Gymnema for Sugar Cravings — The T1R2/T1R3 Sweet-Taste Blockade and Its Behavioral Applications
There is no other plant compound that produces the gymnemic acid effect: chew a fresh Gymnema sylvestre leaf or hold a gymnema lozenge in your mouth for one minute, then taste anything sweet — sugar in coffee, a piece of chocolate, fresh fruit, even artificial sweeteners like aspartame and sucralose — and you will perceive no sweetness at all. The food still has its other tastes (bitter, salty, sour, savory), but the entire sweetness channel is silenced for roughly 30-90 minutes. The molecular mechanism is selective competitive antagonism at the T1R2/T1R3 sweet-taste receptor heterodimer expressed on type II taste-bud cells. This curiosity has serious applications: it can be deployed as a willpower amplifier to interrupt sugar-craving episodes, has been extensively studied in the development of orexigenic-blocker drug candidates by major pharmaceutical companies, and provides a uniquely satisfying sensory demonstration to patients of how reflexive sugar consumption can be disrupted at the receptor level.
Table of Contents
- The Experience — What Sweet Tastes Like When the Receptor Is Blocked
- The T1R2/T1R3 Receptor and How Gymnemic Acids Block It
- Duration and Onset Kinetics
- Which Sweeteners Are Blocked (and Which Are Not)
- Behavioral Application — The Willpower Amplifier
- Sugar Addiction and the Reward-Circuit Framework
- Big Pharma History — Sweet-Receptor Antagonist Drug Programs
- Practical Preparations — Leaves, Lozenges, Tea
- Combining Tongue Application with Systemic Dosing
- Cautions and Edge Cases
- Key Research Papers
- Connections
- Featured Videos
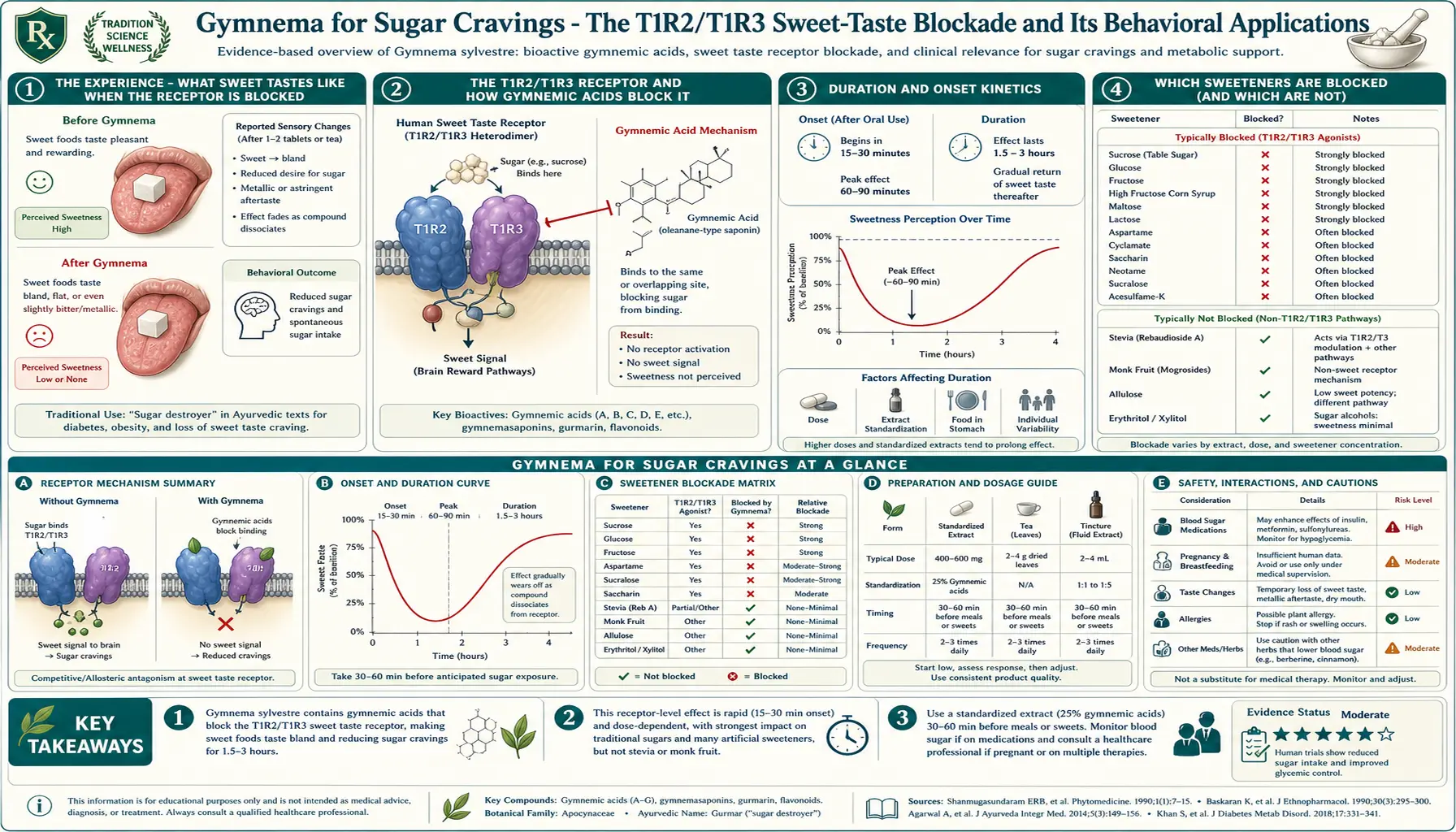
The Experience — What Sweet Tastes Like When the Receptor Is Blocked
The most informative way to understand gymnemic acid is to taste it work. The protocol takes 60 seconds and is harmless. Find a gymnema lozenge or 1-2 g of leaf powder; chew it or hold it in your mouth, distributing across the tongue, for one minute; spit out or swallow. Wait 60 seconds for residual gymnemic acid to bind. Then place a single granule of table sugar (or a small piece of chocolate, or a sip of orange juice) on your tongue.
