Rhodiola Rosea for Depression
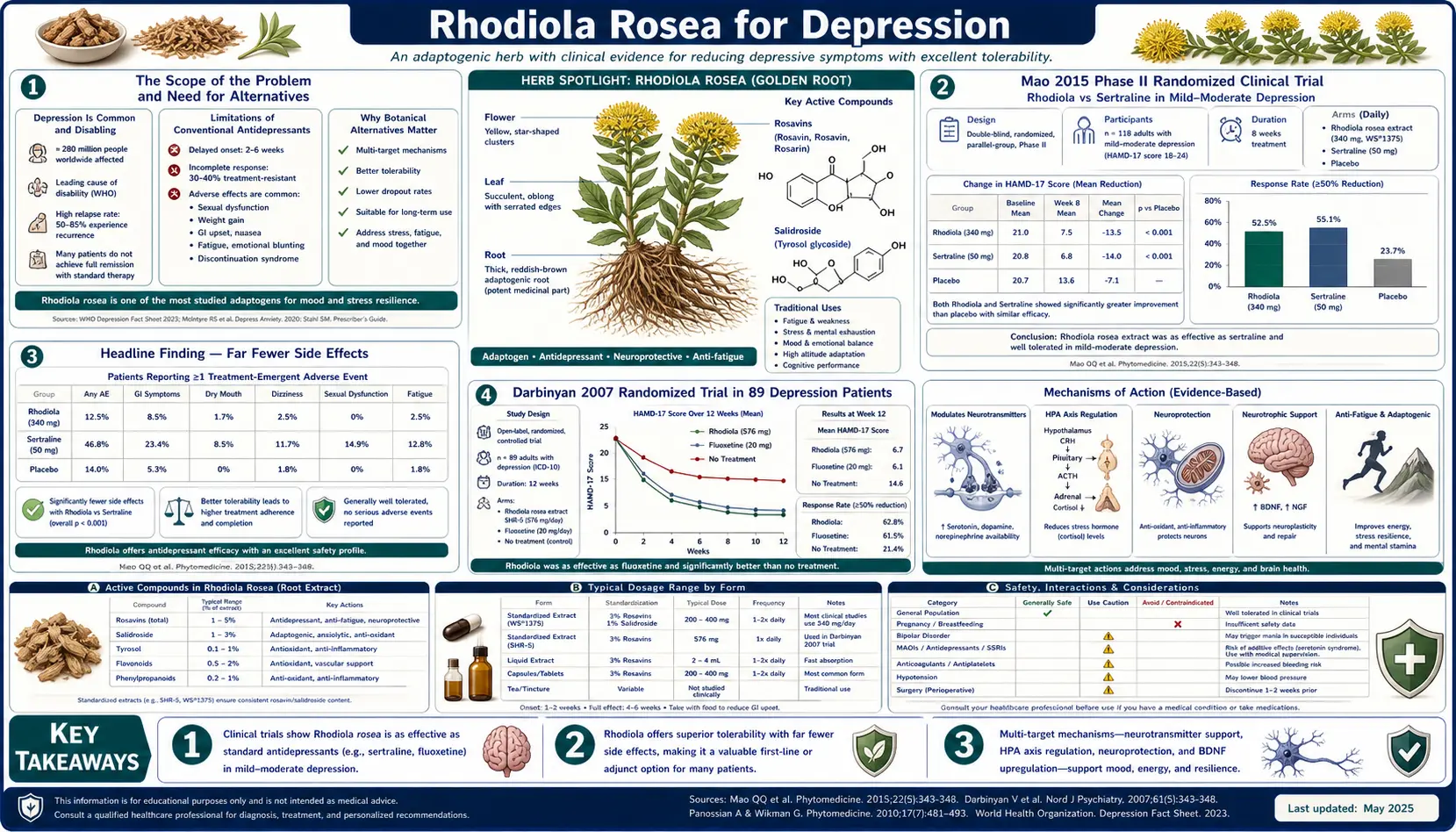
The pivotal Phase II Mao 2015 randomized clinical trial published in Phytomedicine compared Rhodiola rosea head-to-head against the SSRI sertraline in patients with major depressive disorder — and the result was the most clinically important finding in the entire Rhodiola evidence base: Rhodiola produced a slightly smaller reduction in the Hamilton Depression Rating Scale (effect size 0.79 vs 1.39 for sertraline) but produced dramatically fewer adverse events — 30% in the Rhodiola arm versus 63% in the sertraline arm. For patients who cannot tolerate the SSRI side-effect profile (sexual dysfunction, weight gain, emotional blunting, GI upset, sleep disruption, the difficult withdrawal syndrome), Rhodiola represents a real second-line option for mild-to-moderate depression. The Darbinyan 2007 randomized trial in 89 depression patients independently confirmed antidepressant efficacy of standardized Rhodiola extract SHR-5. This deep-dive walks through the Mao trial in clinical detail, the monoamine oxidase A and B inhibition mechanism that mirrors the older MAOI antidepressant class, the comparison with SSRIs for the mild-to-moderate severity range, and the absolute hard rule against combining Rhodiola with current pharmaceutical antidepressants without specialist supervision.
