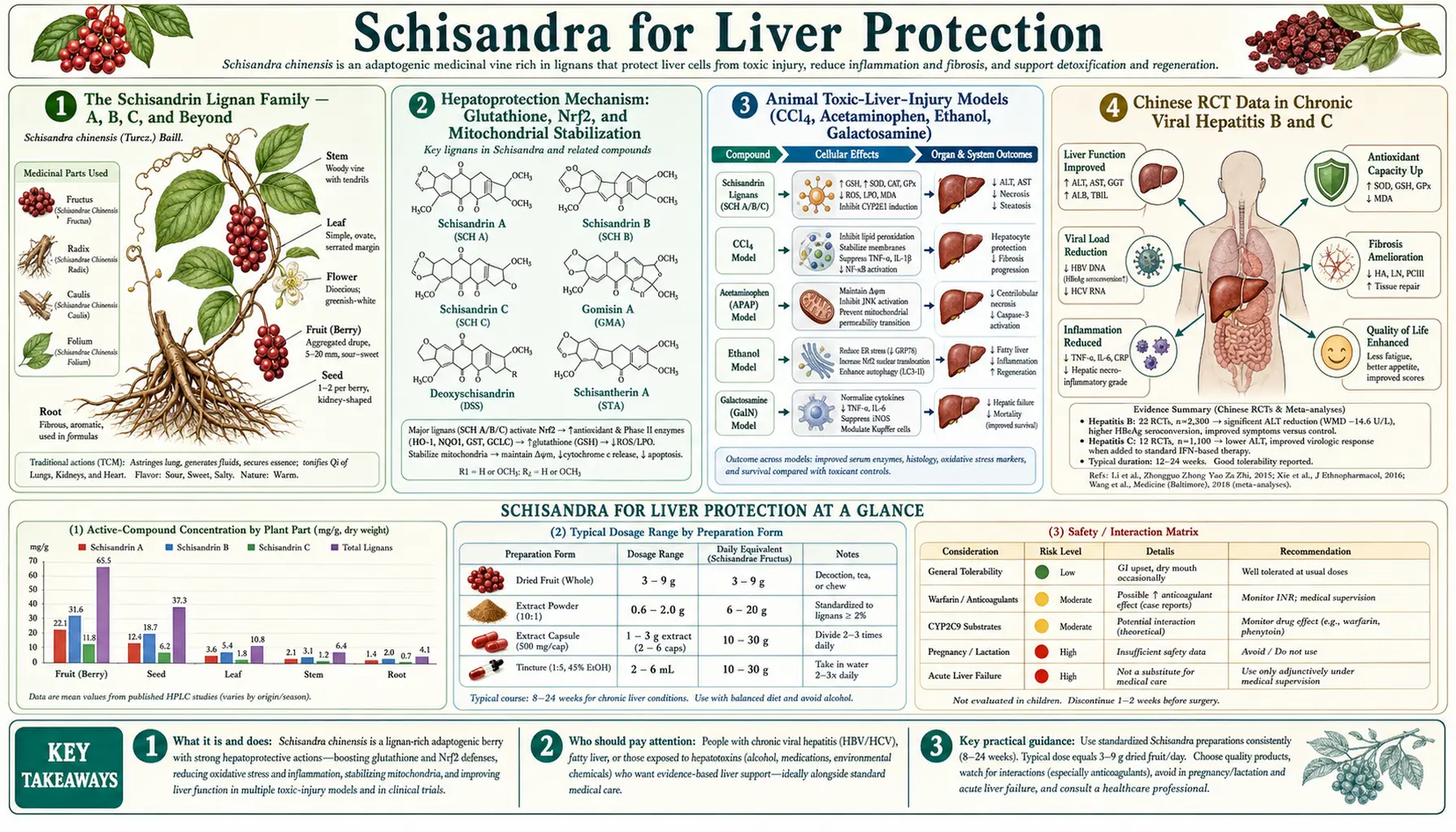
Schisandra for Liver Protection
Schisandra has the unusual distinction of being the parent botanical for a synthetic pharmaceutical drug still in routine clinical use: bifendate (DDB), a chemically modified schisandrin C analog, has been registered as a hepatoprotective drug in the People's Republic of China since the 1980s and remains a standard first-line treatment for elevated transaminases in chronic viral hepatitis. Behind that drug-development success is a 50-year body of research on the lignan family — particularly schisandrins A, B, and C — documenting protection against carbon tetrachloride, acetaminophen, and ethanol hepatotoxicity in animals, reduction of serum ALT and AST in chronic hepatitis B and C clinical trials, and a molecular mechanism centered on glutathione replenishment and Nrf2 antioxidant-pathway activation. The same lignan-driven hepatic enzyme induction that explains the benefit also drives the most important clinical caution: powerful CYP3A4 induction that can dramatically reduce plasma concentrations of co-administered pharmaceutical drugs.