The result is consistently startling. Sugar tastes like a coarse grain of sand — you perceive its texture, its slight cooling effect as it dissolves, perhaps a faint trace of mineral character, but no sweetness. None. Chocolate becomes a flat, bitter, fatty paste. Orange juice tastes like watered-down lemon juice with no sugar to balance the acidity. Fruit becomes vegetable-like — the apple still tastes "appley" in some non-sweet way but is no more pleasant than chewing on celery.
The bitter and salty receptors are unaffected, so coffee still tastes like coffee, beer still tastes like beer, and pickles still taste like pickles. The sour and savory (umami) channels are also untouched. Only sweet is blocked. Artificial sweeteners are blocked just as effectively as table sugar — aspartame, sucralose, stevia, monk fruit, all become flavorless. Sugar alcohols like erythritol and xylitol, which work through the same T1R2/T1R3 receptor, are similarly silenced.
The blockade lasts approximately 30-90 minutes depending on the dose, after which sweetness perception returns to normal — usually starting with a returning awareness of intensely sweet stimuli (sugar in solution) and gradually broadening back to subtle sweetness (mild fruit).
For most people, the single experience of this effect provides a more visceral understanding of how reflexive sugar consumption is than any amount of reading about it. Sugar tastes good. When sugar does not taste good, the craving evaporates almost immediately. This is the basis of the behavioral application discussed below.
The T1R2/T1R3 Receptor and How Gymnemic Acids Block It
The molecular machinery of sweet-taste perception was characterized in the early 2000s. The sweet-taste receptor is a heterodimer of two G-protein-coupled receptors: T1R2 (encoded by the TAS1R2 gene) and T1R3 (encoded by TAS1R3). Both subunits must be expressed for sweet taste to function. T1R3 also dimerizes with T1R1 to form the umami (savory) receptor, but the T1R2-containing dimer is exclusively sweet-specific.