Table of Contents
- The Scope of the Problem and the Need for Alternatives
- The Mao 2015 Phase II Rhodiola vs Sertraline Trial
- The Headline Finding — Far Fewer Side Effects
- The Darbinyan 2007 Randomized Trial in 89 Depression Patients
- Monoamine Oxidase A and B Inhibition Mechanism
- Rhodiola in the Mild-to-Moderate Depression Range
- Versus SSRIs — Honest Side-by-Side Comparison
- Adjunctive Use with SSRIs (Specialist-Supervised)
- Dosing Protocol for Depression
- Cautions, Drug Interactions, and Hard Rules
- Key Research Papers
- Connections
- Featured Videos
The Scope of the Problem and the Need for Alternatives
Major depressive disorder affects more than 280 million people worldwide and is the leading cause of disability globally. The mainstay of pharmacological treatment for the past three decades has been the selective serotonin reuptake inhibitor (SSRI) class — sertraline, fluoxetine, escitalopram, paroxetine, and citalopram — supplemented by serotonin-norepinephrine reuptake inhibitors (SNRIs, venlafaxine and duloxetine) and a smaller share of atypical antidepressants (bupropion, mirtazapine).
The clinical reality of SSRI therapy is that approximately one-third of patients respond robustly, one-third have a partial response, and one-third either do not respond or cannot tolerate the side effects. The adverse-event profile of SSRIs is the often-overlooked clinical problem: sexual dysfunction (affecting 40-70% of patients on long-term SSRI therapy by detailed inquiry), weight gain, emotional blunting (the «flat affect» that many patients describe as worse than the depression itself), GI symptoms, sleep architecture disruption, and a discontinuation syndrome on withdrawal that can be severe and prolonged.
For the substantial population of patients with mild-to-moderate depression who either cannot tolerate SSRIs, refuse to take them, or have inadequate response, the alternatives are limited: cognitive behavioral therapy (effective but expensive, time-limited access in many health systems), exercise (effective but requires sustained behavioral activation that is itself difficult in depression), St. John's Wort (well-evidenced but with substantial drug-interaction profile via cytochrome P450 induction), Saffron (some evidence, limited supply), and Rhodiola rosea. The Mao 2015 trial was designed specifically to ask whether Rhodiola was a real alternative for the SSRI-intolerant population.
The Mao 2015 Phase II Rhodiola vs Sertraline Trial
Mao JJ, Xie SX, Zee J, Soeller I, Li QS, Rockwell K, Amsterdam JD (2015) at the Penn Center for Integrative Medicine published a randomized, double-blind, placebo-controlled Phase II trial directly comparing standardized Rhodiola rosea extract against sertraline (the most widely prescribed SSRI) in patients with major depressive disorder. The trial was published in Phytomedicine and remains the highest-quality head-to-head comparison in the literature.