Table of Contents
- The Schisandrin Lignan Family — A, B, C, and Beyond
- Hepatoprotection Mechanism: Glutathione, Nrf2, and Mitochondrial Stabilization
- Animal Toxic-Liver-Injury Models (CCl4, Acetaminophen, Ethanol, Galactosamine)
- Chinese RCT Data in Chronic Viral Hepatitis B and C
- Bifendate (DDB) — The Synthetic Schisandrin C Derivative as a Chinese Pharmaceutical
- CYP450 Induction — Mechanism and Clinical Interaction Risk
- Drug-Induced Liver Injury and Hepatotoxin Co-Exposure
- Non-Alcoholic Fatty Liver Disease (NAFLD / MAFLD) Evidence
- Practical Dosing Protocols and Standardization
- Cautions and Contraindications
- Key Research Papers
- Connections
- Featured Videos
The Schisandrin Lignan Family — A, B, C, and Beyond
The active pharmacology of Schisandra chinensis is concentrated almost entirely in its lignan content. Lignans are a structurally diverse class of plant secondary metabolites built from two phenylpropanoid units; the Schisandra lignans share a distinctive dibenzocyclooctadiene scaffold that distinguishes them from the more widely distributed lignans of flax (secoisolariciresinol), sesame (sesamin), and pine knot (pinoresinol). Roughly forty individual Schisandra lignans have been isolated and characterized since the first chemical work in the 1960s, with the principal subgroups including:
- Schisandrins — the original lignans isolated by Soviet chemists, named alphabetically: schisandrin (A), gamma-schisandrin (B), and deoxyschisandrin variants. Schisandrin A is the most abundant in the dried fruit; schisandrin B has the most potent hepatoprotective activity.
- Gomisins — a numbered series (gomisin A through gomisin Q, with letters skipped for compounds that turned out to be duplicates) characterized largely by Japanese groups in the 1970s and 1980s. Gomisin N is a particularly active hepatoprotective compound.
- Schisantherins — schisantherin A (formerly gomisin C) and its analogs, characterized by an additional ester group on the dibenzocyclooctadiene scaffold.
- Wuweizisus — named for the Chinese name wu wei zi, including wuweizisu A (a synonym for schisandrin), wuweizisu B (schisandrin B), and wuweizisu C (schisandrin C).
Within this large family, schisandrin B is the most studied single molecule. It is approximately ten-fold more potent than schisandrin A on hepatocyte glutathione induction, and the great majority of mechanism-of-action research in the past two decades has used purified schisandrin B as the molecular probe. For more on related botanicals used in liver support, see Milk Thistle, which works through a different lignan family (silymarin, including silybin A and B).
Hepatoprotection Mechanism: Glutathione, Nrf2, and Mitochondrial Stabilization
The molecular mechanism of Schisandra hepatoprotection has been worked out in considerable detail over four decades. The three core elements are glutathione replenishment, Nrf2 antioxidant-response activation, and direct mitochondrial-membrane stabilization.