The T1R2/T1R3 receptor sits on the surface membrane of type II taste-bud cells, which are clustered in the fungiform papillae on the front of the tongue, the foliate papillae on the sides, and the circumvallate papillae at the back. Binding of a sweetener to either subunit triggers G-protein-coupled signaling through the gustducin pathway, leading to depolarization of the type II cell, release of ATP as a neurotransmitter onto the gustatory nerve fibers, and central perception of sweetness.
The receptor has an unusually large binding pocket that accommodates a remarkable variety of ligand structures: simple sugars (glucose, fructose, sucrose), sugar alcohols (sorbitol, mannitol, xylitol, erythritol), amino acids (glycine, alanine, in mild sweetness), sweet proteins (thaumatin, brazzein, monellin — some of the most intensely sweet substances known), and dozens of synthetic non-caloric sweeteners (saccharin, aspartame, acesulfame K, sucralose, neotame, advantame, steviol glycosides, mogrosides from monk fruit). All of these activate signaling by binding the same receptor complex.
Gymnemic acids are competitive antagonists at the T1R2/T1R3 receptor. Their triterpene saponin structure includes a sugar-like region (the glycoside moiety) that allows them to occupy part of the ligand-binding pocket, while their hydrophobic triterpene aglycone backbone provides binding affinity and orientation. They occupy the pocket without triggering the conformational change required for G-protein activation — the classical definition of a competitive antagonist. While bound, they physically prevent genuine sweeteners from accessing the binding site.
The binding is not covalent — gymnemic acids slowly dissociate from the receptor over the 30-90 minute window, and as they wash off, sweetness perception returns. The duration is determined by the dissociation rate constant and the saliva-mediated washout from the receptor environment.
The specificity for sweet over other taste modalities reflects the fact that bitter, salty, sour, and umami all use entirely different molecular machinery (the bitter receptors are a separate family of approximately 25 T2R G-protein-coupled receptors; salt and sour involve ion channels; umami uses the T1R1/T1R3 heterodimer). Gymnemic acids do not bind any of these, so non-sweet tastes are entirely preserved.
Duration and Onset Kinetics
The pharmacokinetics of the topical taste-blocking effect:
- Onset — full blockade develops within 30-60 seconds of gymnemic acid contact with the tongue. The effect is essentially instantaneous after the receptor saturation occurs.
- Peak effect — immediate and maximal within the first 5-10 minutes
- Decay — the partial return of sweetness perception begins at approximately 20-30 minutes for low doses (a few mg of gymnemic acid) and 45-60 minutes for higher doses (100-200 mg of gymnemic acid as in a standardized lozenge)
- Complete recovery — full restoration of normal sweet-taste perception at 60-120 minutes
- Tachyphylaxis (tolerance) — minimal. Repeated daily use does not appreciably reduce the per-use effect duration or intensity. The receptor is not internalized in response to chronic antagonist exposure, unlike many other GPCRs.
The most reliable way to extend the effect for a known temptation window (a long dinner with desserts, a holiday party with cake) is to redose at the 30-45 minute mark with a second lozenge or chewed leaf rather than to take a larger single dose at the outset. The blockade is dose-dependent in intensity (a larger single dose can produce a more complete and longer-lasting blockade) but the practical ceiling is around the dose of one full standardized lozenge; doubling beyond that produces minimal incremental benefit.