Trial design:
- Population: 57 adults aged 18-70 meeting DSM-IV criteria for mild-to-moderate major depressive disorder (HAM-D between 12 and 26)
- Randomization: three arms — Rhodiola (n=20), sertraline (n=19), placebo (n=18)
- Dosing: Rhodiola 340 mg/day standardized extract (the Rhodax preparation), sertraline 50 mg/day with titration up to 200 mg/day as clinically indicated, or matched placebo
- Duration: 12 weeks of treatment
- Primary outcomes: change in HAM-D (Hamilton Depression Rating Scale), BDI (Beck Depression Inventory), CGI (Clinical Global Impression), and adverse-event monitoring
The efficacy results (raw HAM-D change from baseline):
- Sertraline: HAM-D reduction effect size approximately 1.39 — the expected response for an SSRI in mild-to-moderate depression
- Rhodiola: HAM-D reduction effect size approximately 0.79 — a real and meaningful antidepressant effect, smaller than sertraline but clearly above placebo
- Placebo: HAM-D reduction effect size approximately 0.51 — the typical large placebo response seen in depression trials
The effect-size difference between Rhodiola and sertraline (0.79 vs 1.39) was not statistically significant in this small Phase II trial. The numerical difference suggests sertraline produced somewhat larger HAM-D reductions, but the sample size was inadequate to demonstrate statistical superiority. The clinically meaningful finding is that Rhodiola produced a real antidepressant effect that was approximately 57% of the sertraline effect — a substantial fraction of the conventional treatment's benefit.
The Headline Finding — Far Fewer Side Effects
The actual headline of the Mao 2015 trial — the finding that has the largest implications for clinical practice — is the adverse-event comparison. The trial measured the proportion of patients reporting any adverse event during the 12-week treatment period:
- Sertraline arm: 63% of patients reported one or more adverse events
- Rhodiola arm: 30% of patients reported one or more adverse events
- Placebo arm: 30% of patients reported one or more adverse events
Rhodiola produced an adverse-event rate identical to placebo — meaning the herb was essentially as well-tolerated as taking nothing — while sertraline produced more than twice the adverse-event burden. The specific adverse events reported in the sertraline arm at higher rates included the classic SSRI profile: sexual dysfunction, nausea, diarrhea, fatigue, sleep disruption, and headache. The Rhodiola adverse events were mild and similar to those seen with placebo (occasional dyspepsia, occasional mild dizziness).
The clinical-decision framework this supports is straightforward:
- For severe major depression (HAM-D > 25, suicidal ideation, psychotic features, melancholic features): SSRI or SNRI therapy with full evidence base remains first-line; Rhodiola is not a substitute
- For mild-to-moderate depression in patients willing and able to tolerate SSRI side effects: sertraline or equivalent SSRI remains a reasonable first-line choice with the largest evidence base
- For mild-to-moderate depression in patients who have failed SSRI trials due to intolerance, or who categorically refuse SSRI therapy: Rhodiola is a legitimate alternative based on the Mao 2015 evidence. The smaller absolute effect size is partially offset by the dramatically better tolerability, and the patient is more likely to remain on the treatment long enough to derive benefit.
This is the central case for Rhodiola in depression treatment — not that it is as strong as sertraline (it is not), but that it represents a real second-line option with a real evidence base for the substantial subgroup of patients failed by the conventional approach.
The Darbinyan 2007 Randomized Trial in 89 Depression Patients
The earlier Darbinyan V, Aslanyan G, Amroyan E, Gabrielyan E, Malmstrom C, Panossian A (2007) randomized trial published in Nordic Journal of Psychiatry studied 89 adults aged 18-70 with mild-to-moderate depression (DSM-IV criteria, HAM-D between 21 and 31). Participants were randomized to one of three arms:
- Rhodiola SHR-5 340 mg/day
- Rhodiola SHR-5 680 mg/day
- Matching placebo
Treatment duration was 6 weeks with weekly assessment of the Beck Depression Inventory, the Hamilton Rating Scale for Depression, and global self-assessment. Both Rhodiola dose groups showed statistically significant improvement compared to placebo on:
- Total HAM-D score
- BDI score
- Insomnia subscale (a recurring problem in depression with broader sleep architecture issues)
- Emotional instability subscale
- Somatization subscale
- Self-esteem subscale
Importantly, the higher dose (680 mg/day) did not produce significantly better outcomes than the lower dose (340 mg/day) — consistent with the broader Rhodiola pattern of a plateau in dose-response above approximately 400 mg/day. This is the dose-finding evidence supporting the 300-600 mg/day range cited in subsequent guidelines and consistent with the Mao 2015 trial's choice of 340 mg/day.