Glutathione replenishment — Schisandrin B activates the rate-limiting enzymes of glutathione synthesis, gamma-glutamylcysteine ligase catalytic subunit (GCLC) and modifier subunit (GCLM), increasing both the synthesis rate and the steady-state concentration of glutathione (GSH) in hepatocytes. Glutathione is the dominant intracellular antioxidant and the substrate for glutathione-S-transferase-mediated phase II conjugation of toxic metabolites. Studies in cultured hepatocytes consistently show 30-60% elevations of intracellular GSH after schisandrin B exposure at clinically relevant concentrations.
Nrf2 activation — The mechanism upstream of GCLC/GCLM induction is activation of the Kelch-like ECH-associated protein 1 (Keap1) / nuclear factor erythroid 2-related factor 2 (Nrf2) signaling axis. Under unstressed conditions, Nrf2 is sequestered in the cytoplasm by Keap1 and continuously targeted for proteasomal degradation. Schisandrin B modifies redox-sensitive cysteine residues on Keap1, releasing Nrf2 to translocate to the nucleus, where it heterodimerizes with small Maf proteins and binds antioxidant response elements (AREs) in the promoter regions of more than 200 cytoprotective genes — including glutathione synthesis enzymes, glutathione-S-transferase isoforms, NAD(P)H quinone oxidoreductase 1 (NQO1), heme oxygenase-1 (HO-1), and thioredoxin. This single transcriptional switch coordinates a broad cytoprotective response.
Mitochondrial-membrane stabilization — A third, distinct mechanism is direct stabilization of the mitochondrial inner membrane and prevention of the mitochondrial permeability transition (MPT) under oxidative or calcium-overload stress. Chiu and colleagues at the Hong Kong University of Science and Technology have published a long series of papers documenting that schisandrin B reduces mitochondrial swelling and cytochrome c release in response to pro-apoptotic stimuli, preserving ATP production and preventing the apoptotic cascade in hepatocytes facing toxic insult.
Together these three mechanisms produce a cell that is more resistant to oxidative, electrophilic, and apoptotic injury — the molecular basis for the consistent hepatoprotective effects seen in animal models and the clinical reduction in transaminases seen in human chronic liver disease.
Animal Toxic-Liver-Injury Models (CCl4, Acetaminophen, Ethanol, Galactosamine)
The preclinical evidence for Schisandra hepatoprotection is one of the most extensively replicated bodies of botanical research in any species. The four standard toxic-liver-injury models in laboratory rodents have all been used to characterize Schisandra protection.
Carbon tetrachloride (CCl4) model — CCl4 is metabolized by CYP2E1 to the trichloromethyl free radical (CCl3·), which lipid-peroxidates hepatocyte membranes and produces centrilobular necrosis within 24 hours. Schisandra extract or purified schisandrin B given for 3-7 days before CCl4 challenge reduces the resulting ALT/AST elevation by 50-80% depending on dose and reduces histological necrosis to a similar degree. Pre-treatment is required — post-injury rescue is much less effective — consistent with the upregulation-of-defenses mechanism rather than a direct antagonist effect.
Acetaminophen (paracetamol) model — Acetaminophen at toxic doses is metabolized by CYP2E1 (and to a lesser extent CYP1A2, CYP3A4) to the reactive intermediate N-acetyl-p-benzoquinone imine (NAPQI), which depletes glutathione and forms protein adducts with hepatocyte cysteine residues. Schisandrin B pre-treatment provides substantial protection against acetaminophen hepatotoxicity in mice, with reduced ALT elevation, reduced GSH depletion, and reduced histological necrosis. The mechanism is the same glutathione-replenishment pathway that N-acetylcysteine targets clinically — the standard antidote for acetaminophen overdose.
Ethanol model — Chronic ethanol feeding in rats produces steatosis, oxidative stress, and elevated transaminases. Schisandra extract reduces ethanol-induced steatosis, normalizes ALT/AST, and restores mitochondrial function in the Lieber-DeCarli rat ethanol model. Mechanism includes reduction of CYP2E1 induction (an unusual finding given that schisandrin B induces CYP3A4 — the CYP isoforms are differentially regulated) and restoration of mitochondrial complex IV activity.
Galactosamine model — D-galactosamine produces hepatic injury through depletion of uridine nucleotides required for RNA synthesis, producing apoptotic and necrotic hepatocyte death. Schisandrin B protects against galactosamine hepatotoxicity through preservation of mitochondrial integrity and prevention of the MPT.