Which Sweeteners Are Blocked (and Which Are Not)
Effectively blocked (all activate T1R2/T1R3):
- Caloric sugars — sucrose (table sugar), glucose, fructose, lactose, maltose
- Sugar alcohols — sorbitol, mannitol, xylitol, erythritol, isomalt
- Synthetic non-caloric sweeteners — saccharin, aspartame, acesulfame potassium, sucralose, neotame, advantame
- Plant-derived non-caloric sweeteners — stevia (steviol glycosides), monk fruit (mogrosides), thaumatin
- Naturally sweet amino acids — glycine, D-alanine
- Sweet proteins — brazzein, monellin, miraculin
Not blocked (do not act primarily through T1R2/T1R3):
- The miraculin effect itself — miraculin from miracle berry converts sourness to sweetness through a separate mechanism and is partially affected but not abolished
- Sweet sensations not mediated by T1R2/T1R3 — certain glycosides that activate the receptor through different binding modes may show partial preservation
- The "perceived sweetness" of foods with strong umami — some foods that are described as sweet partly through umami pathway interactions retain some pleasurable character
Other taste modalities are entirely preserved:
- Bitter — T2R family receptors, unaffected. Coffee tastes like coffee, dark chocolate tastes like bitter chocolate, beer tastes like beer.
- Salty — ion channels (ENaC), unaffected. Crisps, pretzels, soy sauce, all unchanged.
- Sour — ion channel mediated, unaffected. Lemon, vinegar, fermented foods unchanged.
- Umami — T1R1/T1R3, unaffected. Mushrooms, parmesan, broths, glutamate-containing foods unchanged.
- Pungent/spicy — TRPV1 and related channels, unaffected. Chili, ginger, mustard unchanged.
- Cool/menthol — TRPM8, unaffected. Mint chewing gum still tastes minty (though if it's a sweetened gum, the sweet component will be absent).
The result is that during gymnemic acid blockade, foods become more "naked" in their non-sweet character. A piece of milk chocolate becomes a bitter waxy fat. A piece of fruit becomes a fibrous source of organic acids. A glass of orange juice becomes acidic dishwater. This is precisely why the effect is so behaviorally useful: the foods that you might otherwise overconsume due to their sweetness become genuinely unappealing, not because of a willpower override but because the brain is simply not receiving the reward signal.
Behavioral Application — The Willpower Amplifier
The most practical use of the taste-blockade is what behavioral nutritionists call the "willpower amplifier" approach. The protocol is simple:
- Identify the temptation moments — the predictable times of day or social situations when sugar consumption tends to derail a dietary plan. Common patterns: the 3 PM office afternoon slump and the candy bowl, the post-dinner dessert craving, the office cake at colleagues' birthdays, the dessert menu after restaurant dinners, the children's leftover Halloween candy.
- Pre-empt with a gymnema dose 5-15 minutes before exposure — chew a leaf, dissolve a lozenge, or take a 1-2 g leaf-powder dose in the mouth and hold it for a minute
- Encounter the temptation — the foods are still physically present, but they now taste flat and unappealing rather than reward-triggering. The decision to skip them becomes trivial rather than effortful.
- Wait out the temptation window — the 30-90 minute blockade is typically long enough to ride past the acute craving phase. Once the moment has passed, the craving for that specific food typically does not return that day.
The mechanism works because most non-clinical sugar cravings are reward-driven rather than nutritional. The brain's dopaminergic reward circuit (ventral tegmental area, nucleus accumbens) is strongly activated by sweetness signals from the tongue, and this activation drives the conscious experience of "craving" and the motor program of reaching for the food. When the sweetness signal does not arrive (because the receptor is blocked), the reward circuit gets no payoff for sugar consumption, and the behavior naturally extinguishes within the blockade window.
Long-term, repeated use of this approach can produce conditioning effects. If gymnema blockade is consistently deployed at the 3 PM office candy bowl over several weeks, the associative learning that "reaching for office candy now produces no reward" can erode the habit even without the herb — the candy bowl stops being a salient stimulus. This is a real behavioral mechanism, not magic, and is consistent with the general principles of cue-extinction in addiction research.
