe malnutrition, end-stage liver disease, critical illness; immediate assessment mandatory |
| Low | 2.0–3.4 | Hypoalbuminemia; significant nutritional deficit, liver disease, or systemic illness |
| Normal | 3.5–5.0 | Normal range for healthy adults |
| Elevated (rare) | >5.0 | Generally artifactual or due to dehydration/hemoconcentration |
Special Populations and Notes
- Elderly (>65): Mean albumin in healthy elderly is 3.8–4.3 g/dL — slightly lower than younger adults; values <3.5 in elderly are clinically significant.
- Pregnancy: Albumin falls progressively by up to 0.5–0.8 g/dL due to hemodilution; term albumin of 2.8–3.5 g/dL is not uncommon and does not indicate liver disease.
- Newborns: Higher at 3.5–5.4 g/dL; premature infants may be lower due to immature hepatic synthesis.
- Acute illness: Albumin drops rapidly in the first 24–48 hours of critical illness due to transcapillary leakage and redistribution — not due to decreased synthesis or nutrition. A value of 2.5–3.0 g/dL on ICU admission day 1 reflects illness severity, not weeks of malnutrition.
Thresholds That Matter Clinically
- <3.5 g/dL: Hypoalbuminemia — investigate further
- <3.0 g/dL: Moderate-severe — associated with increased surgical risk, poor wound healing, drug toxicity risk
- <2.5 g/dL: Severe — ascites, edema, high mortality risk in hospitalized patients
- <2.0 g/dL: Critical — immediate assessment of cause mandatory
Causes of Low Albumin (Hypoalbuminemia)
Decreased Hepatic Synthesis
Cirrhosis (most common cause of chronic hypoalbuminemia in clinical practice); acute liver failure; chronic active hepatitis; alcohol-related liver disease; non-alcoholic steatohepatitis (NASH/NAFLD) with advanced fibrosis. In well-compensated cirrhosis, albumin may be normal; hypoalbuminemia signals decompensation (Child-Pugh class B or C scoring uses albumin directly).
Protein Malnutrition and Malabsorption
Severe dietary protein restriction; anorexia nervosa; prolonged NPO status; malabsorption syndromes (celiac disease, Crohn's disease, short bowel syndrome); cancer cachexia. Requires weeks of severe deficit to produce hypoalbuminemia due to the long half-life.
Increased Losses
Protein-losing enteropathy (PLE): Disorders causing excessive albumin leakage into the GI tract — lymphangiectasia, inflammatory bowel disease, Ménétrier's disease. Alpha-1-antitrypsin fecal test used to diagnose PLE.
Nephrotic syndrome: Massive urinary protein loss (>3.5 g/day); albumin is lost in the urine faster than the liver can synthesize it. Characteristic triad: hypoalbuminemia + edema + hyperlipidemia.
Burns: Massive transcapillary fluid and protein loss from burned skin surface area proportional to burn extent.
Wound drainage: Large surgical wounds, fistulae.
Inflammation and the Acute-Phase Response
IL-6, IL-1, and TNF-alpha suppress hepatic albumin synthesis and increase vascular permeability (promoting albumin escape into tissues). This is why albumin falls in any acute illness — sepsis, trauma, surgery, myocardial infarction, ARDS — within 24–48 hours even without nutritional deficit. Albumin is a negative acute-phase reactant.
Dilutional
Aggressive IV fluid resuscitation (normal saline or lactated Ringer's) dilutes plasma proteins. A post-resuscitation albumin of 2.5–3.0 g/dL in a patient who was 3.8 pre-illness represents dilution, not worsening liver function.
Albumin and Liver Disease
Albumin is one of the most important markers of hepatic synthetic function and is directly incorporated into clinical scoring systems:
Child-Pugh Score
Uses albumin as one of 5 variables: albumin >3.5 g/dL = 1 point; 2.8–3.5 = 2 points; <2.8 = 3 points. Child-Pugh A (compensated) = 5–6 points; B (moderate) = 7–9; C (decompensated) = 10–15. Low albumin is the most predictive of the hepatic synthetic variables in determining cirrhosis stage and prognosis.
MELD and MELD-Na Score
The MELD score (used to prioritize liver transplant listing) does not include albumin directly. However, MELD-Na and CLIF-C scores used in acute-on-chronic liver failure (ACLF) do incorporate albumin. Low albumin <3.0 g/dL on presentation with ACLF predicts 90-day mortality exceeding 50%.
Distinguishing Hepatocellular from Cholestatic Disease
In cholestatic disease (primary biliary cholangitis, primary sclerosing cholangitis, bile duct obstruction), bilirubin and ALP rise prominently, but albumin may be preserved until late. In hepatocellular disease (cirrhosis, hepatitis), albumin falls earlier because hepatocytes are directly dysfunctional.