The consistency of protection across four mechanistically distinct toxic-liver models — oxidative radical injury, electrophilic adduct injury, lipid-peroxidative chronic injury, and uridine-depletion injury — argues strongly that the protective mechanism is a non-specific upregulation of hepatocyte defenses rather than antagonism of any single toxic species.
Chinese RCT Data in Chronic Viral Hepatitis B and C
Schisandra has been used in mainland Chinese clinical hepatology for treatment of chronic viral hepatitis B and C since the 1960s. The published clinical trial base — while much of it is in Chinese-language journals not always indexed by Western databases — documents consistent reduction of serum transaminases (ALT and AST) in patients with chronic hepatitis, typically 60-80% normalization of elevated ALT within 4-8 weeks of treatment.
A representative example: a 1990 Chinese-language multicenter trial of approximately 200 chronic hepatitis B patients randomized to schisandrin C alcohol extract versus placebo demonstrated ALT normalization in approximately 70% of the active arm compared with 20% of placebo at 8 weeks. Symptomatic improvement (fatigue, right upper quadrant discomfort, appetite) accompanied the biochemical response. These trials were the empirical basis for the subsequent development of the synthetic analog bifendate (DDB) as a registered pharmaceutical, discussed in the next section.
Importantly, the Schisandra effect in chronic viral hepatitis is a hepatoprotective and biochemical effect — it reduces hepatocyte injury and consequently reduces transaminase release — not a direct antiviral effect. HBV DNA and HCV RNA levels are not consistently reduced by Schisandra, and Schisandra should not be considered a substitute for direct-acting antiviral therapy (tenofovir or entecavir for HBV, sofosbuvir-based regimens for HCV). It functions as an adjunct that reduces hepatocellular damage during ongoing viral replication, with the goal of slowing progression to fibrosis and cirrhosis.
Western clinical trial evidence is comparatively sparse. The Chinese trial base remains the dominant evidence base, and the translation of those trials into Western practice has been limited by methodological heterogeneity, predominantly Chinese-language publication, and the regulatory non-pharmaceutical status of Schisandra extracts in the United States and Europe. The recent (2015-2024) literature includes a growing number of higher-quality Chinese trials in MAFLD/NAFLD with bilingual abstracts and improved methodology.
Bifendate (DDB) — The Synthetic Schisandrin C Derivative as a Chinese Pharmaceutical
The most striking translational outcome of the Schisandra liver research is the development of bifendate (dimethyl-4,4'-dimethoxy-5,6,5',6'-dimethylenedioxybiphenyl-2,2'-dicarboxylate — DDB), a synthetically modified schisandrin C analog that has been a registered pharmaceutical drug in the People's Republic of China since 1982. Bifendate was developed by Chinese medicinal chemists at the Institute of Materia Medica of the Chinese Academy of Medical Sciences as a structurally simplified, more bioavailable version of the natural schisandrin C scaffold. The synthesis removes one of the methylenedioxy bridges of the natural molecule and adds two methyl ester groups that improve oral absorption.
Bifendate is licensed in China for:
- Chronic hepatitis B and C with elevated transaminases
- Drug-induced hepatitis (most commonly from antituberculosis, antiepileptic, and chemotherapeutic drugs)
- Hepatic transaminase elevation of unspecified cause
The standard dose is 7.5-15 mg orally three times daily for 4-8 weeks initially, then a maintenance phase. Bifendate consistently normalizes elevated ALT within 4-8 weeks in 70-80% of patients with drug-induced or chronic-hepatitis-associated transaminitis. The mechanism is essentially the same as the parent schisandrin C: Nrf2 activation, glutathione upregulation, and mitochondrial stabilization, but with improved oral bioavailability and consistent pharmaceutical-grade dosing.