Sugar Addiction and the Reward-Circuit Framework
The framing of "sugar addiction" is contested in the academic literature — some researchers argue that sugar consumption meets formal addiction criteria (tolerance, withdrawal, compulsive use despite consequences, neuroadaptation in reward circuits), while others argue that the parallels to substances of abuse like alcohol or opioids are oversold and the phenomenology is better characterized as habit-driven hedonic consumption rather than true addiction.
For practical purposes, the distinction matters less than the observation that for some individuals, sugar consumption shows compulsive features: an inability to consume "just one cookie," a sustained pattern of consuming more than intended, return-to-baseline weight gain after diet attempts, and significant distress at the prospect of permanent abstinence. These patterns are particularly visible in patients with binge eating disorder, with reactive hypoglycemia, and with depressive disorders where sugar is being used as a self-medication strategy.
For these subgroups, gymnema provides a unique tool. Unlike most behavioral interventions (which require sustained conscious effort to deploy), gymnema works on the receptor level — the patient takes the lozenge, the receptor is blocked, the trigger food no longer tastes good, and the consumption decision becomes structurally different. This is closer to the model of pharmacological addiction treatments (naltrexone for opioid use disorder, disulfiram for alcohol use disorder) than to most "willpower" interventions.
Clinical experience suggests gymnema is most useful for sugar-craving patients during the first 2-8 weeks of a dietary change, when willpower reserves are most challenged. After the initial habituation period, many patients can taper off active gymnema use as their cravings naturally diminish on lower-carbohydrate intake.
For the broader framing of metabolic and behavioral approaches to weight loss, see our Weight Loss deep-dive.
Big Pharma History — Sweet-Receptor Antagonist Drug Programs
The pharmaceutical industry has periodically explored sweet-receptor antagonists as candidate anti-obesity drugs, with gymnemic acids serving as both an inspiration and a chemical starting point. The logic: if dietary sugar overconsumption drives obesity, and if a molecule could selectively block sweet-taste perception (rendering sugars unappealing without affecting the overall food experience), patients might naturally reduce sugar intake and lose weight without the conscious effort of dietary restriction.
The programs that have been publicly described:
- Lactisole — a non-gymnemic acid sweet-receptor antagonist, originally discovered in coffee and developed as a food-industry sweetness-modulating ingredient (used at low doses to suppress unwanted sweetness in formulations). Has been studied as a research tool for sweet-receptor pharmacology but never advanced to clinical use for obesity.
- The Senomyx / Coca-Cola partnership — in the early 2000s, the biotechnology company Senomyx developed sweetness enhancers (which lower the required sugar dose for a target perceived sweetness) and sweetness modulators including potential antagonists. Most of the clinical-grade work in this area was directed at sweetness enhancement (allowing food manufacturers to reduce sugar content without taste loss) rather than blockade.
- Various Big Pharma orexigenic-blocker programs — through the 2000s and 2010s, several major pharmaceutical companies explored sweet-receptor antagonists as candidate appetite suppressants. None have advanced to FDA approval. The general challenges have included: poor oral bioavailability of compounds that work topically on the tongue, the difficulty of designing a molecule that blocks taste receptors but does not also block the same receptors expressed in the gut (where sweet-taste signaling regulates GLP-1 secretion and other endocrine functions), and the conceptual problem that food-reward pathways involve multiple parallel inputs beyond sweetness alone.
- The arrival of GLP-1 agonists (semaglutide, tirzepatide) in the 2020s has substantially reduced the perceived market opportunity for sweet-receptor antagonists, since the GLP-1 class produces large weight losses (15-20% body weight) through a completely different mechanism and has demonstrated commercial viability.
The pharmaceutical interest has not resulted in marketed drugs, but the academic research generated by these programs has substantially clarified our understanding of how sweet-taste receptors work — including the detailed structural mapping of the T1R2/T1R3 receptor and the development of selective small-molecule antagonists used as research tools. Gymnemic acids remain the prototypical natural-product example and the only widely available sweet-receptor blocker in over-the-counter form.