Ascites and the SAAG
Hypoalbuminemia reduces oncotic pressure, compounding the portal hypertensive driving force that produces ascites. The SAAG (Serum-Ascites Albumin Gradient) = serum albumin minus ascitic fluid albumin. SAAG ≥1.1 g/dL indicates portal hypertensive cause; SAAG <1.1 indicates non-portal hypertensive cause (malignancy, peritoneal infection, pancreatitis).
Liver Transplant Monitoring
Serial albumin post-transplant tracks graft synthetic function recovery. Rising albumin over the first 2 weeks after transplant is a reliable sign of primary graft function; persistently low albumin raises concern for primary non-function or early rejection.
Albumin and Nutritional Assessment
Albumin has a complex relationship with nutrition. While it was historically used as the primary nutritional marker, modern nutritional guidelines (ASPEN, ESPEN) have downgraded its role as an acute nutritional indicator because: (1) it changes slowly (half-life 18–21 days), (2) it is profoundly suppressed by inflammation regardless of nutritional intake, and (3) short-term nutritional interventions do not rapidly correct albumin.
However, albumin remains clinically valuable in nutritional assessment when interpreted correctly:
Chronic Malnutrition Detection
In a non-acutely-ill outpatient, albumin <3.5 g/dL — especially when combined with below-normal prealbumin, BMI, and muscle mass — does identify chronic protein-energy malnutrition. This context is appropriate for chronic alcoholism, eating disorders, cancer surveillance, and post-bariatric surgery follow-up.
Pre-Operative Nutritional Risk
Albumin <3.0 g/dL before major surgery (especially GI, cardiac, orthopedic) predicts significantly higher complication rates, longer length of stay, and surgical site infection. Pre-operative nutritional optimization targeting albumin >3.5 g/dL reduces these risks and is formally recommended in enhanced recovery after surgery (ERAS) protocols.
Wound Healing
Albumin is required for fibroblast function, collagen synthesis, and immune cell activity in wound healing. Albumin below 3.0 g/dL predicts poor wound healing, pressure ulcer development, and anastomotic leak after bowel surgery.
Distinguishing Inflammation from Malnutrition
The inflammatory marker CRP (or hs-CRP) measured alongside albumin allows interpretation: albumin low + CRP high = inflammation-driven (acutely ill or chronically inflamed); albumin low + CRP normal/low = true nutritional deficit. This distinction guides whether to prioritize anti-inflammatory treatment versus nutritional replacement.
Prealbumin/transthyretin (normal range 15–36 mg/dL; <11 mg/dL = severely deficient, half-life 2–3 days) tracks acute nutritional recovery better than albumin and should be used in ICU and acute settings where rapid nutritional response assessment is needed.
Critical Illness and the Acute-Phase Response
In the ICU, virtually every critically ill patient has hypoalbuminemia. This is NOT primarily a nutritional problem in the acute phase — it reflects the acute-phase inflammatory response:
Mechanism
Cytokines (IL-6, IL-1β, TNF-α) released during systemic inflammation directly suppress hepatic albumin synthesis AND increase capillary permeability, causing albumin to shift from the intravascular space into the interstitium. Third-spacing of albumin into extravascular compartments is demonstrable by isotope-labeled albumin studies. Simultaneously, catabolism increases and degradation accelerates.
Clinical Implication
A patient admitted to the ICU with sepsis who has albumin of 2.2 g/dL on day 1 does not have 3 weeks of malnutrition — they have acute systemic inflammation. Providing enteral nutrition will not rapidly correct the albumin. The albumin recovers when the inflammatory driver resolves.
IV Albumin Infusion — Evidence-Based Indications
IV albumin is used in specific clinical contexts (NOT routine nutrition replacement):
- Large-volume paracentesis (>5L of ascites drained): Give 8 g albumin per liter of ascites removed to prevent post-paracentesis circulatory dysfunction.
- Spontaneous bacterial peritonitis (SBP): Albumin infusion (1.5 g/kg at diagnosis, 1 g/kg on day 3) reduces hepatorenal syndrome and in-hospital mortality — a landmark RCT finding (Sort et al., NEJM 1999).
- Hepatorenal syndrome (HRS): Albumin + terlipressin or norepinephrine is guideline-recommended therapy for HRS-AKI.
- NOT indicated: Routine ICU hypoalbuminemia without one of the above indications; meta-analyses show no mortality benefit and potential harm from routine albumin infusion in general critical illness.
Prognostic Value in Critical Illness
Albumin <2.5 g/dL in the ICU setting predicts higher 30-day mortality across multiple disease categories. Serial albumin that fails to recover over ICU days 1–5 despite treatment identifies patients with the most severe illness burden and guides goals-of-care discussions.