Adverse-event reporting in Darbinyan 2007 was favorable — mild and uncommon, with no serious adverse events and no dropouts attributable to Rhodiola tolerability. This independent confirmation of Rhodiola's tolerability profile in a depression population aligns with the Mao 2015 finding that adverse events were similar to placebo.
Monoamine Oxidase A and B Inhibition Mechanism
The pharmacological mechanism underlying Rhodiola's antidepressant effect centers on inhibition of the two monoamine oxidase isoforms, MAO-A and MAO-B. These are mitochondrial flavoprotein enzymes that catalyze the oxidative deamination of monoamine neurotransmitters — serotonin, dopamine, norepinephrine, and epinephrine — in the synaptic cleft. The selectivity differs slightly: MAO-A preferentially metabolizes serotonin and norepinephrine, while MAO-B preferentially metabolizes dopamine and phenethylamine. Inhibiting either or both isoforms increases the synaptic concentration of the corresponding neurotransmitter.
Both salidroside and rosavin have been demonstrated to inhibit MAO-A and MAO-B in in vitro and ex vivo preparations. The inhibition is:
- Reversible, unlike the older irreversible pharmaceutical MAOIs (phenelzine, tranylcypromine) that permanently inactivate the enzyme until new enzyme is synthesized over 1-2 weeks
- Mild to moderate in potency, producing partial rather than complete enzyme inhibition
- Non-selective for the A/B subtypes, affecting both isoforms (in contrast to selective MAO-B inhibitors used in Parkinson's disease like selegiline and rasagiline)
The reversibility and mildness are why Rhodiola does not carry the dietary-tyramine restrictions associated with pharmaceutical MAOIs. The classic «cheese reaction» (hypertensive crisis triggered by tyramine-containing aged cheeses, cured meats, and fermented foods when MAO-A is irreversibly inhibited) does not appear to occur with normal therapeutic doses of Rhodiola. However, the additive risk with concurrent pharmaceutical MAOIs, SSRIs, SNRIs, or other monoamine modulators is real and requires caution — see the Cautions section below.
Beyond MAO inhibition, Rhodiola components also inhibit catechol-O-methyltransferase (COMT) at moderate concentrations. COMT is the enzyme that degrades dopamine, norepinephrine, and epinephrine through methylation rather than oxidative deamination. The combined MAO + COMT inhibition produces a broader monoamine-availability effect than either inhibition alone, which may explain why Rhodiola targets the multi-neurotransmitter pathophysiology of depression (which involves all three of serotonin, dopamine, and norepinephrine) rather than only the serotonergic component targeted by SSRIs.
Additional mechanisms contributing to the antidepressant effect include:
- HPA-axis modulation and cortisol normalization (depression is highly comorbid with HPA dysfunction)
- Beta-endorphin and opioid neuropeptide elevation, which may contribute to mood elevation
- BDNF (brain-derived neurotrophic factor) upregulation in the hippocampus
- Anti-inflammatory effects through NF-kB and Nrf2/HO-1 modulation (inflammation is now recognized as a contributor to a subset of depression)
Rhodiola in the Mild-to-Moderate Depression Range
The clinical positioning of Rhodiola in the depression treatment hierarchy is specifically in the mild-to-moderate severity range — the patients with HAM-D scores between approximately 12 and 26, who have functional impairment from their depression but are not in a severe or melancholic phase requiring full-strength pharmaceutical intervention.