Practical Preparations — Leaves, Lozenges, Tea
For the topical taste-blocking effect (as opposed to the systemic glycemic effect), several preparations work:
- Fresh or dried whole leaves — the most traditional preparation. Chew one or two small leaves (approximately 1-2 g of leaf material) for 60 seconds, distributing across the tongue, then spit out or swallow. The leaves have a mildly bitter, vegetal taste that some find unpleasant. Fresh leaves are nearly impossible to obtain in the West; dried leaves can be sourced from Ayurvedic herb suppliers.
- Chewable lozenges (gymnema sucrosa / gymnema chews) — the most convenient and widely available form. Several manufacturers produce standardized lozenges containing 50-200 mg of standardized gymnema extract (25% gymnemic acids), often in a slightly minty base to mask the herbal flavor. Hold in the mouth for 1-2 minutes, then chew or swallow.
- Standardized extract powder — a heaping pinch (approximately 200-500 mg) placed under the tongue and held for 60-90 seconds. Effective but less convenient than lozenges.
- Gymnema tea — brewed from dried leaves at approximately 1-2 g per cup for 10 minutes. The hot tea contacts the tongue and produces the taste-blocking effect, but the dilute concentration limits intensity compared to direct leaf or extract application. Useful as a pleasant gentle pre-meal beverage.
- Tinctures — less effective than direct leaf or extract application because the alcohol vehicle washes off the tongue quickly, limiting contact time. Generally not recommended for the topical effect.
Cost considerations: a 30-day supply of chewable lozenges typically runs $15-25 USD, which is affordable for daily use through a difficult dietary transition. Standardized extract capsules used for the systemic glycemic effect can be opened and the powder used sublingually if the user wants both effects from a single product.
Combining Tongue Application with Systemic Dosing
The two clinical applications of gymnema — the topical taste-blockade and the systemic glycemic effect — can be combined without conflict. A typical protocol for a patient with type 2 diabetes who also struggles with sugar cravings:
- Twice daily — standardized GS4 extract 400 mg with breakfast and dinner, swallowed as a capsule, for the systemic glycemic effect (see the Blood Sugar deep-dive for the full dosing rationale)
- As needed — a gymnema chewable lozenge held in the mouth 5-15 minutes before any expected sugar-craving moment, for the topical taste-blockade
The systemic capsule does not produce the topical taste effect (it passes through the mouth too quickly and in the wrong vehicle), so the lozenge component is genuinely additive. The total daily gymnemic acid exposure remains well below safety thresholds even with frequent topical use, because the topical doses are small.
One important caveat: each topical dose contributes a small additional systemic absorption of gymnemic acid through the oral mucosa and (if swallowed) through the GI tract. For patients on insulin or sulfonylureas, frequent topical use should be counted toward total daily gymnema exposure when adjusting medication doses (see the hypoglycemia cautions in the Blood Sugar deep-dive).
Cautions and Edge Cases
- Hypoglycemia risk in patients on insulin or sulfonylureas — even topical gymnemic acid use contributes some systemic absorption. Patients on glucose-lowering medications should follow the full hypoglycemia-monitoring protocol described in the Blood Sugar deep-dive.
- Pregnancy and lactation — insufficient safety data. Avoid even occasional use.
- Persistent taste disturbance — very rare reports of taste alteration lasting beyond the expected 60-120 minute window. Usually resolves within 24 hours; persistent dysgeusia beyond that warrants medical evaluation.
- Inadvertent dietary effects — some patients report unintentionally reduced food enjoyment for foods they had not intended to reduce (such as fruit or whole grains). The blockade is non-selective for sweetness source. Time the lozenge dose carefully to align with the temptation window rather than spanning a healthy meal.