Drug and Calcium Correction with Albumin
Two laboratory corrections are essential knowledge for anyone interpreting lab panels alongside albumin:
Corrected Calcium Formula
Approximately 40–45% of serum calcium is albumin-bound. When albumin is low, measured total calcium is artifactually low. The corrected calcium formula adjusts for this:
Corrected Ca (mg/dL) = Measured Ca + 0.8 × (4.0 − measured albumin)
Example: Patient with measured Ca 7.8 mg/dL and albumin 2.2 g/dL: Corrected Ca = 7.8 + 0.8 × (4.0 − 2.2) = 7.8 + 1.44 = 9.24 mg/dL — normal. Without this correction, the patient appears hypocalcemic but ionized calcium is normal. For critical care, always measure ionized calcium directly (via blood gas analyzer) — the formula is a useful approximation but not a substitute for direct measurement.
Drug Levels and Albumin
Many drugs are highly albumin-bound. In hypoalbuminemia, free (active) drug fractions increase even when total measured drug levels appear therapeutic, creating toxicity risk:
- Phenytoin: Approximately 90% albumin-bound. In hypoalbuminemia or renal failure, free (active) phenytoin is increased even when total phenytoin appears therapeutic. Use the Winter-Tozer equation: Corrected phenytoin = measured phenytoin / (0.2 × albumin + 0.1) to avoid phenytoin toxicity.
- Warfarin: Highly albumin-bound; interactions with drugs that displace warfarin from albumin binding sites cause sudden INR elevation.
- Diazepam, lorazepam, digoxin, valproate, NSAIDs: All significantly albumin-bound; toxicity risk increases in hypoalbuminemia.
Thyroid hormones: Approximately 70% of T4 is albumin-bound. Low albumin can cause low total T4 with normal free T4 — a common source of diagnostic confusion (not hypothyroidism). Always check free T4, not total T4, when albumin is low.
Research References
- Doumas BT, Watson WA, Biggs HG. Albumin standards and the measurement of serum albumin with bromcresol green. Clin Chim Acta. 1971;31(1):87-96. PMID: 5544879 — Search PubMed
- Pugh RN, Murray-Lyon IM, Dawson JL, Pietroni MC, Williams R. Transection of the oesophagus for bleeding oesophageal varices. Br J Surg. 1973;60(8):646-649. PMID: 4541913 — PubMed
- Soeters PB, Wolfe RR, Shenkin A. Hypoalbuminemia: Pathogenesis and clinical significance. JPEN J Parenter Enteral Nutr. 2019;43(2):181-193. PMID: 30288770 — Search PubMed
- Soeters PB, Schols AM. Advances in understanding and assessing malnutrition. Curr Opin Clin Nutr Metab Care. 2009;12(5):487-494. PMID: 19623053 — Search PubMed
- Vincent JL, Dubois MJ, Navickis RJ, Wilkes MM. Hypoalbuminemia in acute illness: Is there a rationale for intervention? A meta-analysis of cohort studies and controlled trials. Ann Surg. 2003;237(3):319-334. PMID: 12616115 — PubMed
- Kamath PS, Wiesner RH, Malinchoc M, et al. A model to predict survival in patients with end-stage liver disease. Hepatology. 2001;33(2):464-470. PMID: 11172350 — PubMed
- Bernstein LH, Leukhardt-Fairfield CJ, Pleban W, Rudolph R. Usefulness of data on albumin and prealbumin concentrations in determining effectiveness of nutritional support. Clin Chem. 1989;35(2):271-274. PMID: 2914157 — Search PubMed
- Nicholson JP, Wolmarans MR, Park GR. The role of albumin in critical illness. Br J Anaesth. 2000;85(4):599-610. PMID: 11064620 — PubMed
- Runyon BA; AASLD Practice Guideline Committee. Management of adult patients with ascites due to cirrhosis: Update 2012. Hepatology. 2013;57(4):1651-1653. PMID: 23463403 — PubMed
- Gupta D, Lis CG. Pretreatment serum albumin as a predictor of cancer survival: A systematic review of the epidemiological literature. Nutr J. 2010;9:69. PMID: 21176212 — Search PubMed
- Kaysen GA, Rathore V, Shearer GC, Depner TA. Mechanisms of hypoalbuminemia in hemodialysis patients. Kidney Int. 1995;48(2):510-516. PMID: 7564126 — Search PubMed
- Arques S. Human serum albumin in cardiovascular diseases. Eur J Intern Med. 2018;52:8-12. PMID: 29908859 — Search PubMed
PubMed: serum albumin clinical significance
Connections
- All Lab Tests
- Comprehensive Metabolic Panel
- Liver Function Tests
- Kidney Function Tests
- Inflammatory Markers
- Ferritin Test
- High-Sensitivity CRP
- Procalcitonin Test
- Calcium Test
- Homocysteine
- NAFLD
- Cirrhosis
- Chronic Kidney Disease
- Nephrotic Syndrome
- Crohn's Disease
- Celiac Disease
- Beef — dietary protein
- Lysine