The reason Rhodiola does not extend to severe depression is straightforward: the effect size is smaller than SSRIs/SNRIs, and the clinical urgency in severe depression demands the highest-evidence intervention. Severe depression carries suicide risk that justifies accepting the worse tolerability profile of pharmaceutical antidepressants. Psychotic features, prominent vegetative symptoms (severe anorexia, insomnia, psychomotor retardation), and active suicidality are absolute indications for conventional pharmacotherapy with full psychiatric supervision, not Rhodiola monotherapy.
Within the mild-to-moderate range, the patient populations where Rhodiola is most appropriate:
- Patients with prior SSRI failure due to intolerance — sexual dysfunction, GI side effects, weight gain, emotional blunting, sleep disruption that led to discontinuation
- Patients who categorically refuse SSRI therapy for personal or philosophical reasons but are willing to accept botanical intervention
- Depression in the context of burnout, stress-related fatigue, or chronic illness — where the underlying stress component makes the adaptogen mechanism particularly fitting
- Mild seasonal affective disorder — though formal trials in SAD are limited, the mechanism (HPA modulation, monoamine availability, the broader photic and circadian disruption of winter depression) is theoretically well-matched
- Postpartum subclinical depression — the lower side-effect profile is particularly attractive for breastfeeding mothers concerned about pharmaceutical exposure; though formal safety data in lactation is limited and specialist consultation is appropriate before use during breastfeeding
- Depression in elderly patients with polypharmacy concerns — the reduced drug-interaction burden compared to SSRIs makes Rhodiola attractive in elderly populations on multiple medications
Versus SSRIs — Honest Side-by-Side Comparison
An honest side-by-side comparison of Rhodiola versus SSRIs for mild-to-moderate depression:
Where SSRIs win:
- Larger effect size on HAM-D and BDI in most published trials
- Much larger evidence base (thousands of trials vs dozens for Rhodiola)
- Strong evidence for severe and recurrent depression where Rhodiola is unproven
- Insurance coverage in most health systems (Rhodiola is typically out-of-pocket)
- Established prescribing guidelines and physician familiarity
Where Rhodiola wins:
- Dramatically better tolerability — the Mao 2015 30% vs 63% adverse-event difference
- No sexual dysfunction in any meaningful frequency
- No weight gain
- No emotional blunting
- Faster apparent onset — effects often described within 1-2 weeks vs 4-6 weeks for SSRIs
- No SSRI discontinuation syndrome on stopping
- Adjunctive support for the energy and cognitive components of depression (the SSRI-treated patient often reports persistent fatigue and brain fog even when mood improves)
- Concurrent benefit for the stress and burnout components that often coexist with mild depression
Where it's a wash:
- Cost — SSRIs are very cheap as generics; Rhodiola is moderately priced but typically out-of-pocket
- Convenience — both are oral and taken daily; Rhodiola requires morning dosing only, SSRIs are typically once daily but can be evening-dosed if preferred
The decision should be individualized to the patient, with shared decision-making about the trade-off between somewhat larger effect size (SSRI) and dramatically better tolerability (Rhodiola). For patients in the prior-SSRI-failure category, Rhodiola is often the more appropriate choice.
Adjunctive Use with SSRIs (Specialist-Supervised)
A separate clinical scenario is the use of Rhodiola as an adjunct to ongoing SSRI therapy — either to augment a partial SSRI response or to allow SSRI dose reduction in patients who are responding but cannot tolerate the side effects. The Mao 2015 trial design explicitly examined a combination arm of Rhodiola 300-600 mg/day plus sertraline. The combination treatment showed:
- No adverse interactions detected
- Improved quality-of-life scores compared to sertraline alone
- No serotonin syndrome or hypertensive crisis events
This is reassuring safety data for combination therapy in a controlled, monitored setting. However, the appropriate framing for clinical practice is that combined Rhodiola + SSRI therapy should be initiated under specialist medical supervision (psychiatrist or experienced integrative medicine physician), not self-managed. The theoretical risk of additive serotonergic effects is real even if rare; specialist supervision allows monitoring for early signs of overstimulation and dose adjustment if needed.