Bifendate is not approved by the U.S. Food and Drug Administration or the European Medicines Agency, where it has not been submitted for licensing, but it is part of standard hepatology practice in mainland China, Hong Kong, and Taiwan, and is sometimes encountered by Western physicians treating patients of East Asian background who self-source it. The drug is widely available and reasonably priced in Chinese pharmacies and provides an interesting case study in how botanical phytochemistry can directly generate a registered pharmaceutical drug.
CYP450 Induction — Mechanism and Clinical Interaction Risk
The clinically most important caution for Schisandra use is its potent induction of hepatic cytochrome P450 enzymes — particularly CYP3A4, the single enzyme responsible for metabolizing roughly 30% of all clinically used pharmaceutical drugs. Schisandrin B and schisantherin A activate the pregnane X receptor (PXR), a nuclear receptor that drives transcription of CYP3A4 and other phase I and phase II metabolizing enzymes. In human hepatocyte cultures, schisandrin B at clinically relevant concentrations produces 4- to 8-fold increases in CYP3A4 enzyme activity within 48-72 hours of exposure.
The clinical implication is that Schisandra supplementation can substantially accelerate the clearance and reduce the plasma concentration of co-administered CYP3A4 substrate drugs. Documented or strongly suspected clinically significant interactions include:
- Tacrolimus and cyclosporine — transplant immunosuppressants with narrow therapeutic windows. Case reports document organ-rejection episodes coincident with herbal product use containing Schisandra or related CYP3A4-inducing botanicals.
- Warfarin — bidirectional INR changes through CYP2C9 and CYP3A4 effects on R- and S-warfarin enantiomers.
- Direct oral anticoagulants (DOACs) — apixaban, rivaroxaban, and to a lesser extent dabigatran are partly CYP3A4 substrates, and reduced plasma levels could increase stroke risk in atrial fibrillation patients.
- Oral contraceptives — ethinyl estradiol and progestin levels reduced, with potential contraceptive failure.
- HIV antiretrovirals — many protease inhibitors and NNRTIs are CYP3A4 substrates with strict therapeutic-window requirements.
- Statins — simvastatin, lovastatin, and atorvastatin (more so than the non-CYP3A4 statins pravastatin or rosuvastatin) have reduced exposure.
- Anticancer agents — imatinib, sunitinib, erlotinib, and other tyrosine kinase inhibitors.
- Benzodiazepines — midazolam (the standard CYP3A4 phenotyping probe), triazolam, alprazolam.
- Calcium channel blockers — felodipine, amlodipine, nifedipine.
The interaction risk is highest with narrow-therapeutic-index drugs and with chronic Schisandra use. Brief or occasional use of dried berries in culinary preparations is unlikely to produce clinically meaningful interactions. Patients on any prescription medication should consult a pharmacist or physician before initiating chronic Schisandra supplementation.
Drug-Induced Liver Injury and Hepatotoxin Co-Exposure
One of the most clinically attractive applications of Schisandra is as an adjunct in drug-induced liver injury (DILI), particularly during antituberculosis therapy. Isoniazid, rifampicin, and pyrazinamide all carry meaningful hepatotoxicity risk, with clinically significant transaminase elevation in 10-20% of patients during standard 6-month combination therapy. Bifendate (the schisandrin C derivative) is routinely co-administered with antituberculosis regimens in Chinese practice and has been shown in trials to reduce transaminase elevation and reduce the need to interrupt TB therapy for hepatotoxicity. The parent extract Schisandra fruit similarly reduces transaminase elevation in patients receiving chronic chemotherapy (methotrexate, antiepileptics).
The mechanism is the same glutathione and Nrf2 upregulation discussed above — the liver tolerates the drug-induced electrophilic and oxidative stress better when its phase II conjugation capacity and antioxidant defense are augmented. The same principle has been applied to environmental hepatotoxin exposure (occupational solvents, ethanol abuse contexts), with smaller but generally favorable evidence.
One important caveat: the CYP3A4 induction effect can interact unpredictably with drug-metabolism pathways. If a drug is metabolized by CYP3A4 to a hepatotoxic metabolite (rather than detoxified by CYP3A4), Schisandra induction could theoretically increase hepatotoxic metabolite production. This has not been a major clinical issue but is a theoretical consideration in drug-DILI management.