- Effect on the social experience of food — using gymnema at a birthday party or family dinner where dessert is offered may produce awkward social moments if the host has prepared something they hoped you would enjoy. Polite social calibration is needed.
- Eating disorders — for patients with anorexia nervosa or restrictive eating disorders, gymnema is generally contraindicated because it can reinforce avoidance patterns rather than addressing the underlying disorder. For binge eating disorder, careful use under therapy supervision can be appropriate.
- Children — insufficient safety data; not recommended.
- Drug interactions — theoretical interaction with any medication absorbed through buccal mucosa, though clinically reported interactions are minimal.
Key Research Papers
- Imoto T et al. (1991). A novel peptide isolated from the leaves of Gymnema sylvestre — I. Characterization and its suppressive effect on the neural responses to sweet taste stimuli in the rat. Comparative Biochemistry and Physiology. Identified gurmarin as a second sweet-suppressing principle. — PubMed
- Sigoillot M et al. (2012). Sweet-taste-suppressing compounds: current knowledge and perspectives of application. Applied Microbiology and Biotechnology. Comprehensive review of gymnemic acids and other sweet-receptor antagonists. — PubMed
- Hellfritsch C et al. (2012). Human psychometric and taste receptor responses to steviol glycosides. Journal of Agricultural and Food Chemistry. Provides the T1R2/T1R3 mechanistic framework used to interpret gymnemic acid antagonism. — PubMed
- Suttisri R et al. (1995). Plant-derived triterpenoid sweetness inhibitors. Journal of Ethnopharmacology. Classification of gymnema-related saponins. — PubMed
- Brouwer J et al. (1983). The effect of gymnemic acid on the perception of sweetness. Chemical Senses. Early psychophysical characterization. — PubMed
- Kurihara Y (1992). Characteristics of antisweet substances, sweet proteins, and sweetness-inducing proteins. Critical Reviews in Food Science and Nutrition. Classic review covering gymnemic acids alongside other taste modulators. — PubMed
- Liu H et al. (2009). Gymnema sylvestre as a potential therapeutic approach for diabetes mellitus. Phytotherapy Research. Includes taste-receptor mechanism in broader pharmacology review. — PubMed
- Ye W et al. (2001). Sugar inhibitors from Gymnema sylvestre: comparative study and structure-activity relationships. Journal of Asian Natural Products Research. Structural analysis of gymnemic acid family. — PubMed
- Nelson G et al. (2001). Mammalian sweet taste receptors. Cell. The foundational paper identifying T1R2/T1R3 as the mammalian sweet-taste receptor. — PubMed
- Margolskee RF (2002). Molecular mechanisms of bitter and sweet taste transduction. Journal of Biological Chemistry. Reviews the gustducin signaling cascade that gymnemic acids interrupt. — PubMed
- Sanematsu K et al. (2014). Molecular mechanisms for sweet-suppressing effect of gymnemic acids. Journal of Biological Chemistry. Detailed structural and mutational analysis of the gymnemic acid binding site on T1R2/T1R3. — PubMed
- Hellekant G et al. (1985). Sweet taste suppressors and the human sweet taste receptor. Acta Physiologica Scandinavica. Cross-species comparison of gymnemic acid effects. — PubMed
PubMed Topic Searches
- PubMed: gymnemic acid sweet-taste receptor
- PubMed: T1R2/T1R3 sweet receptor antagonist
- PubMed: sugar craving sweet-taste blockade
- PubMed: gymnema behavioral sugar addiction
- PubMed: gurmarin sweet-suppressing protein
Connections
- Gymnema Overview
- Gymnema Benefits Hub
- Gymnema for Blood Sugar
- Gymnema for Weight Loss
- Gymnema for Cholesterol
- Artificial Sweeteners
- Refined Sugar
- Elimination Diet
- Blood Sugar Control
- Obesity
- Diabetes
- Berberine
- Cinnamon
- Fasting
- Chromium