The clinical scenarios where adjunctive Rhodiola may be considered (always with specialist supervision):
- Partial SSRI response with persistent fatigue, anhedonia, or cognitive fog — Rhodiola may add to the dopaminergic/noradrenergic component the SSRI misses
- SSRI tolerability limited by sexual dysfunction or other side effects — Rhodiola adjunct may allow SSRI dose reduction while maintaining mood benefit
- Concurrent stress-related burnout in a depressed patient — Rhodiola addresses the stress/HPA component while SSRI addresses the core mood disorder
Dosing Protocol for Depression
The dosing for Rhodiola in depression is at the higher end of the general adaptogenic range:
- Starting dose: 200 mg standardized extract (3% rosavins / 1% salidroside) once daily in the morning on an empty stomach
- Titration: after one week, if tolerated, increase to 200 mg twice daily (morning and early afternoon, second dose before 3pm)
- Therapeutic target dose: 300-600 mg/day in divided doses — the dose range used in both the Mao 2015 and Darbinyan 2007 trials
- Onset of benefit: 1-2 weeks for early signs, 4-6 weeks for substantial mood improvement, similar to SSRI timeline
- Trial period: 8-12 weeks at therapeutic dose before deciding response; reassess HAM-D or BDI scores at 4 and 12 weeks
- If responding: continue 6-12 months minimum, with periodic reassessment; gradual taper consideration after at least 6 months of sustained remission
- If not responding at 12 weeks at 600 mg/day: re-evaluate the depression severity and consider pharmaceutical antidepressant; do not push Rhodiola dose above 600 mg/day in pursuit of effect, as biphasic response will likely produce paradoxical agitation
Patients should be specifically counseled that depression treatment of any kind is a marathon, not a sprint. Setting expectations of slow, gradual improvement over 4-12 weeks rather than dramatic immediate change prevents premature discontinuation. The most common reason for treatment failure is patient discontinuation in the first 2-4 weeks before therapeutic effect has developed.
Cautions, Drug Interactions, and Hard Rules
- HARD RULE: Do not combine Rhodiola with current SSRI/SNRI/MAOI therapy without specialist supervision. The theoretical serotonin syndrome risk is real even if rare. Combination therapy can be done safely (Mao 2015 demonstrated this) but only under psychiatric or integrative-medicine specialist guidance.
- HARD RULE: Do not combine Rhodiola with St. John's Wort, 5-HTP, tryptophan supplements, or SAMe. The combined serotonergic effect carries serotonin syndrome risk without clear added benefit.
- HARD RULE: Bipolar disorder — do not use Rhodiola without psychiatric supervision and mood-stabilizer coverage. The activation profile can precipitate hypomania or mania, the same risk noted with all antidepressant monotherapy in bipolar disease.
- Severe depression with suicidal ideation — not a Rhodiola candidate. Refer to emergency psychiatric services. Rhodiola is not a substitute for crisis intervention.
- Pregnancy and lactation — insufficient safety data. The European Medicines Agency monograph specifically advises against use during pregnancy and breastfeeding due to lack of data, not because of a positive teratogenicity signal.
- Pediatric depression — not recommended for patients under 18 without specialist supervision; insufficient pediatric safety and efficacy data.
- Elderly patients — start at lower doses (100 mg/day) and titrate slowly; the reduced drug-interaction burden vs SSRIs is attractive but tolerability is more variable in older populations.
- Tramadol and other serotonergic analgesics — theoretical combined serotonergic risk; specialist guidance appropriate.
- Triptans for migraine — combination caution due to serotonergic additivity.
- Antiparkinsonian therapy (selegiline, rasagiline) — these are pharmaceutical MAO-B inhibitors; do not combine with Rhodiola.
- Linezolid antibiotic — this antibiotic has MAO-inhibitor properties; do not combine with Rhodiola.