Non-Alcoholic Fatty Liver Disease (NAFLD / MAFLD) Evidence
The recent (2015-2024) Schisandra literature has shifted increasingly toward non-alcoholic fatty liver disease (NAFLD), now reclassified as metabolic-dysfunction-associated fatty liver disease (MAFLD), reflecting the global epidemic of metabolic-syndrome-driven liver injury. Multiple Chinese and Korean trials have documented:
- Reduction in hepatic steatosis on ultrasound imaging
- Reduction in ALT and AST
- Improvement in HOMA-IR insulin sensitivity index
- Modest reduction in body weight and waist circumference
- Improvement in serum lipid profile (LDL down, HDL up modestly)
The mechanism in MAFLD likely combines the established hepatoprotective effects with secondary metabolic effects: AMP-activated protein kinase (AMPK) activation, peroxisome proliferator-activated receptor alpha (PPAR-alpha) modulation, and reduction of de novo lipogenesis. The schisandrin B effect on PPAR-alpha is particularly interesting because PPAR-alpha is the target of the fibrate class of lipid-lowering drugs.
Schisandra as a MAFLD adjunct is best considered in combination with the standard interventions of weight loss, exercise, and dietary modification. It is not a substitute for those interventions but appears to augment their effect, similar to how Milk Thistle (silymarin) has been used as a MAFLD adjunct for several decades.
Practical Dosing Protocols and Standardization
Practical Schisandra dosing for liver support varies substantially depending on the preparation. A few representative regimens drawn from clinical and traditional usage:
- Dried Schisandra berry — 1.5-6 grams per day in decoction (boiled tea), the traditional Chinese preparation. The fruit is added to water and simmered 15-30 minutes; the resulting astringent reddish-brown tea is consumed throughout the day. This is the lowest-potency preparation, best used for general support and as part of a broader herbal protocol.
- Schisandra tincture (1:5 in 50% ethanol) — 2-4 mL three times daily. Tinctures extract lignans more efficiently than water decoction and provide a more concentrated dose in a more convenient format.
- Standardized lignan extract — commercially available preparations are typically standardized to either 9% schisandrins or to a specified content of schisandrin B. Typical dose is 100-500 mg of standardized extract one to three times daily, providing roughly 9-100 mg of total lignans per day.
- Bifendate (DDB) pharmaceutical — Chinese practice — 7.5-15 mg three times daily for 4-8 weeks, then maintenance dose adjusted to liver function tests.
Standardization to lignan content (preferably with schisandrin B reported separately) is the single most important quality indicator for a commercial Schisandra product. Extracts that report only "Schisandra chinensis fruit, 500 mg" without lignan content are essentially uncharacterized in pharmacological terms. Reputable suppliers will provide either a certificate of analysis or list standardized content on the label.
Duration of use: traditional Chinese practice uses Schisandra in 6- to 12-week courses with breaks, not continuous indefinite use. There is no formal published evidence for or against indefinite continuous use, but the precautionary principle and the CYP450 interaction profile both argue for cycling rather than continuous chronic dosing in the absence of a specific clinical indication.
Cautions and Contraindications
- Drug interactions via CYP3A4 induction — as discussed in detail above, this is the dominant safety concern with Schisandra. Patients on any of the affected drug classes (immunosuppressants, anticoagulants, oral contraceptives, antiretrovirals, statins, anticancer agents, benzodiazepines, calcium channel blockers) should not initiate chronic Schisandra without pharmacist or physician consultation.
- Pregnancy and lactation — insufficient safety data in human pregnancy. Schisandra has documented uterine-stimulant effects in animal studies (it was traditionally used in late-pregnancy Chinese medicine to support labor) and should be avoided in early and mid-pregnancy. Avoid in lactation due to absence of pediatric safety data.
- Active peptic ulcer disease — Schisandra fruit is highly astringent and acidic, and case reports describe worsening of gastric ulcer pain. Caution in patients with active PUD or severe GERD.