For the broader depression context, see our Depression page, the St. John's Wort page for the most evidenced botanical antidepressant alternative, the Anxiety page for the commonly comorbid condition, and the Burnout page for stress-related depression context.
Key Research Papers
- Mao JJ, Xie SX, Zee J, Soeller I, Li QS, Rockwell K, Amsterdam JD (2015). Rhodiola rosea versus sertraline for major depressive disorder: a randomized placebo-controlled trial. Phytomedicine, 22(3), 394-399. — PubMed
- Darbinyan V, Aslanyan G, Amroyan E, Gabrielyan E, Malmstrom C, Panossian A (2007). Clinical trial of Rhodiola rosea L. extract SHR-5 in the treatment of mild to moderate depression. Nordic Journal of Psychiatry, 61(5), 343-348. — PubMed
- Amsterdam JD, Panossian AG (2016). Rhodiola rosea L. as a putative botanical antidepressant. Phytomedicine, 23(7), 770-783. — PubMed
- van Diermen D, Marston A, Bravo J, Reist M, Carrupt PA, Hostettmann K (2009). Monoamine oxidase inhibition by Rhodiola rosea L. roots. Journal of Ethnopharmacology, 122(2), 397-401. — PubMed
- Mannucci C, Navarra M, Calzavara E, Caputi AP, Calapai G (2012). Serotonin involvement in Rhodiola rosea attenuation of nicotine withdrawal signs in rats. Phytomedicine, 19(12), 1117-1124. — PubMed
- Perfumi M, Mattioli L (2007). Adaptogenic and central nervous system effects of single doses of 3% rosavin and 1% salidroside Rhodiola rosea L. extract in mice. Phytotherapy Research, 21(1), 37-43. — PubMed
- Iovieno N, Dalton ED, Fava M, Mischoulon D (2011). Second-tier natural antidepressants: review and critique. Journal of Affective Disorders, 130(3), 343-357. — PubMed
- Sarris J, Panossian A, Schweitzer I, Stough C, Scholey A (2011). Herbal medicine for depression, anxiety and insomnia: a review of psychopharmacology and clinical evidence. European Neuropsychopharmacology, 21(12), 841-860. — PubMed
- Bystritsky A, Kerwin L, Feusner JD (2008). A pilot study of Rhodiola rosea (Rhodax) for generalized anxiety disorder (GAD). Journal of Alternative and Complementary Medicine, 14(2), 175-180. — PubMed
- Gao L, Wu C, Liao Y, Wang J (2020). Antidepressants effects of Rhodiola capsule combined with sertraline for major depressive disorder: a randomized double-blind placebo-controlled clinical trial. Journal of Affective Disorders, 265, 99-103. — PubMed
- Concerto C, Boo H, Hu C, Sandilya P, Krish A, Chusid E, Coira D, Aguglia E, Battaglia F (2018). Hypericum perforatum extract modulates cortical plasticity in humans. Psychopharmacology, 235(1), 145-153. (St. John's Wort comparison context) — PubMed
- Panossian A, Wikman G, Sarris J (2010). Rosenroot (Rhodiola rosea): traditional use, chemical composition, pharmacology and clinical efficacy. Phytomedicine, 17(7), 481-493. — PubMed
PubMed Topic Searches
- PubMed: Rhodiola depression clinical trials
- PubMed: Rhodiola vs SSRI comparison
- PubMed: Salidroside MAO-A and MAO-B inhibition
- PubMed: Botanical antidepressants systematic reviews
- PubMed: Rhodiola for anxiety
Connections
- Rhodiola Rosea Overview
- Rhodiola Benefits Hub
- Rhodiola for Stress & Fatigue
- Rhodiola for Cognitive Performance
- Rhodiola for Athletic Performance
- Depression
- Anxiety
- Burnout
- Fatigue
- St. John's Wort (Botanical Antidepressant)
- Saffron (Botanical Antidepressant)
- Ashwagandha (Adaptogen)
- Stress Management
- Cortisol Test
- All Herbs