- Epilepsy — one of the active lignans, schisandrin A, has CNS-stimulant properties at high doses and has been reported to lower seizure threshold in animal models. Avoid in poorly controlled epilepsy or use with caution and pharmacist consultation.
- Surgical procedures — discontinue Schisandra at least 2 weeks before any elective surgery, due to the CYP3A4 induction effect on anesthetics (particularly midazolam and fentanyl) and unpredictable effects on intraoperative drug pharmacokinetics.
- Acute hepatitis with markedly elevated transaminases (e.g., ALT > 10x upper limit) — acute hepatocellular necrosis is not the right setting for Schisandra; standard medical management is required first. Schisandra and bifendate are adjuncts for chronic hepatitis with moderate transaminitis, not rescue therapy for fulminant liver failure.
Key Research Papers
- Liu KT, Lesca P (1982). Pharmacological properties of dibenzo[a,c]cyclooctene derivatives isolated from Fructus Schizandrae chinensis. Chemico-Biological Interactions. — PubMed
- Chiu PY, Tang MH, Mak DH, et al. (2003). Hepatoprotective mechanism of schisandrin B: role of mitochondrial glutathione antioxidant status against oxidative stress. Free Radical Biology and Medicine 35(4):368-380. — PubMed
- Pan SY, Dong H, Zhao XY, et al. (2008). Schisandrin B from Schisandra chinensis reduces hepatic lipid contents in hypercholesterolaemic mice. Journal of Pharmacy and Pharmacology. — PubMed
- Panossian A, Wikman G (2008). Pharmacology of Schisandra chinensis Bail.: An overview of Russian research and uses in medicine. Journal of Ethnopharmacology 118(2):183-212. — PubMed
- Stacchiotti A, Li Volti G, Lavazza A, et al. (2009). Schisandrin B stimulates a cytoprotective response in rat liver. European Journal of Histochemistry. — PubMed
- Mocan A, Crisan G, Vlase L, et al. (2014). Comparative studies on polyphenolic composition, antioxidant and antimicrobial activities of Schisandra chinensis leaves and fruits. Molecules 19(9):15162-15179. — PubMed
- Cheng N, Ren N, Gao H, Lei X, Zheng J, Cao W (2013). Antioxidant and hepatoprotective effects of Schisandra chinensis pollen extract on CCl4-induced acute liver damage in mice. Food and Chemical Toxicology. — PubMed
- Park HJ, Lee SJ, Song Y, et al. (2014). Schisandra chinensis prevents alcohol-induced fatty liver disease in rats. Journal of Medicinal Food. — PubMed
- Liu HM, Yan X, Kikuchi T, Nakamura Y (1997). Inhibitory effect of bifendate on rat liver microsomal mixed function oxidase activities. Pharmacological Research. — PubMed
- Loo WT, Cheung MN, Chow LW (2007). The inhibitory effect of a herbal formula comprising ginseng and Schisandra chinensis on aromatase activity in vitro. Cancer Chemotherapy and Pharmacology. — PubMed
- Mou Q, Jiang H, Zhang C, et al. (2016). Schisandra chinensis lignans improve insulin resistance in NAFLD via AMPK and PPAR signaling pathways. Phytotherapy Research. — PubMed
- Wu MD, Cheng HC, Yuan GF, Ma YT (2014). Schisandra lignan extract protects rat liver from carbon tetrachloride-induced fibrosis. Journal of Ethnopharmacology. — PubMed
PubMed Topic Searches
- PubMed: Schisandra hepatoprotection
- PubMed: Schisandrin B / glutathione / Nrf2
- PubMed: Bifendate / DDB hepatitis trials
- PubMed: Schisandra CYP3A4 induction
- PubMed: Schisandra NAFLD/MAFLD
Connections
- Schisandra Overview
- Schisandra Benefits Hub
- Schisandra Adaptogenic Action
- Schisandra Cognitive Function
- Schisandra Endurance & Recovery
- Milk Thistle (Silymarin)
- Dandelion
- Glutathione
- N-Acetylcysteine (NAC)
- Hepatology
- Hepatitis
- Hepatitis B
- Liver Function Tests
- Liver Cleansing
- Detoxification